Loading...
Abdominal Aortic Aneurysm (Ruptured)
Ruptured AAA is a catastrophic vascular emergency with an overall mortality of 80–90%, with most patients dying before reaching the hospital. [1][1] Among those who arrive alive, approximately 50%…
Dr. Lucas Mastropaolo
Ruptured AAA is a catastrophic vascular emergency with an overall mortality of 80–90%, with most patients dying before reaching the hospital. [1][1] Among those who arrive alive, approximately 50% do not survive surgical repair. [2] Misdiagnosis occurs in up to 30–42% of cases, most commonly confused with renal colic, diverticulitis, and myocardial infarction. [3-5]
1. History
- Classic triad (present in only ~one-third of cases): sudden abdominal/back pain, pulsatile abdominal mass, and hypotension [6-7]
- Abrupt onset of severe abdominal or back/flank pain, often radiating to the groin or scrotum [2][8]
- Pain is typically maximal at onset ("thunderclap" quality), constant, and unrelenting
- Syncope or near-syncope (pooled sensitivity only 27.8%) [9]
- Lower extremity weakness, numbness, or sudden inability to walk [10]
- Ask about known AAA, prior vascular imaging, or prior vascular surgery
- Timing: symptoms may be biphasic — an initial contained leak followed by free rupture within hours [8]
- Important negatives: absence of classic symptoms does NOT rule out rAAA; classic symptoms have poor sensitivity (abdominal pain 61.7%, back pain 53.6%, hypotension 30.9%) [9]
2. Alarm Features
- Hemodynamic instability or frank shock
- Sudden-onset severe abdominal or back pain in a patient >60 years with vascular risk factors
- Syncope with abdominal/back pain
- New lower extremity weakness, mottling, or pulse loss
- Grey Turner sign (flank ecchymosis) or Cullen sign (periumbilical ecchymosis) [2]
- Tearing sensation radiating to the back [10]
- Abdominal distension with rigidity
- Any patient with a known AAA presenting with new pain warrants immediate evaluation for rupture [1]
3. Medications
- Permissive hypotension strategy: target SBP 50–100 mmHg until surgical control is achieved; avoid aggressive fluid resuscitation to prevent clot disruption and the "lethal triad" of hypothermia, acidemia, and coagulopathy [1][11]
- Avoid raising blood pressure to normotensive levels prior to aortic control — this can dislodge retroperitoneal tamponade and precipitate free rupture [7]
- Massive transfusion protocol: balanced ratio of pRBCs, FFP, and platelets (1:1:1 approach)
- Pain control with IV opioids (fentanyl preferred for hemodynamic stability)
- Anticoagulants and antiplatelets should be noted and reversed as appropriate (warfarin → 4-factor PCC; DOACs → specific reversal agents)
- Avoid NSAIDs (renal perfusion concerns in shock)
- Postoperatively: beta-blockers and antihypertensives for long-term aortic wall stress reduction [1]
4. Diet
- NPO immediately upon suspicion — emergent surgical intervention is anticipated
- No specific dietary triggers for rupture
- Long-term: heart-healthy diet for cardiovascular risk reduction; smoking cessation is the single most impactful lifestyle modification [2]
5. Review of Systems
- Cardiovascular: chest pain, palpitations, syncope, prior claudication
- GI: nausea/vomiting, hematemesis, melena (aortoenteric fistula), abdominal distension
- GU: hematuria, oliguria/anuria (renal malperfusion), flank pain mimicking renal colic
- Neurologic: lower extremity weakness or paralysis (spinal cord ischemia), paresthesias
- Vascular: cold/pale/pulseless extremities, livedo reticularis [10]
- Constitutional: diaphoresis, lightheadedness, sense of impending doom
6. Collateral History and Family History
- Known AAA: prior imaging, size, surveillance history, and whether repair was previously discussed
- Family history of AAA (10–25% of AAA patients have a first-degree relative with the condition) [1][1]
- Family history of connective tissue disorders (Marfan, Ehlers-Danlos, Loeys-Dietz)
- Family history of sudden death or aortic dissection
- Smoking history from family members if patient unable to provide history
- Advance directives and surgical candidacy discussions (critical given high mortality)
7. Risk Factors
- Strongest risk factors for AAA: smoking history, older age (>65), male sex, family history of AAA, atherosclerotic cardiovascular disease [1]
- Additional risk factors: hypertension, hyperlipidemia, White race, inherited connective tissue disorders [1]
- Risk factors specifically for rupture: large aneurysm diameter (especially >5.5 cm), female sex (rupture at smaller diameters — mean 5.0 cm vs 6.0 cm in men), rapid expansion (>1 cm/year), continued smoking, uncontrolled hypertension, COPD [1][11]
- Peripheral artery disease and coronary artery disease are independent predictors of rupture [12]
8. Differential Diagnosis
The most common misdiagnoses are renal colic and myocardial infarction. [3-4] Key differentials:
- Renal colic/ureteral stone — colicky flank pain, hematuria; distinguish by bedside ultrasound showing AAA
- Acute myocardial infarction — chest/epigastric pain, ECG changes, troponin elevation; rAAA can cause troponin elevation from shock [13]
- Acute mesenteric ischemia — abdominal pain out of proportion to exam, lactic acidosis
- Perforated viscus — peritonitis, free air on imaging
- Acute pancreatitis — epigastric pain radiating to back, elevated lipase
- Diverticulitis — LLQ pain, fever; CT distinguishes
- Aortic dissection — tearing pain, blood pressure differential between arms
- GI hemorrhage — hematemesis/melena; consider aortoenteric fistula in patients with prior aortic graft [8]
- Retroperitoneal hemorrhage (other causes) — anticoagulation, trauma
- Spinal pathology — acute disc herniation, epidural abscess
Pearl: In any patient >50 years with sudden abdominal/back pain and hemodynamic instability, rAAA must be excluded before pursuing other diagnoses. [4-5]
9. Past Medical History
- Known AAA — size, growth rate, prior surveillance imaging
- Prior aortic or vascular surgery (risk of anastomotic pseudoaneurysm, aortoenteric fistula)
- Peripheral artery disease, coronary artery disease, cerebrovascular disease
- COPD (associated with both AAA development and rupture risk)
- Hypertension, hyperlipidemia
- Connective tissue disorders
- Chronic kidney disease (impacts contrast use and surgical risk)
- Anticoagulant/antiplatelet use
10. Physical Exam
- Vital signs: hypotension (may be absent initially in contained rupture), tachycardia, tachypnea; narrow pulse pressure
- Abdominal exam: pulsatile abdominal mass (sensitivity only 47.1%; decreased in obesity); tenderness, distension, rigidity [2][9]
- Vascular exam: diminished or absent femoral/pedal pulses, asymmetric blood pressures in extremities, cool/mottled lower extremities, livedo reticularis [10]
- Skin: Grey Turner sign (flank ecchymosis), Cullen sign (periumbilical ecchymosis) — late findings [2]
- Neurologic: lower extremity motor/sensory deficits (spinal cord ischemia from intercostal artery compromise)
- Rectal exam: may reveal blood if aortoenteric fistula present
- Pearl: Abdominal palpation does NOT increase the risk of rupture [2]
11. Lab Studies
- Type and crossmatch — immediate, at least 6–10 units pRBCs
- CBC — baseline hemoglobin/hematocrit (may be initially normal due to acute blood loss before equilibration)
- BMP/CMP — renal function (baseline and for contrast planning), electrolytes
- Coagulation studies — PT/INR, PTT, fibrinogen (guide massive transfusion)
- Lactate — marker of tissue hypoperfusion and shock severity
- ABG — assess for metabolic acidosis
- Troponin — elevated in ~55% of post-repair patients; associated with increased mortality (OR 4.23 for in-hospital death) [13]
- D-dimer — may be elevated but nonspecific; useful in ruling out AAS in low-probability patients [1]
- Thromboelastography (TEG/ROTEM) — if available, guides targeted blood product resuscitation
12. Imaging
- Point-of-care ultrasound (PoCUS): first-line bedside test; sensitivity 97.8%, specificity 97.0% for detecting AAA in suspected rAAA (cannot detect rupture itself, but identifies the aneurysm and guides urgent transfer) [9]
- CT angiography (CTA): gold standard for confirming rupture; sensitivity 91.4%, specificity 93.6%. Recommended in hemodynamically stable patients to evaluate anatomy for endovascular repair [1][1][9]
- CT findings: retroperitoneal hematoma, active contrast extravasation, crescent sign (intramural hemorrhage), draped aorta sign (contained rupture), discontinuity of aortic wall calcification [14]
- Do NOT delay surgery for imaging in hemodynamically unstable patients with a known or palpable AAA — proceed directly to the OR [7]
- Plain radiography: not sensitive or specific; may show aortic calcification or loss of psoas shadow
13. Special Tests
- Bedside FAST/aortic ultrasound: rapid identification of AAA; should be part of the initial assessment in any undifferentiated shock or abdominal pain in at-risk patients
- Resuscitative endovascular balloon occlusion of the aorta (REBOA): can be used as a temporizing measure for hemorrhage control in hemodynamically unstable patients while preparing for definitive repair [1]
- Hardman Index: scoring system for predicting mortality after rAAA repair (age >76, Cr >190 μmol/L, Hb <9 g/dL, loss of consciousness, ECG ischemia)
- Glasgow Aneurysm Score: preoperative risk stratification
14. ECG
- Obtain ECG in all patients to rule out concurrent acute MI (a common misdiagnosis) [3]
- ECG may show ST changes from demand ischemia secondary to hemorrhagic shock — ST depression (23%), ST elevation (12%) in post-repair patients with elevated troponin [13]
- Sinus tachycardia is the most common finding
- New arrhythmias (atrial fibrillation) may occur from hemodynamic stress
- Pearl: A normal ECG does not exclude rAAA; an abnormal ECG does not confirm MI — always consider rAAA in the differential of "ACS" with abdominal/back pain
15. Assessment
- rAAA is a time-critical surgical emergency with mortality increasing every minute of delay
- Overall mortality 80–90%; in-hospital surgical mortality historically ~50%, reduced to as low as 18.5% with endovascular-first protocols [1][1]
- The classic triad is present in only ~one-third of cases; maintain a high index of suspicion [6-7]
- Misdiagnosis rate of 32–42% is associated with substantially higher mortality (OR 1.83) [3][5]
- Contained (retroperitoneal) rupture may present with relative hemodynamic stability initially — this is a window for diagnosis and intervention before free rupture [8]
- Complications: hemorrhagic shock, DIC, abdominal compartment syndrome, acute kidney injury, bowel ischemia, spinal cord ischemia/paraplegia, multiorgan failure, aortoenteric fistula [1][8]
16. Treatment Plan
Initial stabilization
- Activate massive transfusion protocol and vascular surgery consultation simultaneously
- Permissive hypotension: target SBP 50–100 mmHg; limit crystalloid; prioritize blood products [1][11]
- Avoid aggressive fluid resuscitation — prevents clot disruption and the lethal triad [7][11]
- Large-bore IV access (bilateral), arterial line placement
- Consider REBOA for temporizing hemorrhage control if available [1]
Definitive repair
- Endovascular repair (EVAR) is recommended over open repair in patients with suitable anatomy (Class I, LOE B-R) [1][1]
- In hemodynamically stable patients, obtain CTA to assess EVAR suitability [1][1]
- Local anesthesia preferred over general anesthesia for EVAR to reduce perioperative mortality (Class IIa) [1][1]
- Open repair for patients with unsuitable anatomy or hemodynamic instability precluding imaging
- Endovascular balloon occlusion under fluoroscopy can reduce excessive bleeding during repair [1]
Postoperative
- ICU admission with invasive hemodynamic monitoring
- Monitor for abdominal compartment syndrome, renal failure, bowel ischemia, coagulopathy
- Serial troponin monitoring (elevated cTnI is an independent predictor of mortality, OR 4.23) [13]
- Surveillance imaging per protocol (see Follow-Up)
17. Disposition
- All confirmed or suspected rAAA → emergent surgical intervention (no patient with rAAA is a candidate for discharge or observation)
- Immediate vascular surgery consultation; if no vascular surgery available, emergent transfer to a vascular center
- Postoperatively: ICU admission mandatory
- Palliative care discussion is appropriate for patients with prohibitive surgical risk, preoperative cardiac arrest, or those who decline intervention — but the prevailing surgical view is that operation should not be denied as it provides the only hope for survival [7]
- Patients with symptomatic but unruptured AAA (pain attributable to AAA without evidence of rupture on CT): ICU admission, arterial BP monitoring, tight BP control, and repair ideally within 24–48 hours [1]
18. Follow-Up / Return Precautions
Post-repair surveillance (per 2022 ACC/AHA and SVS guidelines):
- After EVAR: CTA at 1 month postoperatively; if no endoleak or sac enlargement, annual duplex ultrasound; cross-sectional imaging (CT or MRI) every 5 years; lifelong surveillance is required [1][15-16]
- After open repair: CT or MRI within 1 year, then every 5 years (monitoring for para-anastomotic aneurysm or new aneurysm formation) [1]
- Lifelong cardiovascular risk factor management: smoking cessation, statin therapy, antihypertensive therapy, antiplatelet therapy [2]
- Return precautions (for survivors): seek immediate care for new abdominal/back/flank pain, syncope, GI bleeding (concern for aortoenteric fistula), lower extremity ischemia, or fever (graft infection)
- Screen first-degree relatives for AAA with ultrasound [1]
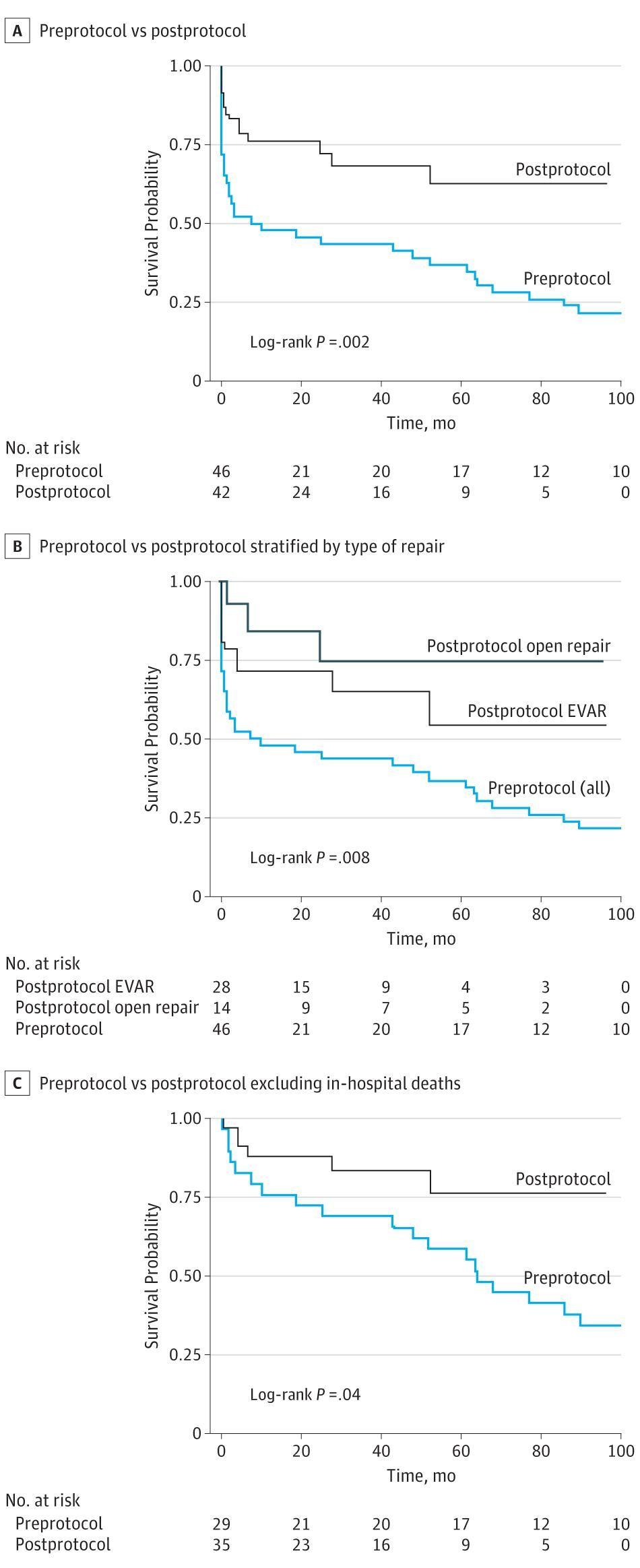
The following figure from Ullery et al. demonstrates the survival benefit associated with implementing an endovascular-first protocol for rAAA management:
References
1. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. — Writing Committee Members, Isselbacher EM, Preventza O, et al. Journal of the American College of Cardiology. 2022.
2. Abdominal Aortic Aneurysm. — Haque K, Bhargava P. American Family Physician. 2022.
3. Misdiagnosis of Ruptured Abdominal Aortic Aneurysm: Systematic Review and Meta-Analysis. — Azhar B, Patel SR, Holt PJ, et al. Journal of Endovascular Therapy : An Official Journal of the International Society of Endovascular Specialists. 2014.
4. Misdiagnosis of Ruptured Abdominal Aortic Aneurysms. — Marston WA, Ahlquist R, Johnson G, Meyer AA. Journal of Vascular Surgery. 1992.
5. Misdiagnosis of Ruptured Abdominal Aortic Aneurysms Is Common and Is Associated With Increased Mortality. — Smidfelt K, Nordanstig J, Davidsson A, Törngren K, Langenskiöld M. Journal of Vascular Surgery. 2021.
6. ACC/AHA 2005 Guidelines for the Management of Patients With Peripheral Arterial Disease (Lower Extremity, Renal, Mesenteric, and Abdominal Aortic): Executive Summary a Collaborative Report From the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) Endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; And Vascular Disease Foundation. — Hirsch AT, Haskal ZJ, Hertzer NR, et al. Journal of the American College of Cardiology. 2006.
7. Abdominal Aortic Aneurysm. — Ernst CB. The New England Journal of Medicine. 1993.
8. Abdominal Aortic Aneurysm. — Sakalihasan N, Limet R, Defawe OD. Lancet. 2005.
9. Accuracy of Presenting Symptoms, Physical Examination, and Imaging for Diagnosis of Ruptured Abdominal Aortic Aneurysm: Systematic Review and Meta-Analysis. — Fernando SM, Tran A, Cheng W, et al. Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine. 2022.
10. Livedo Reticularis as a Manifestation of Abdominal Aortic Aneurysm. — Scofield M, Kan C. The Journal of Emergency Medicine. 2025.
11. Controlled Hypotension Versus Normotensive Resuscitation Strategy for People With Ruptured Abdominal Aortic Aneurysm. — Moreno DH, Cacione DG, Baptista-Silva JC. The Cochrane Database of Systematic Reviews. 2018.
12. Computed Tomography Angiography Markers and Intraluminal Thrombus Morphology as Predictors of Abdominal Aortic Aneurysm Rupture. — Arbănași EM, Mureșan AV, Coșarcă CM, et al. International Journal of Environmental Research and Public Health. 2022.
13. Elevated Cardiac Troponin in the Early Post-Operative Period and Mortality Following Ruptured Abdominal Aortic Aneurysm: A Retrospective Population-Based Cohort Study. — Kopolovic I, Simmonds K, Duggan S, et al. Critical Care. 2012.
14. Abdominal Aortic Aneurysms Revisited: MDCT With Multiplanar Reconstructions for Identifying Indicators of Instability in the Pre- And Postoperative Patient. — Wadgaonkar AD, Black JH, Weihe EK, et al. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2015.
15. Society for Vascular Surgery Implementation of Clinical Practice Guidelines for Patients With an Abdominal Aortic Aneurysm: Postoperative Surveillance After Abdominal Aortic Aneurysm Repair. — Rokosh RS, Wu WW, Schermerhorn M, Chaikof EL. Journal of Vascular Surgery. 2021.
16. Management of Abdominal Aortic Aneurysms. — Schanzer A, Oderich GS. The New England Journal of Medicine. 2021.
17. Association of an Endovascular-First Protocol for Ruptured Abdominal Aortic Aneurysms With Survival and Discharge Disposition. — Ullery BW, Tran K, Chandra V, et al. JAMA Surgery. 2015.