Loading...
Resuscitation Reference
ACLS · PALS · NRP
Rapid Access
SHOCKABLE
Defib 200J → Epi 1mg → Amio 300mg → Defib → Epi → Amio 150mg
NON-SHOCKABLE
Epi 1mg q3-5min → Hunt H's & T's → Consider advanced airway
Quick Doses
Epi
1mg
Amio
300→150
Bicarb
50-150mEq
CaCl
1g
Mg
2g
D50
25g
Lipid
1.5mL/kg
tPA
50mg
Naloxone
0.04→0.4→2mg
Mode
VC-AC (or PRVC if available)
TV
6-8 mL/kg PBW
RR
12-16/min (avoid hyperventilation post-arrest)
PEEP
5 cmH₂O (increase if hypoxemia)
FiO₂
1.0 initially, then titrate to SpO₂ 94-98%
I:E
1:2 (consider longer expiration if obstructive)
Targets
ETCO₂ 35-45 (or per strategy), MAP stable
Post intubation checklist
- •Waveform ETCO₂ + CXR/US confirmation
- •Set alarms, secure tube, OG/NG as needed
- •Analgesia/sedation, avoid hypotension
- •Avoid hyperventilation post-arrest
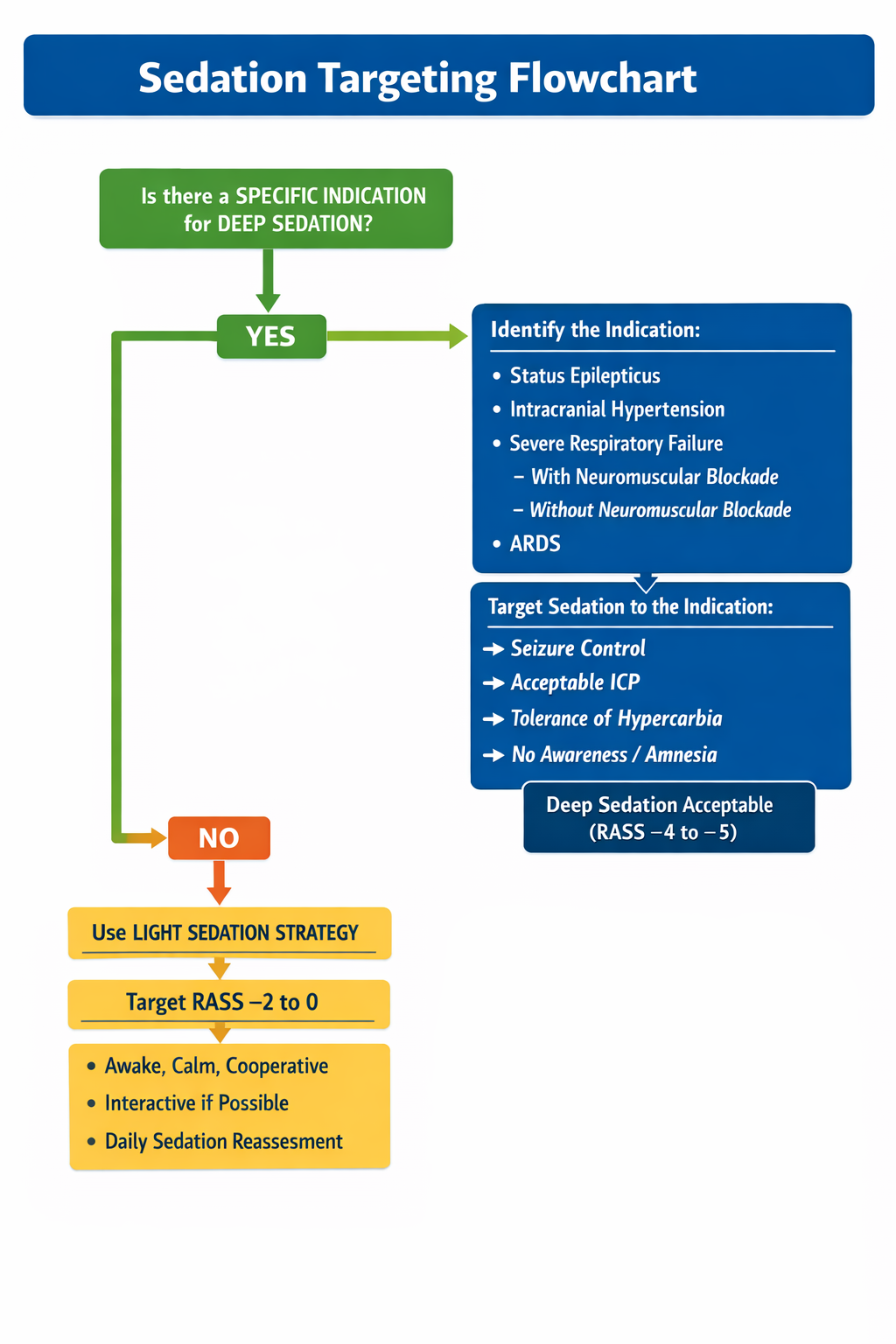
Strategy
Default to analgesia first. If no specific indication for deep sedation, aim for light sedation with frequent reassessment.
Light sedation target
RASS -2 to 0
Awake, calm, cooperative if possible
Deep sedation when indicated
RASS -4 to -5
Match target to indication
Decision Flow
+4
Combative
Combative, violent, immediate danger to staff
+3
Very agitated
Pulls to remove tubes or catheters; aggressive
+2
Agitated
Frequent non-purposeful movements, fights ventilator
+1
Restless
Anxious, apprehensive, movements not aggressive
0
Alert & calm
Spontaneously pays attention to caregiver
-1
Drowsy
Not fully alert, but has sustained awakening to voice (eye opening & contact to GREATER than 10 sec.)
-2
Light sedation
Briefly awakens to voice (eyes open & contact to LESS than 10 sec.)
-3
Moderate sedation
Movement or eye opening to voice (no eye contact)
-4
Deep sedation
No response to voice, but movement or eye opening to physical stimulation
-5
Unarousable
No response to voice or physical stimulation
Pain (analgesia)
Bolus
50-100 mcg IV q30-60min PRN
Infusion
25-100 mcg/hr (start low, titrate)
Rapid onset enables rapid titrationNo histamine release so less hemodynamically disruptiveNo toxic metabolites that accumulate in renal failure
Bolus
0.25-0.5 mg/kg IV
Infusion
1-5 mg/kg/hr
Hemodynamically stable for many patients (may increase BP at higher dose)Bronchodilator, useful in status asthmaticusAnticonvulsant propertiesAmnestic; can treat agitation refractory to other agents
Sedation
Bolus
Usually avoid; consider 10-20 mg only if stable
Infusion
5-50 mcg/kg/min, titrate by 5-10 mcg/kg/min (suggested starting rate 1 mg/kg/hour or 15 mcg/kg/min)
Rapid on/off: good for frequent neuro checksAnticonvulsant propertiesBronchodilatorLess tolerance/withdrawal than benzodiazepines in many patientsCan help in alcohol withdrawal (context dependent)
Loading
0.01-0.05 mg/kg (0.5-4 mg)
Infusion
0.02-0.1 mg/kg/hr
Bolus
0.5-4 mg intermittent
Dose dependent hemodynamic stability for many patientsRapid onsetAnticonvulsantAmnesticUseful for alcohol withdrawal and sympathomimetic intoxication
Reassess
- •Check sedation and pain after intubation and after any change
- •If paralyzed (eg rocuronium), assume pain and awareness unless treated
- •Avoid hypotension: consider fluids/pressors and sedative choice
H Causes
Recognition
Flat neck veinsTrauma/hemorrhageGI bleed
POCUS
IVC: Flat, collapsing <1cm
FAST: Free fluid
Interventions
Crystalloid bolus
2LActivate MTP
if hemorrhagic
Recognition
CyanosisAirway obstructionPre-arrest hypoxemia
POCUS
Lung: B-lines or absent sliding
Interventions
Confirm ETT
visualization + ETCO₂
FiO₂ 100%
Recognition
Renal failureDKAProlonged arrest
POCUS
Renal: Small kidneys (CKD)
Interventions
Sodium bicarbonate
1-3 ampsRecognition
Dialysis patientPeaked TsWide QRS
POCUS
Cardiac: Poor contractility
Interventions
Calcium chloride
1gBicarb + Insulin/D50
Recognition
Cold exposureTemp <30°CJ waves
POCUS
Cardiac: Slow/absent motion
Interventions
Active rewarming
warm fluids, Bair Hugger
Consider ECMO
T Causes
Recognition
Absent breath soundsTracheal deviationDifficult to bag
POCUS
Lung: Absent lung sliding
M-mode: Barcode sign
Interventions
Finger thoracostomy
5th ICS AAL
Recognition
Distended neck veinsMuffled heartsPenetrating trauma
POCUS
Subxiphoid: Pericardial effusion
RV: Diastolic collapse
Interventions
Pericardiocentesis
US-guided
Recognition
Pill bottlesWide QRSToxidrome
POCUS
Cardiac: Variable by toxin
Interventions
Lipid emulsion
1.5 mL/kgBicarb
1-2 mEq/kgif wide QRS
Recognition
DVT riskPEA narrow QRSRV dilation
POCUS
Cardiac: RV:LV >1:1, D-sign
DVT: Non-compressible vein
Interventions
tPA
50mg bolusExtended CPR
60-90min
Recognition
Respiratory depression/apnea↓ LOCMiosis (may be absent)Needles/patches/med bottles
POCUS
Lung: Often normal aeration; exclude pneumothorax/edema
Cardiac: Often normal contractility; bradycardia if hypoxic
Interventions
BVM + O₂
ventilation first; avoid hyperventilation
Naloxone (titrate)
0.04→0.4→2 mg IV/IMgoal: adequate breathing
If no IV/IM
4 mg INrepeat in 2-3 min as needed
Consider infusion
recurrent toxicity/long acting opioid
Frequently Asked Questions
The H's are: Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/hyperkalemia, and Hypothermia. The T's are: Tension pneumothorax, Tamponade (cardiac), Toxins, and Thrombosis (pulmonary or coronary). These reversible causes must be systematically addressed during cardiac arrest resuscitation.
Key ACLS medications include epinephrine (1mg IV/IO every 3-5 minutes), amiodarone (300mg IV/IO for VF/pVT, then 150mg), lidocaine (1-1.5mg/kg for VF/pVT), atropine (1mg IV for bradycardia), and calcium (1g for hyperkalemia or calcium channel blocker overdose). Dosing varies for PALS and NRP protocols.
Defibrillation (asynchronous, high energy) is used for pulseless rhythms: VF and pulseless VT. Cardioversion (synchronized, lower energy) is used for perfusing unstable tachyarrhythmias: unstable SVT, unstable atrial fibrillation/flutter, and unstable monomorphic VT. Always ensure patient is sedated for cardioversion.
ACLS (Advanced Cardiac Life Support) is for adults, PALS (Pediatric Advanced Life Support) is for children, and NRP (Neonatal Resuscitation Program) is for newborns. Key differences include compression depth (adults: 2-2.4", pediatrics: 1/3 chest depth), compression rate (all: 100-120/min), and medication dosing based on weight/age.
Reversible causes of PEA include the H's and T's: Hypovolemia (fluid resuscitation), Hypoxia (oxygenation/ventilation), Hydrogen ion/acidosis (bicarbonate), Hypo/hyperkalemia (electrolyte correction), Hypothermia (warming), Tension pneumothorax (needle decompression), Tamponade (pericardiocentesis), Toxins (antidotes), and Thrombosis (thrombolytics for PE/MI).
Opioid toxicity typically presents with respiratory depression (slow or absent breathing), decreased level of consciousness, and often miosis; hypoxia and hypercapnia can rapidly lead to bradycardia and arrest. Priorities are airway and ventilation (BVM with oxygen, early advanced airway if needed) plus naloxone for suspected opioid induced respiratory depression. Use the lowest effective naloxone dose to restore adequate ventilation, repeat titrated doses as needed, and monitor for recurrent toxicity because naloxone duration may be shorter than many opioids. Continue standard ACLS if cardiac arrest occurs.
A typical initial adult strategy is lung protective ventilation: volume assist control, tidal volume about 6-8 mL/kg predicted body weight, rate 12-16/min (adjust to target normocapnia unless permissive hypercapnia is intended), PEEP 5 cmH2O, and FiO2 1.0 initially then titrate down to maintain SpO2 around 94-98% when feasible. Confirm tube placement with waveform capnography, avoid hyperventilation (especially post arrest), and adjust settings based on ETCO2, blood gas, and hemodynamics.
Post-cardiac arrest care includes targeted temperature management (TTM) at 32-36°C for 24 hours, maintaining normoxia (SpO2 94-98%), normocapnia (PaCO2 35-45), normotension (MAP ≥65), glucose control (140-180 mg/dL), and early coronary angiography if STEMI or suspected cardiac cause. Neurologic assessment and prognostication should occur after 72 hours.