Loading...
Viral Meningitis
Viral meningitis is the most common form of meningitis, with an annual incidence of approximately 2.7–7.6 per 100,000 adults.[1-2] It is an inflammation of the meninges characterized by acute onset…
Dr. Lucas Mastropaolo
Viral meningitis is the most common form of meningitis, with an annual incidence of approximately 2.7–7.6 per 100,000 adults.[1-2] It is an inflammation of the meninges characterized by acute onset of meningeal symptoms, fever, CSF pleocytosis, and no growth on routine bacterial culture.[3] While generally self-limiting, it is not always benign — up to 20% of patients have unfavorable outcomes at 30 days, and long-term neuropsychiatric sequelae are increasingly recognized.[1][4]
1. History
- Headache is nearly universal (99–100%), typically severe, diffuse, and worsened by movement[5-6]
- Fever present in 65–81%; may be absent at time of presentation (only 48% febrile ≥38°C on arrival)[5-6]
- Photophobia/phonophobia in 63–77%[5-6]
- Nausea/vomiting in ~76%[5]
- Neck stiffness reported by only 37–50% of patients[5-6]
- The classic triad of headache + neck stiffness + photophobia is present in only 28%[1]
- Onset typically acute over 1–3 days; median 2 days from symptom onset to presentation[5]
- Ask about prodromal illness: upper respiratory symptoms (~14%) or gastroenteritis (~16%) suggest enteroviral etiology[5]
- Ask about sick contacts — concurrent illness in family/relatives in 53% of enterovirus cases[5]
- Ask about genital herpes history (HSV-2), shingles/varicella (VZV), recent travel, tick exposure, HIV risk factors[1][7]
- Seasonality: enterovirus peaks summer–autumn; HSV-2 and VZV are year-round[5][8]
2. Alarm Features
- Altered mental status/decreased consciousness — suggests encephalitis or bacterial meningitis; the triad of fever + neck stiffness + decreased consciousness essentially never occurs in isolated viral meningitis[2]
- Seizures — rare in viral meningitis (0% in one cohort); consider HSV encephalitis, bacterial meningitis[6]
- Focal neurologic deficits — suggest encephalitis or space-occupying lesion[9]
- Petechial/purpuric rash — meningococcemia until proven otherwise[9]
- Rapidly progressive symptoms or hemodynamic instability
- Immunocompromised state — higher risk of atypical pathogens and severe disease[8-9]
- Neonates and infants — nonspecific presentations; higher morbidity[9]
- Papilledema — suggests raised intracranial pressure; obtain imaging before LP
3. Medications
- Empiric antibiotics (ceftriaxone + vancomycin ± ampicillin) should be started immediately when bacterial meningitis cannot be excluded, and discontinued once aseptic meningitis is confirmed[9-10]
- Acyclovir should be started empirically if HSV encephalitis is suspected; however, for isolated HSV-2 or VZV meningitis (without encephalitis), early antiviral treatment was not associated with improved outcomes in a large prospective cohort[1]
- Approximately 21% of patients with undiagnosed lymphocytic meningitis receive unnecessary acyclovir courses[4]
- Drug-induced aseptic meningitis is an important consideration — common culprits include NSAIDs (especially ibuprofen), trimethoprim-sulfamethoxazole, IVIG, intrathecal agents, and monoclonal antibodies[6]
- Supportive medications: analgesics (acetaminophen, NSAIDs), antiemetics, IV fluids
- Dexamethasone is recommended for suspected bacterial meningitis (10 mg IV q6h × 4 days) but has no established role in viral meningitis[9-10]
4. Diet
- No specific dietary triggers or restrictions
- Adequate hydration is essential, particularly with fever, nausea, and poor oral intake
- Patients with significant nausea/vomiting may require IV fluid resuscitation
- No long-term dietary modifications needed
5. Review of Systems
- Neurologic: headache character/severity, photophobia, phonophobia, confusion, vision changes, weakness, numbness, seizures
- Constitutional: fever, chills, malaise, fatigue, myalgias
- GI: nausea, vomiting, diarrhea (enteroviral prodrome)
- Respiratory: cough, rhinorrhea, sore throat (enteroviral prodrome)
- Dermatologic: vesicular rash (HSV genital lesions, zoster dermatome), petechiae/purpura (meningococcal)
- Genitourinary: genital lesions, urinary retention (sacral radiculitis with HSV-2)
- Musculoskeletal: myalgias, arthralgias
6. Collateral History and Family History
- Sick contacts — concurrent febrile or GI illness in household members strongly suggests enterovirus (present in 53% of enterovirus meningitis cases)[5]
- Daycare/school exposure in pediatric contacts
- Sexual history — HSV-2 serostatus, new partners (HSV-2 is the second most common cause at ~16%)[1]
- Travel history — arboviruses (West Nile, Japanese encephalitis, Toscana, Dengue, Zika)[7]
- Tick exposure — tick-borne encephalitis[7]
- Immunosuppression — HIV status, transplant, chemotherapy; VZV meningitis associated with immunosuppression in 20% of cases[1]
- Previous episodes of meningitis — recurrent episodes suggest Mollaret meningitis (HSV-2), seen in ~22% of HSV-2 meningitis patients[11]
- Family history of immunodeficiency or recurrent infections may suggest genetic susceptibility[12]
7. Risk Factors
- Age: young adults most commonly affected (median age 31–33 years)[1][5]
- Female sex: 54% of cases; 77% of HSV-2 meningitis cases are female; females have higher risk of unfavorable outcomes (aRR 1.34)[1]
- Summer–autumn season for enterovirus[5]
- Immunosuppression: particularly for VZV meningitis (20% immunosuppressed)[1]
- HSV-2 seropositivity: risk factor for both primary and recurrent (Mollaret) meningitis[11-12]
- HIV infection: associated with aseptic meningitis at seroconversion and increased susceptibility[6]
- Close-contact settings: dormitories, military barracks, daycare (enterovirus transmission)
- Lack of vaccination: measles, mumps, varicella, Japanese encephalitis in endemic areas[7]
8. Differential Diagnosis
- The critical task in the ED is distinguishing viral meningitis from bacterial meningitis, which is a medical emergency.[6]
- Bacterial meningitis — more toxic appearance, altered mental status (60–69%), higher CSF WBC (usually >1000/μL), neutrophilic predominance, elevated protein (>100 mg/dL), low glucose (<30 mg/dL), positive Gram stain (50–90% sensitivity)[9][13]
- HSV encephalitis — altered mental status, seizures, temporal lobe findings on MRI; requires urgent IV acyclovir[7]
- Tuberculous meningitis — subacute onset, cranial nerve palsies, basilar enhancement, CSF lymphocytic with very low glucose[8]
- Fungal meningitis (Cryptococcus) — immunocompromised patients, subacute/chronic course, elevated opening pressure[14]
- Subarachnoid hemorrhage — thunderclap headache, xanthochromia; 8% of enterovirus meningitis initially misdiagnosed as SAH[5]
- Drug-induced aseptic meningitis — temporal relationship with offending medication[15]
- Autoimmune/inflammatory meningitis — SLE, neurosarcoidosis, Behçet disease, anti-NMDAR encephalitis[15]
- Meningeal carcinomatosis — subacute, cranial neuropathies, known malignancy[13]
- Neurosyphilis — should be considered in undiagnosed aseptic meningitis, especially with HIV risk factors[6]
9. Past Medical History
- Previous episodes of meningitis — recurrence in 2% of viral meningitis; Mollaret meningitis defined as ≥3 self-resolving episodes[5][15]
- HSV-2 infection — genital herpes history; 22% progression risk from single-episode to recurrent meningitis[11]
- Immunocompromising conditions — HIV/AIDS, transplant, chemotherapy, biologics
- Varicella/zoster history — VZV meningitis associated with concurrent shingles in 60%[1]
- Vaccination history — MMR, varicella, meningococcal
- Neurosurgical history — VP shunt raises concern for bacterial etiology
- Autoimmune conditions — may cause aseptic meningitis or predispose to infections
10. Physical Exam
- Vital signs: temperature ≥38°C in ~48% at presentation; tachycardia common; hypotension suggests sepsis/bacterial etiology[5]
- Mental status: should be normal or near-normal in viral meningitis; altered mentation (present in 60–69% of bacterial meningitis) is a red flag[9]
- Nuchal rigidity: present in 37–50% of viral meningitis[5-6]
- Kernig sign: low sensitivity (2–23%)[9]
- Brudzinski sign: low sensitivity (2–28%)[9]
- Jolt accentuation test: sensitivity 52–65% for meningitis[9]
- Skin exam: vesicular lesions (HSV, VZV dermatomal rash); petechiae/purpura (meningococcal — urgent escalation)
- Cranial nerves: deficits suggest encephalitis or raised ICP
- Fundoscopy: papilledema warrants imaging before LP
- Genital exam: if HSV-2 suspected, look for active herpetic lesions
11. Lab Studies
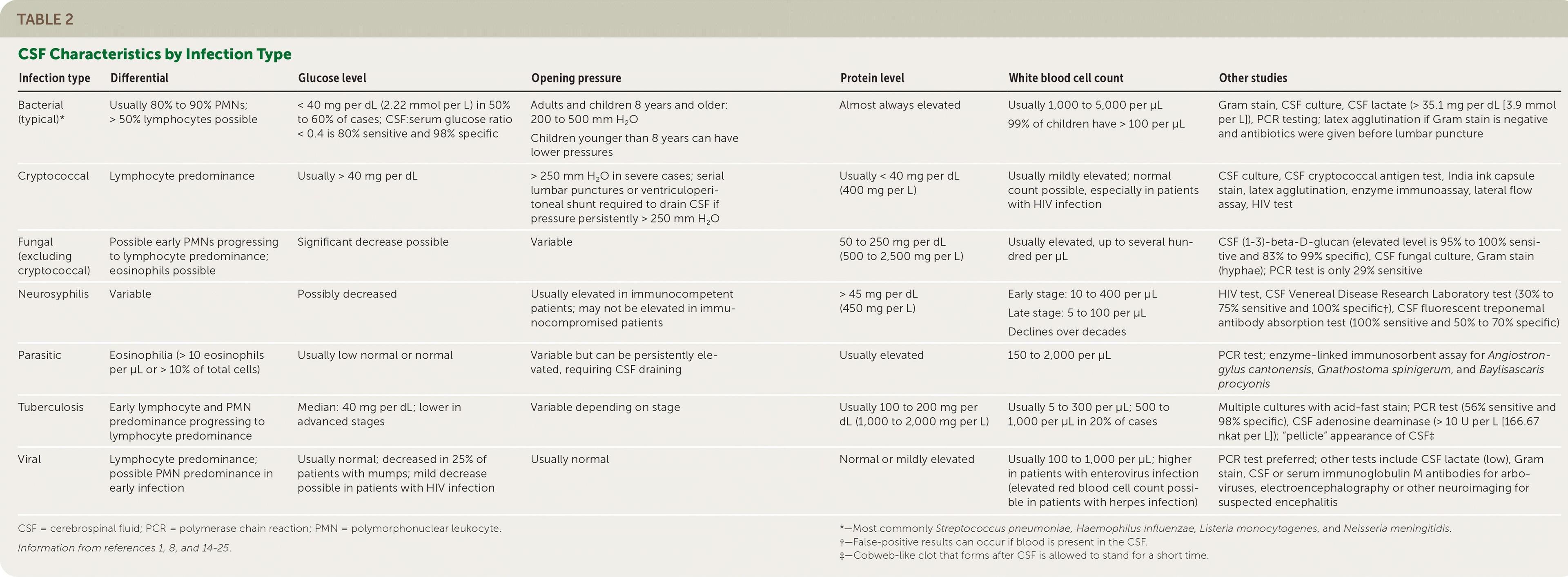
CSF analysis is the cornerstone of diagnosis
- The following table summarizes typical CSF findings by infection type:
- Table 2. CSF Characteristics by Infection Type Cerebrospinal Fluid Analysis. Am Fam Physician. March 31, 2021.
Key CSF findings in viral meningitis
- WBC: typically 100–1,000/μL (median 160, IQR 60–358); lymphocyte predominance (though early PMN predominance can occur, especially with enterovirus)[1][8]
- Protein: normal or mildly elevated
- Glucose: usually normal (decreased in only ~25% of mumps cases)[14]
- CSF lactate: low (helps distinguish from bacterial; AUC 0.98)[13]
Serum studies
- CBC, CRP (median CRP 8 mg/L in enterovirus — much lower than bacterial)[5]
- Procalcitonin: excellent discriminator for bacterial vs. viral (sensitivity 95%, specificity 97%, AUC 0.98); combined PCT + CSF protein yields AUC 0.998[13][16]
- Blood cultures (×2) — to rule out bacteremia
- HIV testing — should be considered in all undiagnosed aseptic meningitis[6]
- RPR/VDRL if neurosyphilis is a concern[6]
12. Imaging
- CT head before LP is indicated only if: focal neurologic deficits, papilledema, altered mental status, new-onset seizures, or immunocompromised state[9]
- Unnecessary neuroimaging delays LP and decreases pathogen yield[4]
- MRI brain with contrast if encephalitis is suspected (temporal lobe signal changes in HSV encephalitis)
- Routine imaging is not necessary in an immunocompetent patient with classic meningitis presentation and no red flags
13. Special Tests
- CSF multiplex PCR (e.g., BioFire FilmArray Meningitis/Encephalitis Panel): rapid identification of viral pathogens; 24/7 availability significantly reduces hospitalization rate (73.9% → 42.0%), antibiotic use, and length of stay[17]
- CSF enterovirus PCR: most important single test; rapid turnaround enables early antibiotic discontinuation[6][17]
- CSF HSV-1/2 PCR: essential to distinguish meningitis from encephalitis
- CSF VZV PCR: particularly in immunocompromised or patients with concurrent shingles
- Bacterial Meningitis Score and validated risk scores can help stratify low-risk patients (99.5–100% sensitivity for ruling out bacterial meningitis)[13]
- Opening pressure: typically normal in viral meningitis; elevated in bacterial or cryptococcal
14. ECG
- Not routinely indicated for viral meningitis
- Consider ECG if enteroviral myocarditis is suspected (chest pain, dyspnea, tachycardia out of proportion)
- ECG monitoring if hemodynamically unstable or sepsis is a concern
- Enterovirus D68 and Coxsackievirus B are associated with myocarditis/pericarditis
15. Assessment
- Viral meningitis is the most common cause of meningitis overall (~72% of all meningitis cases)[13]
- Most common pathogens: enteroviruses (39%), HSV-2 (16%), VZV (15%); pathogen unidentified in 27%[1]
- The classic triad is present in only 28% — absence does not rule out meningitis[1]
- Despite being labeled "benign," 20% have unfavorable outcomes at 30 days (GOS 1–4)[1]
- Long-term sequelae include headache (28% at 6 months), fatigue (31%), cognitive impairment (36%), and sleep disturbance (31%)[18-19]
- At 6 months post-infection, approximately 25% of patients have reduced or no work ability[19]
- Outcomes are similar across viral etiologies; female sex is an independent risk factor for unfavorable outcome[1]
16. Treatment Plan
Initial stabilization
- IV access, fluid resuscitation if dehydrated, antipyretics, analgesics, antiemetics
Empiric therapy (until bacterial meningitis excluded)
- Ceftriaxone 2g IV q12h + vancomycin 15–20 mg/kg IV q8–12h[9]
- Add ampicillin 2g IV q4h if Listeria risk (age >50, pregnancy, immunocompromised)[9]
- Dexamethasone 0.15 mg/kg IV q6h × 4 days — give with or before first antibiotic dose if bacterial meningitis suspected[9-10]
- Acyclovir 10 mg/kg IV q8h if HSV encephalitis is a concern[10]
Once viral meningitis confirmed
- Discontinue antibiotics[9]
- Supportive care: analgesics, hydration, rest in a dark/quiet room
- Antivirals are not routinely recommended for HSV-2 or VZV meningitis (without encephalitis) — early antiviral treatment was not associated with improved outcomes[1][4]
- For Mollaret meningitis: IV acyclovir during acute episodes is standard practice, though evidence for prevention of recurrence is limited; some patients use patient-initiated episodic valacyclovir at symptom onset[20-21]
17. Disposition
Admission criteria
- Diagnostic uncertainty (cannot exclude bacterial meningitis pending cultures/PCR)
- Altered mental status or focal neurologic deficits
- Immunocompromised patients
- Inability to tolerate oral intake
- Significant comorbidities or extremes of age
- Suspected encephalitis
Discharge from ED may be appropriate if
- Rapid CSF viral PCR confirms enteroviral etiology[17]
- Patient is well-appearing, tolerating PO, normal mental status
- Reliable follow-up available
- 24/7 multiplex PCR availability reduced hospitalization from 74% to 42%[17]
- Median length of stay: 4 days (can be reduced to <1 day with rapid on-site PCR)[4][17]
Specialist consultation triggers
- Infectious diseases: atypical CSF profile, immunocompromised, HIV-associated
- Neurology: seizures, focal deficits, suspected encephalitis, recurrent meningitis
- ICU: hemodynamic instability, respiratory compromise, severely altered mental status
18. Follow Up / Return Precautions
Follow-up timing
- Outpatient follow-up at 1 month — assess for persistent symptoms[19]
- Consider repeat assessment at 3 and 6 months given high rates of persistent sequelae[19]
- Neuropsychological testing should be considered if cognitive complaints persist (utilized in only 26% of patients in one cohort)[19]
- Return precautions — instruct patients to return immediately for:
- Worsening or new-onset confusion/altered behavior
- New seizures
- Worsening headache unresponsive to analgesics
- High fever (>39°C) or inability to keep fluids down
- New rash (especially petechial/purpuric)
- Neck stiffness worsening
- Vision changes or new weakness
Patient counseling
- Most patients recover fully within 7–18 days of acute symptoms[9]
- However, persistent symptoms are common: headache (56% at 1 month, 28% at 6 months), concentration difficulty, fatigue, sound sensitivity[19]
- At 6 months, ~25% still have reduced work capacity; female sex and lower GOS at discharge predict slower return to work[19]
- Reassure that viral meningitis is not typically contagious person-to-person (though enteroviruses spread via fecal-oral/respiratory routes — hand hygiene is important)
- For HSV-2 meningitis: counsel about 22% risk of recurrence (Mollaret meningitis) and to seek care promptly with recurrent symptoms[11]
References
1. Clinical Features and Prognostic Factors in Adults With Viral Meningitis. — Petersen PT, Bodilsen J, Jepsen MPG, et al. Brain : A Journal of Neurology. 2023.
2. Red and Orange Flags for Secondary Headaches in Clinical Practice: SNNOOP10 List. — Do TP, Remmers A, Schytz HW, et al. Neurology. 2019.
3. Viral (Aseptic) Meningitis: A Review. — Wright WF, Pinto CN, Palisoc K, Baghli S. Journal of the Neurological Sciences. 2019.
4. Incidence, Aetiology, and Sequelae of Viral Meningitis in UK Adults: A Multicentre Prospective Observational Cohort Study. — McGill F, Griffiths MJ, Bonnett LJ, et al. The Lancet. Infectious Diseases. 2018.
5. Enterovirus Meningitis in Adults: A Prospective Nationwide Population-Based Cohort Study. — Bodilsen J, Mens H, Midgley S, et al. Neurology. 2021.
6. The impact of cerebrospinal fluid viral polymerase chain reaction testing on the management of adults with viral meningitis: A multi‐center retrospective study. — Kim MG, Gulholm T, Lennard K, et al. Journal of Medical Virology. 2023.
7. Viral Meningitis and Encephalitis: An Update. — Gundamraj V, Hasbun R. Current Opinion in Infectious Diseases. 2023.
8. Diagnostic Test Accuracy of Jolt Accentuation for Headache in Acute Meningitis in the Emergency Setting. — Iguchi M, Noguchi Y, Yamamoto S, Tanaka Y, Tsujimoto H. The Cochrane Database of Systematic Reviews. 2020.
9. Aseptic and Bacterial Meningitis: Diagnosis, Treatment, and Prevention. — Krebs L, Durden B, Saguil A. American Family Physician. 2026.
10. Clinical Reasoning: A 44-Year-Old Woman With Headache Followed by Sudden Neurologic Decline. — Berkowitz AL, Kimchi EY, Hwang DY, et al. Neurology. 2013.
11. Benign Recurrent Lymphocytic Meningitis (Mollaret's Meningitis) in Denmark: A Nationwide Cohort Study. — Petersen PT, Bodilsen J, Jepsen MPG, et al. European Journal of Neurology. 2024.
12. Whole-Exome Sequencing of Patients With Recurrent HSV-2 Lymphocytic Mollaret Meningitis. — Hait AS, Thomsen MM, Larsen SM, et al. The Journal of Infectious Diseases. 2021.
13. Progress and Challenges in Bacterial Meningitis: A Review. — Hasbun R. The Journal of the American Medical Association. 2022.
14. Cerebrospinal Fluid Analysis. — Shahan B, Choi EY, Nieves G. American Family Physician. 2021.
15. Clinical Reasoning: A 35-Year-Old Man With 2 Episodes of Meningoencephalitis Associated With Flu-Like Illnesses. — Amin AJ, Lewis SL. Neurology. 2015.
16. Microbial Aspects and Potential Markers for Differentiation Between Bacterial and Viral Meningitis Among Adult Patients. — Alnomasy SF, Alotaibi BS, Mujamammi AH, Hassan EA, Ali ME. PloS One. 2020.
17. Impact of a 24/7 Multiplex-PCR on the Management of Patients With Confirmed Viral Meningitis. — Péan de Ponfilly G, Chauvin A, Salmona M, et al. The Journal of Infection. 2021.
18. Long-Term Sequelae After Viral Meningitis and Meningoencephalitis Are Frequent, Even in Mildly Affected Patients, a Prospective Observational Study. — Schwitter J, Branca M, Bicvic A, et al. Frontiers in Neurology. 2024.
19. Ability to Return to Work and Persistent Symptoms Six Months After Viral Meningitis - A Retrospective Single-Centre Cohort Study. — Imishti A, Nissen MJ, Øvrehus A, Larsen L. Infectious Diseases. 2025.
20. Recurrent Herpes Simplex Virus Type 2 Mollaret Meningitis in a Man Living With HIV: A Case Report and Patient-Initiated Episodic Valacyclovir Strategy. — Wakutsu T, Inoue E, Nakamoto T, et al. International Journal of Infectious Diseases : IJID : Official Publication of the International Society for Infectious Diseases. 2026.
21. The Neurotropic Herpes Viruses: Herpes Simplex and Varicella-Zoster. — Steiner I, Kennedy PG, Pachner AR. The Lancet. Neurology. 2007.