Loading...
Viral Pneumonia
1. History
Dr. Lucas Mastropaolo
1. History
- Key HPI questions: Onset and duration of cough (productive vs. dry), dyspnea, fever/chills, pleuritic chest pain, sputum character, hemoptysis
- Symptom characterization: Viral pneumonia typically presents with gradual onset of dry cough, low-grade fever (<38.5°C), myalgias, and malaise, often preceded by upper respiratory prodrome (rhinorrhea, sore throat)[1-2]
- Timing/triggers: Seasonal patterns — RSV and influenza peak in late autumn/winter; rhinovirus in autumn/spring. Ask about sick contacts, recent travel, congregate living[2]
- Associated symptoms: Rhinorrhea, headache, myalgias, anosmia/ageusia (suggestive of COVID-19), wheezing, diarrhea (some viral etiologies)[1]
- Important negatives: Absence of purulent sputum, rigors, and pleuritic chest pain makes bacterial etiology less likely; however, clinical features alone cannot reliably distinguish viral from bacterial pneumonia[2]
2. Alarm Features
- SpO₂ <93% on room air, respiratory rate >30 breaths/min, or severe respiratory distress[3]
- Hemodynamic instability (SBP <90 mmHg) or need for vasopressors[4]
- Altered mental status / new confusion[4-5]
- Multilobar infiltrates on imaging[4]
- Signs of organ dysfunction: oliguria, thrombocytopenia (platelets <100,000), leukopenia (WBC <4,000)[4]
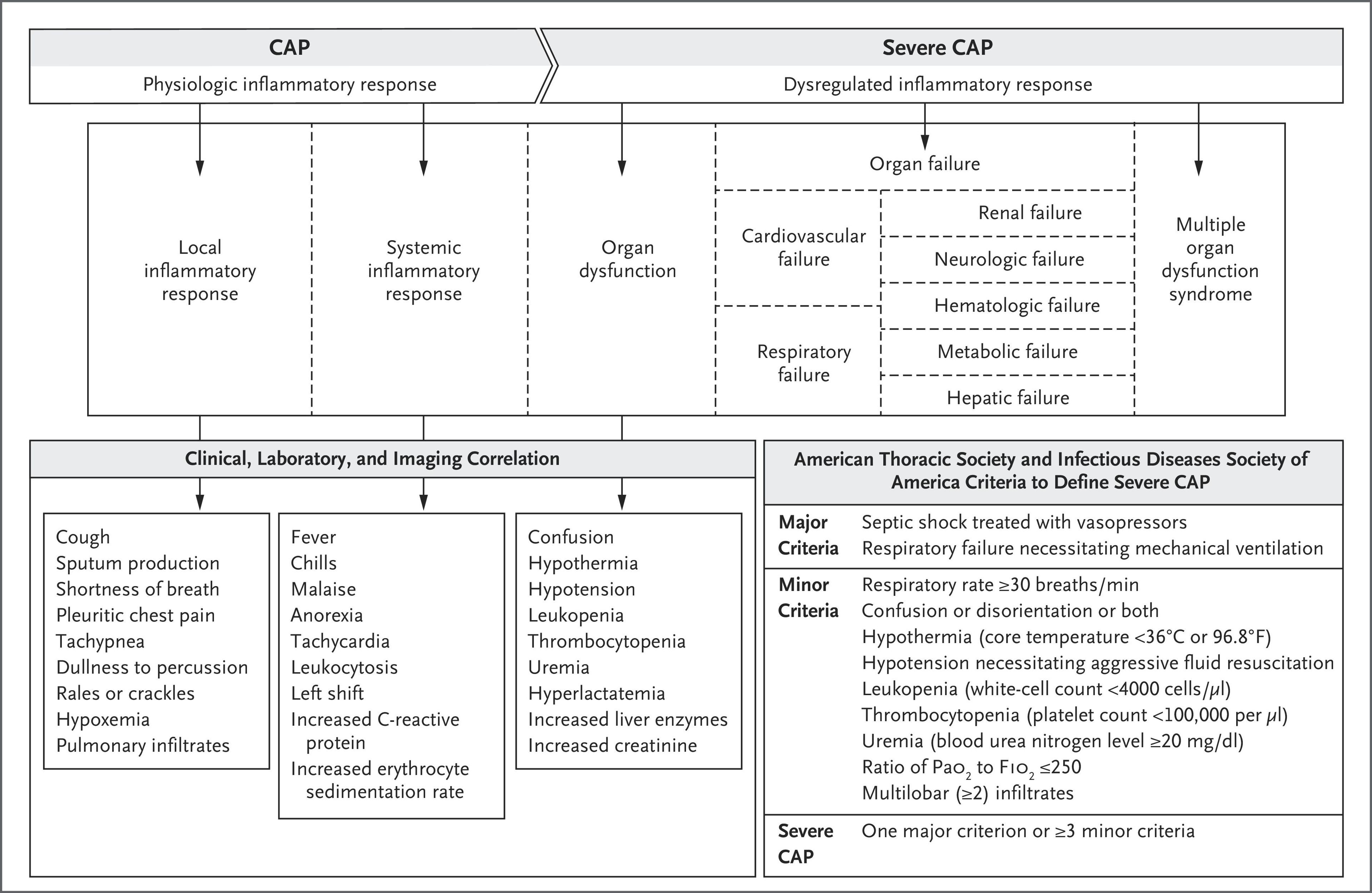
- ATS/IDSA severe CAP criteria: 1 major criterion (mechanical ventilation or septic shock requiring vasopressors) OR ≥3 minor criteria warrants ICU admission[4-5]
- Rapid clinical deterioration despite supportive care
- Hemoptysis or signs of secondary bacterial superinfection (new purulent sputum, rising procalcitonin)
3. Medications
Influenza-specific antivirals
- Oseltamivir 75 mg PO BID × 5 days — first-line for influenza A/B; most benefit within 48 hours of symptom onset, but still recommended in severe/hospitalized cases beyond 48 hours[6-7]
- Baloxavir marboxil (Xofluza) — single-dose oral; FDA-approved for uncomplicated influenza within 48 hours in patients ≥5 years[8]
- Peramivir 600 mg IV single dose — option when oral/inhaled routes not feasible[8]
- Zanamivir inhaled — alternative, especially if oseltamivir resistance suspected[2]
COVID-19 antivirals
- Remdesivir (Veklury) — FDA-approved for hospitalized patients and high-risk outpatients with mild-to-moderate COVID-19[8]
- Nirmatrelvir/ritonavir (Paxlovid) for high-risk outpatients within 5 days of symptom onset
- RSV/other viruses: Largely supportive; ribavirin (aerosolized or IV) considered in immunocompromised patients with RSV, hMPV, or parainfluenza. Cidofovir for severe adenovirus in immunocompromised. Acyclovir for varicella pneumonia[2][4]
- Corticosteroids: Dexamethasone reduces mortality in severe COVID-19 requiring supplemental O₂; role in non-COVID viral pneumonia is controversial and not routinely recommended[1-2]
- Antibiotics: Should be deferred if viral etiology is confirmed and bacterial coinfection is low suspicion (procalcitonin ≤0.25 ng/mL); IDSA suggests antiviral therapy alone in this setting[9]
- Contraindicated/cautions: Avoid unnecessary antibiotics — up to 20% of hospitalized patients receiving antibacterials experience adverse events, and each additional day increases resistant organism risk by ~7%[9]
4. Diet
- Hydration: Adequate oral fluid intake is essential; IV fluids for patients unable to maintain oral intake or with hemodynamic compromise
- Nutritional support: Malnourished and elderly patients benefit from individualized nutritional intervention programs (high protein 1.2–1.5 g/kg/day, energy 25–30 kcal/kg/day), which have been shown to reduce pneumonia readmission rates by up to 77% in malnourished older adults[10-11]
- Micronutrients: Vitamin C supplementation may have modest benefit in patients with deficiency; vitamins C and D, zinc, and selenium highlighted as potentially beneficial in respiratory viral infections, though supplementation has not been linked to prevention[12-13]
- Acute phase: Small, frequent, calorie-dense meals; avoid aspiration risk in patients with altered mental status or severe dyspnea
5. Review of Systems
- Respiratory: Cough (dry vs. productive), dyspnea, wheezing, chest tightness, hemoptysis
- Constitutional: Fever, chills, rigors, fatigue, myalgias, night sweats, weight loss
- ENT: Rhinorrhea, sore throat, anosmia, ageusia, sinus congestion
- GI: Nausea, vomiting, diarrhea (common with COVID-19, adenovirus)
- Cardiac: Chest pain, palpitations (screen for myocarditis complication)
- Neurologic: Confusion, headache, altered mental status
- Skin: Rash (consider measles, varicella, adenovirus)
6. Collateral History and Family History
- Collateral: Vaccination status (influenza, COVID-19, pneumococcal), sick contacts, daycare/school/nursing home exposure, recent travel (MERS-endemic areas, avian influenza regions), occupational exposures (healthcare workers, poultry workers)
- Family history: Immunodeficiency syndromes, household members with respiratory illness
- Social context: Congregate living (shelters, dormitories, military barracks — adenovirus outbreaks), smoking status, substance use, ability to comply with outpatient treatment, home support adequacy[14]
7. Risk Factors
- Age extremes: Elderly (≥65 years) and young children at highest risk[1][9]
- Immunosuppression: Transplant recipients, chemotherapy, HIV/AIDS, chronic corticosteroid use — at risk for severe disease and broader viral etiologies (CMV, HSV, adenovirus reactivation)[4][15]
- Chronic lung disease: COPD, asthma, bronchiectasis, cystic fibrosis[9]
- Smoking[9]
- Comorbidities: Diabetes, heart failure, chronic kidney disease, liver disease, obesity
- Unvaccinated status against influenza, COVID-19, or measles
- Pregnancy
- Nursing home/long-term care facility residence
8. Differential Diagnosis
- Bacterial pneumonia (S. pneumoniae, H. influenzae, S. aureus) — higher fever, rigors, purulent sputum, lobar consolidation, elevated procalcitonin[2][16]
- Atypical pneumonia (Mycoplasma, Chlamydophila, Legionella) — subacute onset, younger patients, extrapulmonary symptoms; procalcitonin may be normal with Mycoplasma[16-17]
- Acute bronchitis — cough without radiographic infiltrate
- Pulmonary embolism — pleuritic chest pain, dyspnea, tachycardia, risk factors for VTE
- Heart failure exacerbation — bilateral infiltrates, elevated BNP, orthopnea, peripheral edema
- Hypersensitivity pneumonitis / eosinophilic pneumonia — exposure history, peripheral eosinophilia
- Fungal pneumonia (Coccidioides, Histoplasma, Pneumocystis) — geographic/immune risk factors[9]
- Tuberculosis — chronic cough, night sweats, weight loss, upper lobe cavitary disease, endemic exposure
- COVID-19 — cannot-miss; test all patients with CAP when circulating in community[9]
9. Past Medical History
- Prior pneumonia episodes and hospitalizations
- Chronic respiratory disease (COPD, asthma, ILD)
- Immunosuppressive conditions or medications
- Prior intubation/mechanical ventilation
- Vaccination history (influenza, COVID-19, pneumococcal, measles)
- Recent antibiotic use (risk for resistant organisms)
- Splenectomy (encapsulated organism risk)
- Swallowing dysfunction or aspiration risk
10. Physical Exam
- Vital signs: Temperature (fever or hypothermia <36°C), tachypnea (RR >30 is a minor severity criterion), tachycardia, hypotension, SpO₂ (critical for severity assessment)[4][18]
- Pulmonary: Crackles/rales, rhonchi, decreased breath sounds, egophony, dullness to percussion (consolidation), wheezing (more common in viral)[16][18]
- General: Assess work of breathing, accessory muscle use, ability to speak in full sentences
- Cardiac: Tachycardia, new murmur, gallop (concern for myocarditis)
- Skin: Cyanosis, mottling (shock), rash (varicella, measles)
- Neurologic: Mental status assessment — confusion is a severity criterion[4]
- Expected vs. concerning: Diffuse bilateral crackles with wheezing more typical of viral; focal consolidation with bronchial breath sounds more suggestive of bacterial, though significant overlap exists[2]
11. Lab Studies
Recommended initial labs (hospitalized patients)
- CBC with differential — lymphopenia common in viral pneumonia; leukocytosis with left shift suggests bacterial[2]
- BMP (BUN, creatinine — severity scoring and organ dysfunction)
- Procalcitonin — low levels (<0.25 ng/mL) support viral etiology and may allow deferral of antibiotics; >0.5 ng/mL supports bacterial infection, though NPV is more reliable than PPV[9][16]
- CRP — elevated in both viral and bacterial, but higher levels (>30 mg/L) strengthen pneumonia diagnosis[18]
- Lactate (if sepsis concern)
- Blood cultures × 2 (before antibiotics if bacterial coinfection suspected)
- Hepatic function panel, troponin (if myocarditis concern)
Microbiologic testing
- Respiratory viral panel (multiplex PCR) — identifies influenza, RSV, SARS-CoV-2, adenovirus, parainfluenza, hMPV, rhinovirus[15][19]
- Rapid influenza and COVID-19 testing for all patients with CAP when these viruses are circulating[9]
- Sputum culture if bacterial coinfection suspected
- Urine antigens (Legionella, S. pneumoniae) in hospitalized patients
- Monitoring: Serial procalcitonin can guide antibiotic de-escalation[16]
12. Imaging
- First-line: Chest X-ray (PA and lateral) — required to confirm pneumonia diagnosis; viral pneumonia classically shows bilateral, diffuse interstitial or ground-glass opacities rather than focal lobar consolidation[20-21]
- CT chest: More sensitive than CXR; indicated when CXR is negative but clinical suspicion remains high, or for complications (abscess, empyema, PE). Ground-glass opacity (GGO) is an independent predictor of viral etiology (OR 4.68)[5][16][21]
- Lung ultrasound: Pooled sensitivity 92%, specificity 89% — superior to CXR; useful at bedside in ED/ICU; dynamic air bronchograms are pathognomonic for pneumonia[5]
- Imaging patterns by virus: Influenza — bilateral GGO and consolidation; COVID-19 — peripheral, bilateral GGO with crazy-paving; RSV — peribronchial thickening, air trapping; adenovirus — multifocal consolidation[20]
- When imaging is unnecessary: Low-risk outpatients with classic viral URI symptoms and no hypoxia or exam findings of consolidation may not require imaging[18]
13. Special Tests
Severity scoring systems
- Low risk: consider outpatient treatment. Patients with a CURB-65 score of 0 or 1 generally have a low risk of mortality and may be suitable for outpatient management.[22-23] However, clinical judgment should be used as additional factors such as hypoxemia, failure of outpatient therapy, or cardiovascular events may necessitate hospitalization.[22]
- PSI (Pneumonia Severity Index): Preferred by ATS/IDSA for site-of-care decisions; classes I–III generally safe for outpatient management[9][14]
- SMART-COP: Predicts need for intensive respiratory or vasopressor support[5]
- Point-of-care testing: Rapid antigen tests for influenza and COVID-19; POCT procalcitonin
- Multiplex respiratory PCR panels — gold standard for viral pathogen identification[15][19]
- Bronchoscopy with BAL: Consider in immunocompromised patients or when upper respiratory sampling is negative but clinical suspicion remains high[19]
14. ECG
- Indications: Obtain ECG in patients with chest pain, tachycardia, palpitations, or hemodynamic instability to evaluate for myocarditis or other cardiac complications
- Viral pneumonia-associated myocarditis findings: Sinus tachycardia, diffuse ST-segment elevation (without reciprocal changes), T-wave inversions (especially inferior/lateral leads), PR depression, low QRS voltage, new conduction abnormalities[24-25]
- Dangerous patterns: New AV block (2nd or 3rd degree), wide QRS ≥120 ms, ventricular tachycardia, prolonged QT — raise suspicion for giant cell myocarditis or fulminant myocarditis requiring urgent cardiology consultation[25-26]
- COVID-19 specific: QT prolongation (especially if on QT-prolonging medications), atrial fibrillation, ventricular arrhythmias[27]
- Sinus tachycardia alone is common and nonspecific in febrile pneumonia patients
15. Assessment
- Viral pneumonia accounts for up to 40% of CAP cases with an identified pathogen; influenza, rhinovirus, and SARS-CoV-2 are the most common viral etiologies[9][17]
- No clinical algorithm reliably distinguishes viral from bacterial pneumonia; the combination of rhinorrhea, GGO on imaging, lower procalcitonin, and lymphocyte-predominant differential favors viral etiology[2][21]
- Severity stratification should use CURB-65 or PSI supplemented by clinical judgment; ATS/IDSA severe CAP criteria guide ICU admission[4-5][16]
- Typical presentation: Gradual onset, dry cough, low-grade fever, bilateral interstitial infiltrates, preceded by URI prodrome
- Atypical/severe presentations: Rapid progression to ARDS (especially influenza H1N1, COVID-19, adenovirus type 14), secondary bacterial superinfection (S. aureus with influenza), invasive aspergillosis in severe viral pneumonia on steroids[5]
- Complications: ARDS, sepsis, myocarditis, secondary bacterial pneumonia, empyema, multiorgan dysfunction
- The following figure illustrates the pathogenesis of CAP from inflammatory response to organ dysfunction, including the ATS/IDSA criteria for severe CAP:
16. Treatment Plan
- Initial stabilization: Supplemental O₂ to maintain SpO₂ ≥92% (≥95% in pregnancy); high-flow nasal cannula or NIV for moderate-severe hypoxemia; intubation for refractory respiratory failure
Antiviral therapy
- Influenza → oseltamivir 75 mg PO BID × 5 days (start empirically if influenza suspected, do not wait for test results in severe illness)[6-7]
- COVID-19 → remdesivir (hospitalized), nirmatrelvir/ritonavir (high-risk outpatients)
- Other viruses → primarily supportive; ribavirin or cidofovir in select immunocompromised patients[2][4]
- Antibiotics: Defer if confirmed viral etiology with low procalcitonin (≤0.25 ng/mL) and low suspicion for bacterial coinfection. If bacterial coinfection cannot be excluded, treat empirically per ATS/IDSA guidelines with early de-escalation when bacterial infection is ruled out[5][9]
- Corticosteroids: Dexamethasone 6 mg daily × 10 days for COVID-19 requiring supplemental O₂; systemic corticosteroids within 24 hours may reduce 28-day mortality in severe CAP. Not routinely recommended for non-COVID viral pneumonia[1-2][9]
- Supportive care: IV fluids (avoid overhydration), antipyretics, VTE prophylaxis in hospitalized patients, nutritional support for malnourished patients[10-11]
17. Disposition
- Outpatient management: CURB-65 score 0–1 or PSI class I–III, SpO₂ >92% on room air, able to tolerate oral medications, adequate home support, no alarm features[9][14][16]
- Admission criteria: CURB-65 ≥2, PSI class IV–V, hypoxemia requiring supplemental O₂, inability to maintain oral intake, significant comorbidities, failed outpatient therapy, inadequate home support or social determinants precluding safe discharge[9][14]
- ICU admission: 1 major ATS/IDSA criterion (vasopressor requirement or mechanical ventilation) OR ≥3 minor criteria[4][28]
- Observation: Consider for borderline cases (CURB-65 = 2, PSI class III) — reassess within 24 hours
- Specialist consultation triggers: Pulmonology for refractory hypoxemia or ARDS; infectious disease for immunocompromised patients or unusual viral pathogens; cardiology if myocarditis suspected
18. Follow Up / Return Precautions
- Follow-up timing: Outpatients should be reassessed within 48–72 hours if not improving; follow-up CXR at 6–8 weeks to confirm radiographic resolution (especially in smokers and patients >50 years to exclude underlying malignancy)
- Clinical stability criteria for discharge: Temperature <37.8°C, HR <100, RR <24, SBP ≥90, SpO₂ ≥90% on room air, normal mental status, tolerating oral intake[17]
- Return precautions — instruct patients to return immediately for:
- Worsening shortness of breath or inability to catch breath at rest
- Persistent or worsening fever >72 hours despite treatment
- Chest pain, lightheadedness, or syncope
- Confusion or altered mental status
- Inability to keep down fluids
- Coughing up blood
- Expected recovery: Fever typically resolves within 2–4 days; cough may persist 2–4 weeks; fatigue may last several weeks. Failure to improve by 72 hours should prompt reassessment for complications, resistant organisms, or alternative diagnoses[17]
- Patient counseling: Hand hygiene, respiratory etiquette, isolation precautions during acute illness, smoking cessation, vaccination (influenza annually, COVID-19, pneumococcal per guidelines)
References
1. Characteristics of Viral Pneumonia in the COVID-19 Era: An Update. — Pagliano P, Sellitto C, Conti V, Ascione T, Esposito S. Infection. 2021.
2. Viral Pneumonia. — Ruuskanen O, Lahti E, Jennings LC, Murdoch DR. Lancet. 2011.
3. Signs and Symptoms to Determine if a Patient Presenting in Primary Care or Hospital Outpatient Settings Has COVID-19. — Struyf T, Deeks JJ, Dinnes J, et al. The Cochrane Database of Systematic Reviews. 2022.
4. Nucleic Acid-Based Testing for Noninfluenza Viral Pathogens in Adults With Suspected Community-Acquired Pneumonia. An Official American Thoracic Society Clinical Practice Guideline. — Evans SE, Jennerich AL, Azar MM, et al. American Journal of Respiratory and Critical Care Medicine. 2021.
5. Community-Acquired Pneumonia. — Reyes LF, Conway Morris A, Serrano-Mayorga C, et al. Lancet. 2025.
6. ERS/ESICM/ESCMID/ALAT Guidelines for the Management of Severe Community-Acquired Pneumonia. — Martin-Loeches I, Torres A, Nagavci B, et al. The European Respiratory Journal. 2023.
7. The Management of Community-Acquired Pneumonia in Infants and Children Older Than 3 Months of Age: Clinical Practice Guidelines by the Pediatric Infectious Diseases Society and the Infectious Diseases Society of America. — Bradley JS, Byington CL, Shah SS, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2011.
8. FDA Orange Book. — FDA Orange Book. 2026.
9. Community-Acquired Pneumonia: A Review. — Vaughn VM, Dickson RP, Horowitz JK, Flanders SA. The Journal of the American Medical Association. 2024.
10. Effect of Nutritional Intervention Programs on Nutritional Status and Readmission Rate in Malnourished Older Adults With Pneumonia: A Randomized Control Trial. — Yang PH, Lin MC, Liu YY, Lee CL, Chang NJ. International Journal of Environmental Research and Public Health. 2019.
11. Management of Disease-Related Malnutrition for Patients Being Treated in Hospital. — Schuetz P, Seres D, Lobo DN, et al. Lancet. 2021.
12. Vitamin C Supplementation for Prevention and Treatment of Pneumonia. — Padhani ZA, Moazzam Z, Ashraf A, et al. The Cochrane Database of Systematic Reviews. 2021.
13. Dietary Recommendations During the COVID-19 Pandemic. — de Faria Coelho-Ravagnani C, Corgosinho FC, Sanches FFZ, et al. Nutrition Reviews. 2021.
14. Diagnosis and Treatment of Adults With Community-Acquired Pneumonia. An Official Clinical Practice Guideline of the American Thoracic Society and Infectious Diseases Society of America. — Metlay JP, Waterer GW, Long AC, et al. American Journal of Respiratory and Critical Care Medicine. 2019.
15. Viral Pneumonia: Etiologies and Treatment. — Dandachi D, Rodriguez-Barradas MC. Journal of Investigative Medicine : The Official Publication of the American Federation for Clinical Research. 2018.
16. Community-Acquired Pneumonia. — File TM, Ramirez JA. The New England Journal of Medicine. 2023.
17. Community-Acquired Pneumonia. — Aliberti S, Dela Cruz CS, Amati F, Sotgiu G, Restrepo MI. Lancet. 2021.
18. Adult Outpatients With Acute Cough Due to Suspected Pneumonia or Influenza: CHEST Guideline and Expert Panel Report. — Hill AT, Gold PM, El Solh AA, et al. Chest. 2019.
19. Society of Critical Care Medicine and the Infectious Diseases Society of America Guidelines for Evaluating New Fever in Adult Patients in the ICU. — O'Grady NP, Alexander E, Alhazzani W, et al. Critical Care Medicine. 2023.
20. Radiographic and CT Features of Viral Pneumonia. — Koo HJ, Lim S, Choe J, et al. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2018.
21. Predictors of Viral Pneumonia in Patients With Community-Acquired Pneumonia. — Kim JE, Kim UJ, Kim HK, et al. PloS One. 2014.
22. Low CURB-65 Is of Limited Value in Deciding Discharge of Patients With Community-Acquired Pneumonia. — Aliberti S, Ramirez J, Cosentini R, et al. Respiratory Medicine. 2011.
23. Performance of the CURB-65 Score in Predicting Critical Care Interventions in Patients Admitted With Community-Acquired Pneumonia. — Ilg A, Moskowitz A, Konanki V, et al. Annals of Emergency Medicine. 2019.
24. Diagnosis and Treatment of Acute Myocarditis: A Review. — Ammirati E, Moslehi JJ. The Journal of the American Medical Association. 2023.
25. 2024 ACC Expert Consensus Decision Pathway on Strategies and Criteria for the Diagnosis and Management Of Myocarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. — Drazner MH, Bozkurt B, Cooper LT, et al. Journal of the American College of Cardiology. 2025.
26. Recognition and Initial Management of Fulminant Myocarditis: A Scientific Statement From the American Heart Association. — Kociol RD, Cooper LT, Fang JC, et al. Circulation. 2020.
27. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. — Gluckman TJ, Bhave NM, Allen LA, et al. Journal of the American College of Cardiology. 2022.
28. Community-Acquired Pneumonia: Updated Recommendations From the ATS and IDSA. — Armstrong C. American Family Physician. 2020.