Loading...
Ventricular Fibrillation
Ventricular fibrillation (VF) is a chaotic, grossly irregular ventricular rhythm with rates usually >300 bpm and marked variability in QRS cycle length, morphology, and amplitude, resulting in no e…
Dr. Lucas Mastropaolo
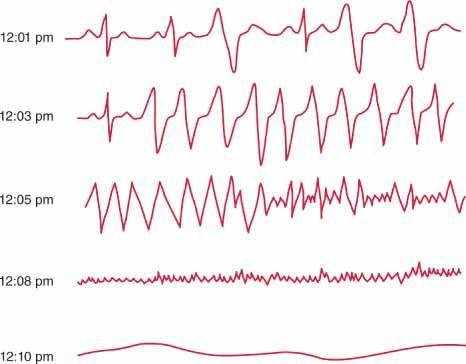
Ventricular fibrillation (VF) is a chaotic, grossly irregular ventricular rhythm with rates usually >300 bpm and marked variability in QRS cycle length, morphology, and amplitude, resulting in no effective cardiac output and immediate cardiac arrest if not treated.[1-3] Every minute without defibrillation decreases survival by approximately 7–10%.[4] The following figure illustrates the typical progression from VT to VF to asystole in sudden cardiac death:
1. History
- VF presents as sudden cardiac arrest — patients are unresponsive, pulseless, and apneic (or with agonal gasps only)[2]
- There is no "HPI" in the traditional sense; history is obtained from bystanders, family, and EMS
Key pre-arrest questions to reconstruct
- Preceding symptoms: chest pain, palpitations, dyspnea, syncope/presyncope
- Activity at onset: exertional vs. at rest (exertional arrest raises concern for CPVT, HCM, anomalous coronaries)
- Timing: witnessed vs. unwitnessed; estimated downtime; bystander CPR and AED use
- Prodromal symptoms: prior episodes of syncope, near-syncope, or palpitations
- Substance use: cocaine, amphetamines, energy drinks, alcohol
- Medication history: QT-prolonging drugs, antiarrhythmics, recent medication changes
2. Alarm Features
- VF itself is the ultimate alarm — it is a pulseless, non-perfusing rhythm and a medical emergency
Pre-arrest red flags that may precede VF
- Syncope with exertion or during emotional stress
- Chest pain with diaphoresis (acute MI)
- Known prolonged QT interval or Brugada pattern on ECG
- Family history of sudden cardiac death at young age (<40 years)
- Prior VT episodes or ICD shocks
- New-onset heart failure symptoms
3. Medications
- Acute ACLS medications (per 2025 AHA Guidelines and 2017 AHA/ACC/HRS Guidelines):[6-8]
- Epinephrine 1 mg IV/IO every 3–5 minutes during CPR (Class IIb)[8]
- Amiodarone 300 mg IV push (first dose), then 150 mg IV (second dose) for shock-refractory VF (Class I)[6][8]
- Lidocaine 1.0–1.5 mg/kg IV (alternative to amiodarone if unresponsive to CPR, defibrillation, and vasopressors; repeat 0.5–0.75 mg/kg up to 3 mg/kg total) (Class IIa)[1][8]
- IV beta blockers for polymorphic VT/VF due to myocardial ischemia or VT/VF storm (Class IIa)[8]
- Magnesium 1–2 g IV for torsades de pointes only; not beneficial for refractory VF unrelated to torsades (Class III: No Benefit)[1][8]
Medications to avoid
- High-dose epinephrine (>1 mg boluses) — no benefit over standard dosing (Class III)[8]
- Prophylactic lidocaine or high-dose amiodarone in suspected AMI — potentially harmful (Class III: Harm)[8]
- Calcium channel blockers (verapamil, diltiazem) in wide-complex tachycardia of unknown origin — potentially harmful (Class III: Harm)[8]
- Procainamide in out-of-hospital VF arrest — associated with worse outcomes[2][8]
Medications that cause VF (proarrhythmic)
- QT-prolonging drugs (antiarrhythmics, antipsychotics, fluoroquinolones, macrolides, methadone)
- Digitalis toxicity (bidirectional VT → VF)
- Cocaine, amphetamines
4. Diet
- Not directly applicable in the acute setting
Post-resuscitation and long-term considerations
- Maintain adequate potassium (goal 4.0–4.5 mEq/L) and magnesium levels
- Avoid excessive caffeine and energy drinks in patients with channelopathies
- Heart-healthy diet for underlying coronary artery disease prevention
- Alcohol moderation (binge drinking can trigger arrhythmias)
5. Review of Systems
- Cardiovascular: prior palpitations, syncope, exertional dyspnea, chest pain, known heart disease
- Neurologic: prior seizure-like episodes (may represent arrhythmic syncope misdiagnosed as seizure)
- Pulmonary: dyspnea, orthopnea (heart failure)
- Psychiatric/Substance use: cocaine, methamphetamine, synthetic cannabinoids
- Endocrine: thyroid disease (thyrotoxicosis can precipitate arrhythmias)
- Family history: sudden death, drowning, single-vehicle accidents, known channelopathies
6. Collateral History and Family History
- Critical collateral: bystander account of the arrest (witnessed vs. unwitnessed, downtime, CPR/AED use, preceding symptoms)
- Family history is essential, especially in younger patients (<40 years):[8]
- Sudden cardiac death at young age
- Known long QT syndrome, Brugada syndrome, CPVT, HCM, ARVC
- Unexplained drowning, SIDS, or single-car accidents in family members
- Genetic testing can provide a diagnosis in 13–60% of younger SCA survivors[8]
- Social context: illicit drug use, medication access, recent stressors
7. Risk Factors
- Coronary artery disease — the most common cause of VF in adults[9]
- Reduced LVEF <40% — risk increases with severity of ventricular dysfunction[2][6]
- Prior MI with scar-related reentry substrate[6][9]
- Heart failure (ischemic and nonischemic cardiomyopathy)[6]
- Channelopathies: long QT syndrome, short QT syndrome, Brugada syndrome, CPVT[10-11]
- Cardiomyopathies: HCM, ARVC, dilated cardiomyopathy[1]
- Electrolyte abnormalities: hypokalemia, hypomagnesemia[1][12]
- Drug toxicity: QT-prolonging medications, cocaine, digitalis[12]
- Acute myocardial ischemia/infarction[1][9]
- Myocarditis (viral, autoimmune, toxic)[12]
- Male sex, increasing age (for CAD-related VF)
- Idiopathic VF accounts for ~5–10% of out-of-hospital cardiac arrest survivors with structurally normal hearts[9][13]
8. Differential Diagnosis
On the monitor, VF must be distinguished from
- Pulseless ventricular tachycardia — organized wide-complex rhythm vs. chaotic VF
- Ventricular flutter — regular ~300 bpm, monomorphic, sinusoidal pattern[1]
- Torsades de pointes — polymorphic VT with "twisting of the points" in setting of prolonged QT[1]
- Artifact/lead disconnect — check the patient; artifact mimics VF but patient has a pulse
- Fine VF vs. asystole — confirm in multiple leads; fine VF may appear isoelectric in some leads
- SVT with aberrancy — not typically pulseless
- Etiologic differential (reversible causes — the "Hs and Ts"):[12]
- Hypovolemia, Hypoxia, Hydrogen ion (acidosis), Hypo/Hyperkalemia, Hypothermia
- Tension pneumothorax, Tamponade, Toxins, Thrombosis (coronary or pulmonary)
9. Past Medical History
- Prior MI or coronary artery disease — most important risk factor
- Known cardiomyopathy (ischemic, dilated, hypertrophic, ARVC)
- Prior cardiac arrest or VT episodes
- ICD in situ — interrogate device for stored arrhythmia data
- Prior cardiac surgery (CABG, valve replacement)
- Known channelopathy or family history of sudden death
- Chronic kidney disease (electrolyte derangements)
- Thyroid disease
- Medication list — especially antiarrhythmics, QT-prolonging drugs
10. Physical Exam
During arrest
- Unresponsive, no pulse, no effective respirations (agonal gasps may be present)
- Confirm pulselessness at carotid/femoral arteries
Post-ROSC focused exam
- Vitals: blood pressure (target MAP ≥65 mmHg, avoid hypotension), temperature, SpO2
- Cardiovascular: murmurs (valvular disease, HCM), JVD, S3 (heart failure)
- Pulmonary: crackles (pulmonary edema), absent breath sounds (pneumothorax)
- Neurologic: GCS, pupillary reactivity, corneal reflexes, motor response — critical for neuroprognostication baseline
- Skin: track marks (drug use), cyanosis, mottling
- Stigmata of trauma: if arrest was unwitnessed
11. Lab Studies
Stat labs during/after resuscitation
- BMP/CMP: potassium, magnesium, calcium, glucose, renal function, bicarbonate/pH
- Troponin: serial measurements to evaluate for ACS as cause[12]
- ABG/VBG: pH, lactate, PaO2, PaCO2
- CBC: anemia, infection
- Coagulation studies: PT/INR, PTT
- Toxicology screen: urine drug screen, serum drug levels (digoxin, antiarrhythmics)
- TSH if thyroid disease suspected
- BNP/NT-proBNP if heart failure suspected
- Expected abnormalities: lactic acidosis, hyperkalemia (or hypokalemia as cause), elevated troponin (may be from arrest itself or causative ACS), transient renal/hepatic injury
- Monitoring: serial potassium and magnesium (maintain K+ >4.0, Mg2+ >2.0)
12. Imaging
Echocardiography — first-line post-ROSC to assess
- LV function (wall motion abnormalities suggesting ischemia, reduced EF)
- Structural heart disease (HCM, ARVC, valvular disease)
- Pericardial effusion/tamponade
- Regional wall motion abnormalities
Coronary angiography — recommended emergently for
- STEMI on post-ROSC ECG (Class I)[6][8]
- Should be considered even without ST elevation if cardiac etiology suspected — one-third of patients without ST elevation have a culprit lesion[8]
- Chest X-ray: ETT placement, pulmonary edema, pneumothorax, cardiomegaly
- CT head: if prolonged arrest or concern for neurologic injury/primary neurologic event
- CT chest/abdomen: if PE or aortic dissection suspected
- Cardiac MRI: post-stabilization for myocarditis, ARVC, infiltrative disease, scar characterization
13. Special Tests
- Electrophysiology study (EPS): post-stabilization for risk stratification and to guide ICD implantation or ablation[8]
- Genetic testing: recommended in patients <40 years with unexplained SCA and no structural heart disease — yield of 13–60%[8][14]
- Pharmacologic provocation: sodium channel blocker challenge (ajmaline/procainamide) for Brugada syndrome; epinephrine challenge for LQTS[14]
- Signal-averaged ECG: late potentials suggesting arrhythmogenic substrate[15]
- Exercise stress testing: to unmask CPVT, exercise-induced arrhythmias, or ischemia[15]
- Point-of-care ultrasound (POCUS): during arrest to identify reversible causes (tamponade, PE, hypovolemia)[16]
14. ECG
VF ECG characteristics
- Rapid, grossly irregular electrical activity >300 bpm
- No identifiable QRS complexes, P waves, or T waves
- Marked variability in waveform amplitude, morphology, and cycle length
- Coarse VF: higher amplitude fibrillatory waves (more likely to respond to defibrillation)
- Fine VF: low amplitude waves approaching isoelectric line (confirm in multiple leads to distinguish from asystole)
Post-ROSC ECG — look for
- ST elevation → emergent cath lab activation
- Prolonged QTc → drug-induced or congenital LQTS
- Brugada pattern (coved ST elevation V1–V2)
- Epsilon waves, T-wave inversions V1–V3 → ARVC
- Short QT interval → short QT syndrome
- Early repolarization pattern in inferior/lateral leads
- Signs of hyperkalemia (peaked T waves, widened QRS)
- Delta waves (WPW with pre-excited AF → VF)
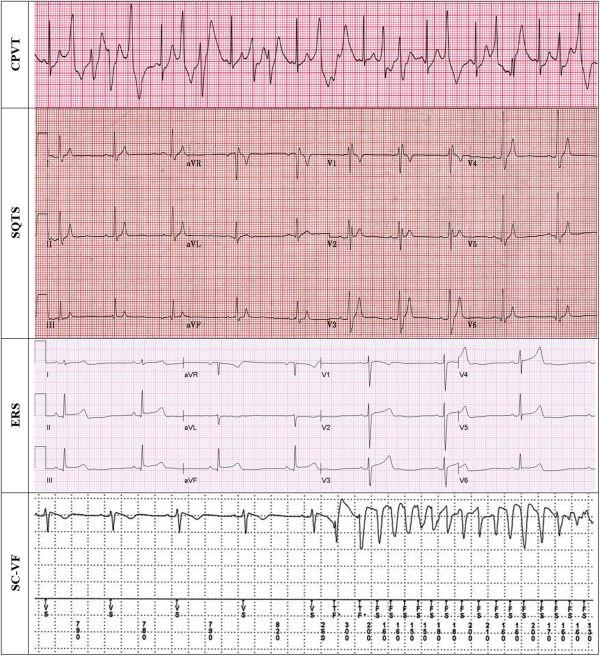
- The following figure illustrates ECG patterns of latent causes of sudden cardiac arrest, including CPVT, short QT syndrome, early repolarization syndrome, and short-coupled VF:
- View full figure Figure 2. ECG Examples of “Latent” Cardiac Arrest Conditions Latent Causes of Sudden Cardiac Arrest. JACC Clin Electrophysiol. May 31, 2022.
15. Assessment
- VF is a lethal arrhythmia that results in immediate hemodynamic collapse and death within minutes if untreated[8]
- Survival decreases rapidly: >90% in monitored ICU settings with immediate defibrillation, but ≤25% by 4–5 minutes and 0% by 10 minutes without intervention[8]
- Survival is better for patients presenting with VF/pVT than for those with bradyarrhythmic or asystolic mechanisms[8]
- Severity stratification post-ROSC depends on: downtime, initial rhythm, bystander CPR, time to ROSC, neurologic status, hemodynamic stability, and underlying etiology
- Typical presentation: witnessed collapse → bystander CPR → AED/EMS defibrillation → ROSC
- Atypical presentations: unwitnessed arrest found in asystole (VF may have degenerated), seizure-like activity (arrhythmic syncope), drowning
- Complications: anoxic brain injury (leading cause of death post-ROSC), cardiogenic shock, multiorgan failure, aspiration pneumonia, rib fractures from CPR, post-cardiac arrest syndrome[18]
16. Treatment Plan
Immediate (during arrest) — per 2025 AHA ACLS Guidelines
- High-quality CPR — minimize interruptions, 100–120 compressions/min, full recoil
- Defibrillation — as soon as possible; biphasic defibrillator preferred
- Manufacturer-recommended energy or maximum dose if unknown[7]
- Single shock strategy → immediate CPR resumption (do not stack shocks)[7]
- Escalating energy (200→300→360 J) may improve conversion in patients requiring multiple shocks[7]
- Epinephrine 1 mg IV/IO every 3–5 min[8]
- Amiodarone 300 mg IV push after ≥3 failed shocks → repeat 150 mg once[1][8]
- Identify and treat reversible causes (Hs and Ts)[12]
Post-ROSC management
- Temperature control: maintain constant temperature 32°C–37.5°C for at least 36 hours; prevent fever[19-20]
- Hemodynamic support: target MAP ≥65 mmHg; vasopressors as needed
- Oxygenation: avoid hyperoxia (target SpO2 92–98%); avoid hypoxia
- Ventilation: target normocapnia (PaCO2 35–45 mmHg)
- Coronary angiography: emergent for STEMI; consider for suspected cardiac etiology even without ST elevation[6][8]
- Seizure management: continuous EEG monitoring; treat clinical seizures[18-19]
- Neuroprognostication: multimodal approach, delay ≥72 hours after return to normothermia[16]
Secondary prevention
- ICD implantation — indicated for survivors of VF/pulseless VT after evaluation to exclude completely reversible causes (Class I)[8][12]
- ICD is NOT indicated if VF was due to a completely reversible disorder without structural heart disease (e.g., isolated electrolyte imbalance, drug toxicity, trauma)[12]
- Catheter ablation for recurrent VF triggered by consistent PVC morphology[8]
- Antiarrhythmic therapy: amiodarone ± beta blocker infusion post-resuscitation; beta blockers are cornerstone of long-term prevention[4]
- Genetic evaluation and family screening in young patients with unexplained VF[8]
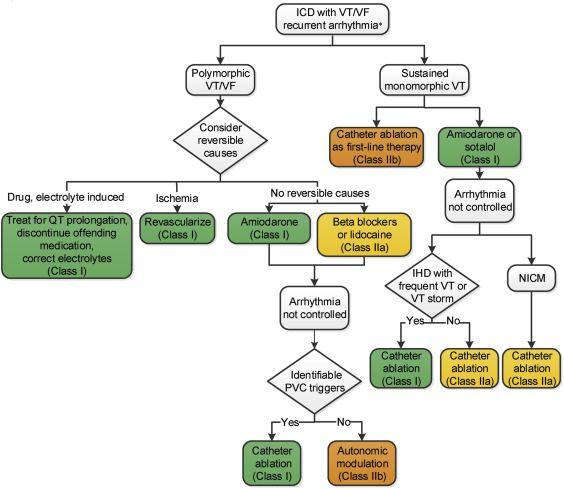
- The following algorithm summarizes the approach to recurrent VT/VF in patients with structural heart disease:
View full figure Figure 5. Treatment of Recurrent VA in Patients With Ischemic Heart Disease or NICM 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J Am Coll Cardiol. October 1, 2018.
17. Disposition
- All VF cardiac arrest patients require ICU admission — no exceptions[18][21]
- Cardiac arrest center transfer if local facility lacks comprehensive post-arrest capabilities (cath lab, TTM, EP, neurocritical care)[21]
- Admission criteria: all patients with ROSC after VF arrest
- Observation is not appropriate — VF arrest mandates full ICU-level care
Specialist consultation triggers
- Cardiology/interventional cardiology (emergent if STEMI or suspected ACS)
- Electrophysiology (for ICD evaluation, ablation consideration)
- Neurology/neurocritical care (neuroprognostication, seizure management)
- Genetics (young patients with unexplained VF)[8]
- Palliative care (if poor neurologic prognosis established)
18. Follow Up / Return Precautions
For survivors discharged after VF arrest
- Cardiology/EP follow-up within 1–2 weeks of discharge
- ICD follow-up: device check within 2 weeks, then per protocol (remote monitoring)
- Cardiac rehabilitation referral
- Driving restrictions: per local regulations (typically 6 months post-ICD for secondary prevention)
- Psychological support: screen for PTSD, anxiety, depression — common in cardiac arrest survivors[21]
- Family screening: ECG, echocardiography, and genetic counseling for first-degree relatives if channelopathy or inherited cardiomyopathy suspected[8]
Return precautions for patients/families
- Return immediately for: syncope, presyncope, palpitations, chest pain, ICD shocks, dyspnea
- Expected recovery: neurologic recovery may continue for months; cognitive deficits are common
- Medication adherence (beta blockers, antiarrhythmics) is critical
- Avoid QT-prolonging medications (reference: www.crediblemeds.org)
- Avoid triggers specific to underlying condition (e.g., competitive sports in CPVT/LQTS, fever in Brugada syndrome)
References
1. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). — European Heart Rhythm Association, Heart Rhythm Society, Zipes DP, et al. Journal of the American College of Cardiology. 2006.
2. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
3. 2019 HRS/EHRA/APHRS/LAHRS Expert Consensus Statement on Catheter Ablation of Ventricular Arrhythmias: Executive Summary. — Cronin EM, Bogun FM, Maury P, et al. Heart Rhythm. 2020.
4. Handling of Ventricular Fibrillation in the Emergency Setting. — Szabó Z, Ujvárosy D, Ötvös T, Sebestyén V, Nánási PP. Frontiers in Pharmacology. 2019.
5. The Electrophysiology Study in the Evaluation and Treatment of Ventricular Arrhythmias. — Richard Fogoros, John Mandrola Fogoros' Electrophysiologic Testing, 7th Edition. 2023.
6. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
7. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Wigginton JG, Agarwal S, Bartos JA, et al. Circulation. 2025.
8. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Heart Rhythm. 2018.
9. Venice Chart International Consensus Document on Ventricular Tachycardia/Ventricular Fibrillation Ablation. — Natale A, Raviele A, Al-Ahmad A, et al. Journal of Cardiovascular Electrophysiology. 2010.
10. Cardiac Channelopathies: Clinical Diagnosis and Promising Therapeutics. — Dib Nehme R, Sinno L, Shouman W, et al. Journal of the American Heart Association. 2025.
11. Sudden Death in the Young: Information for the Primary Care Provider. — Erickson CC, Salerno JC, Berger S, et al. Pediatrics. 2021.
12. 2016 AHA/ACC Clinical Performance and Quality Measures for Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Performance Measures. — Al-Khatib SM, Yancy CW, Solis P, et al. Journal of the American College of Cardiology. 2017.
13. Distinct Substrates of Idiopathic Ventricular Fibrillation Revealed by Arrhythmia Characteristics on Implantable Cardioverter-Defibrillator. — Haïssaguerre M, Sellal JM, Benali K, et al. JACC. Clinical Electrophysiology. 2024.
14. Idiopathic Ventricular Fibrillation: The Ongoing Quest for Diagnostic Refinement. — Conte G, Giudicessi JR, Ackerman MJ. Europace : European Pacing, Arrhythmias, and Cardiac Electrophysiology : Journal of the Working Groups on Cardiac Pacing, Arrhythmias, and Cardiac Cellular Electrophysiology of the European Society of Cardiology. 2021.
15. Sudden Death in Patients Without Structural Heart Disease. — Wever EF, Robles de Medina EO. Journal of the American College of Cardiology. 2004.
16. Part 1: Executive Summary: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Merchant RM, Topjian AA, Panchal AR, et al. Circulation. 2020.
17. Latent Causes of Sudden Cardiac Arrest. — Krahn AD, Tfelt-Hansen J, Tadros R, et al. JACC. Clinical Electrophysiology. 2022.
18. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Panchal AR, Bartos JA, Cabañas JG, et al. Circulation. 2020.
19. Part 11: Post-Cardiac Arrest Care: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Hirsch KG, Amorim E, Coppler PJ, et al. Circulation. 2025.
20. 2023 American Heart Association Focused Update on Adult Advanced Cardiovascular Life Support: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Perman SM, Elmer J, Maciel CB, et al. Circulation. 2024.
21. Part 7: Systems of Care: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Berg KM, Cheng A, Panchal AR, et al. Circulation. 2020.