Loading...
Weber's Syndrome
Weber syndrome is a classic midbrain stroke syndrome characterized by ipsilateral cranial nerve III (oculomotor) palsy with contralateral hemiparesis, caused by a lesion involving the ventral midbr…
Dr. Lucas Mastropaolo
Weber syndrome is a classic midbrain stroke syndrome characterized by ipsilateral cranial nerve III (oculomotor) palsy with contralateral hemiparesis, caused by a lesion involving the ventral midbrain — specifically the oculomotor nerve fascicles and the cerebral peduncle.[1-2] It is most commonly caused by midbrain infarction secondary to occlusion of perforating branches of the posterior cerebral artery (PCA) or upper basilar artery.[1][3-4]
1. History
- Acute onset of diplopia, ptosis, and eye deviation (eye "down and out" on the affected side)
- Simultaneous or rapidly progressive contralateral limb weakness (arm, leg, ± face)
- Timing: sudden onset suggests vascular etiology; subacute onset raises concern for mass lesion, abscess, or demyelination[1][5]
- Ask about preceding TIA symptoms: vertigo, visual changes, dysarthria, ataxia, drop attacks
- Headache (may suggest hemorrhage or mass effect)
- Recent trauma, infection, or immunosuppression (tuberculoma, abscess)[1][6]
- Important negatives: no seizure activity, no altered mental status (unless extensive lesion), no preceding fever
2. Alarm Features
- Rapidly declining consciousness — suggests basilar artery occlusion or expanding hemorrhage[7-8]
- Bilateral motor deficits or quadriparesis — suggests bilateral midbrain or extensive brainstem involvement
- Respiratory irregularity or hemodynamic instability — brainstem compression
- Locked-in syndrome features (preserved consciousness with quadriplegia and anarthria)
- Acute severe headache — hemorrhagic etiology
- Fever with neurological deficits — brainstem abscess or tuberculoma[1][6]
3. Medications
- Acute ischemic stroke: IV alteplase (0.9 mg/kg) within 4.5 hours of symptom onset; tenecteplase is now FDA-approved for acute ischemic stroke. The EXPECTS trial demonstrated benefit of alteplase for posterior circulation stroke up to 24 hours after onset[9-10]
- Antiplatelet therapy: aspirin 325 mg within 24–48 hours if thrombolytics not given
- Anticoagulation if cardioembolic source identified (after acute phase)
- Contraindicated: anticoagulants and antiplatelets within 24 hours of thrombolysis
- Statin therapy for secondary prevention
- If tuberculoma: antitubercular therapy ± systemic steroids[1]
- If Behçet's disease: corticosteroids[11]
4. Diet
- NPO initially until dysphagia screening is completed[12]
- Heart-healthy/DASH diet for long-term secondary stroke prevention
- Sodium restriction if hypertensive
- Adequate hydration to maintain euvolemia; avoid dehydration which may worsen ischemia
5. Review of Systems
- Neurologic: vision changes, diplopia, ptosis, facial droop, limb weakness/numbness, dysarthria, dysphagia, ataxia, vertigo
- Cardiovascular: palpitations, chest pain (atrial fibrillation as embolic source)
- Constitutional: fever, weight loss, night sweats (tuberculosis, malignancy)[1][5]
- Rheumatologic: oral/genital ulcers, skin lesions (Behçet's disease)[11]
- Infectious: recent illness, immunosuppression
6. Collateral History and Family History
- Time last known well — critical for thrombolytic eligibility
- Witnessed symptom onset vs. wake-up stroke
- Baseline functional status (pre-morbid modified Rankin Scale)
- Family history of stroke, coagulopathy, or connective tissue disorders
- Social history: smoking, alcohol use, illicit drug use (cocaine, amphetamines)
- History of tuberculosis exposure or endemic area travel[1]
7. Risk Factors
- Hypertension — most significant risk factor for small-vessel disease and lipohyalinosis causing midbrain lacunar infarcts[13]
- Diabetes mellitus
- Atrial fibrillation (cardioembolic source)[4][14]
- Hyperlipidemia
- Smoking
- Intracranial atherosclerotic disease — particularly relevant in Asian populations[15]
- Basilar artery stenosis[3]
- Coagulopathy (e.g., hemophilia — reported cause of midbrain hemorrhage leading to Weber syndrome)[16]
- Vasculitis (Behçet's disease, SLE)[5][11]
8. Differential Diagnosis
- Benedikt syndrome: CN III palsy + contralateral tremor/involuntary movements (red nucleus involvement rather than cerebral peduncle)[2]
- Claude syndrome: CN III palsy + contralateral ataxia + tremor (superior cerebellar peduncle + red nucleus)[2]
- Nothnagel syndrome: CN III palsy + ipsilateral cerebellar ataxia[2]
- Posterior communicating artery aneurysm: isolated CN III palsy (pupil-involving) without hemiparesis
- Uncal herniation: CN III palsy with contralateral hemiparesis — mimics Weber syndrome but from supratentorial mass effect
- Cavernous sinus lesion: CN III palsy ± other cranial neuropathies (IV, V1, V2, VI)
- Myasthenia gravis: fluctuating ptosis/diplopia without hemiparesis
- Brainstem tumor (glioma, lymphoma, metastasis)[5]
- Demyelinating disease (MS, NMOSD, MOGAD)[5]
9. Past Medical History
- Prior stroke or TIA (especially posterior circulation)
- Hypertension, diabetes, hyperlipidemia, atrial fibrillation
- Known intracranial atherosclerotic disease or vertebrobasilar stenosis
- Bleeding disorders[16]
- Autoimmune/inflammatory conditions (Behçet's, sarcoidosis, SLE)[5][11]
- History of tuberculosis[1]
- Prior cardiac surgery or prosthetic valves
10. Physical Exam
- Vital signs: hypertension (permissive in acute stroke unless >220/120), tachycardia (atrial fibrillation), fever (infectious etiology)
Eyes (ipsilateral to lesion)
- Ptosis
- Eye deviated "down and out" (lateral strabismus with depression)
- Dilated, fixed pupil (if complete CN III palsy)
- Impaired adduction, elevation, and depression of the eye
Motor (contralateral to lesion)
- Upper motor neuron pattern hemiparesis (face, arm, leg)
- Increased tone, hyperreflexia, positive Babinski sign
- Cerebellar exam: typically normal unless lesion extends
- Assess for dysarthria and dysphagia
- NIHSS for stroke severity scoring[12][17]
11. Lab Studies
- Stat glucose (required before thrombolysis)[17]
- CBC, BMP, coagulation studies (PT/INR, aPTT)
- Troponin (concurrent cardiac event)
- Lipid panel, HbA1c
- ESR/CRP if vasculitis or infection suspected
- Blood cultures if febrile
- Hypercoagulability workup in young patients without traditional risk factors
- TB testing (QuantiFERON, PPD) if tuberculoma suspected[1]
12. Imaging
- Non-contrast CT head: first-line to exclude hemorrhage; often normal in early midbrain infarction[18]
- MRI brain with DWI: gold standard — demonstrates restricted diffusion in the ventral midbrain (cerebral peduncle). MRI is far more sensitive than CT for posterior fossa lesions[3][19-20]
- CT angiography (CTA) or MR angiography (MRA): evaluate for posterior cerebral artery occlusion, basilar artery stenosis/occlusion, or vertebral artery disease[4][21]
- CT perfusion: may help identify salvageable tissue in extended time windows[10]
- Imaging is unnecessary to repeat if the diagnosis is established and the patient is clinically stable
13. Special Tests
- NIHSS: standard stroke severity assessment; note that NIHSS has limitations in posterior circulation strokes[17]
- pc-ASPECTS (Posterior Circulation ASPECTS): 10-point scale assessing extent of posterior circulation ischemia on CT/MRI[15][22]
- Echocardiography (TTE ± TEE): evaluate for cardioembolic source (PFO, valvular disease, intracardiac thrombus)
- Telemetry/Holter monitor: screen for paroxysmal atrial fibrillation
- Carotid/vertebral duplex ultrasound or dedicated vessel imaging
- Lumbar puncture: if infectious or inflammatory etiology suspected[11]
14. ECG
Obtain 12-lead ECG to evaluate for
- Atrial fibrillation/flutter — most common cardioembolic source
- Acute MI (concurrent event)
- Left ventricular hypertrophy (chronic hypertension)
- Continuous cardiac monitoring for at least 24 hours recommended[12]
15. Assessment
Weber syndrome is a crossed brainstem syndrome localizing to the ventral midbrain, where the oculomotor nerve fascicles traverse the cerebral peduncle.[2] The most common etiology is ischemic stroke from occlusion of paramedian perforating branches of the PCA or upper basilar artery.[1][3-4] Less common causes include hemorrhage, tuberculoma, neoplasm, demyelination, and vasculitis.[1][5][11][16] Classic brainstem syndromes like Weber syndrome rarely occur in their pure form.[21] The prognosis of isolated midbrain infarction is generally favorable, except in cases of bilateral involvement.[19]
16. Treatment Plan
- Acute stabilization: ABCs, IV access, cardiac monitoring, continuous pulse oximetry
- Thrombolysis: IV alteplase (0.9 mg/kg, max 90 mg; 10% bolus, remainder over 60 min) if within 4.5 hours of symptom onset. Alteplase may benefit posterior circulation stroke patients up to 24 hours after onset based on the EXPECTS trial[10]
- Endovascular thrombectomy: for large-vessel occlusion (basilar artery) within 24 hours per AHA/ASA 2026 guidelines; ATTENTION and BAOCHE trials demonstrated superiority of EVT over medical management[15][22]
- Blood pressure management: permissive hypertension (do not treat unless >220/120 if no thrombolysis); if thrombolysis given, maintain BP <185/110 pre-treatment and <180/105 post-treatment[12]
- Antiplatelet therapy: aspirin 325 mg within 24–48 hours (if thrombolytics not administered)
- Glucose management: target 140–180 mg/dL[12]
- DVT prophylaxis: intermittent pneumatic compression in immobile patients[12]
- Dysphagia screening before oral intake[12]
- Secondary prevention: statin, antihypertensives, anticoagulation if AF identified
- Non-vascular etiologies: treat underlying cause (antitubercular therapy, corticosteroids for Behçet's, antibiotics for abscess)[1][6][11]
17. Disposition
- All patients with Weber syndrome require admission — typically to a stroke unit or neuro-ICU[12][23]
- ICU admission criteria: declining consciousness, respiratory compromise, large infarct burden, post-thrombolysis/thrombectomy monitoring, hemodynamic instability
- Neurology consultation mandatory; neurosurgery consultation if hemorrhagic etiology or mass lesion
- Transfer to a comprehensive stroke center if EVT capability is unavailable locally[17]
- Patients with bilateral brainstem infarction or basilar artery occlusion carry significantly worse prognosis[4][14]
18. Follow Up / Return Precautions
- Inpatient: serial neurological assessments (NIHSS trending), repeat imaging at 24 hours post-thrombolysis, cardiac monitoring for ≥24 hours
- Post-discharge follow-up: neurology within 1–2 weeks; ophthalmology if persistent CN III palsy; cardiology if AF or cardiac source identified
- Rehabilitation: early physical/occupational/speech therapy referral
- Return precautions: new or worsening weakness, vision changes, difficulty speaking or swallowing, severe headache, altered consciousness
- Expected course: prognosis for isolated midbrain infarction is generally good; CN III palsy may partially or fully recover over weeks to months; contralateral hemiparesis recovery depends on infarct extent[19]
- Long-term: optimize vascular risk factors, medication adherence, lifestyle modification
- Relevant images 3 items
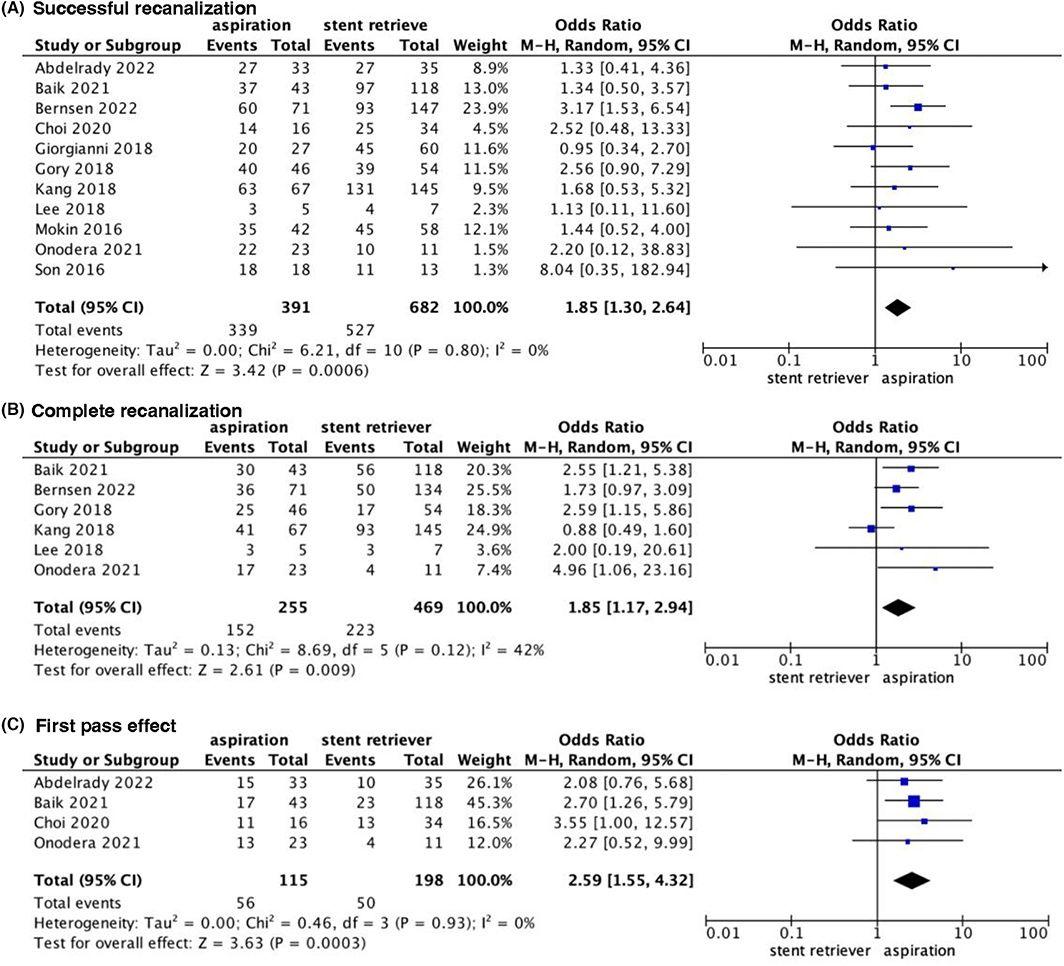
- Forest plot for Forest plot for successful recanalization, complete recanalization, and first‐pass effect.
- CNS Neuroscience & Therapeutics January 31, 2023
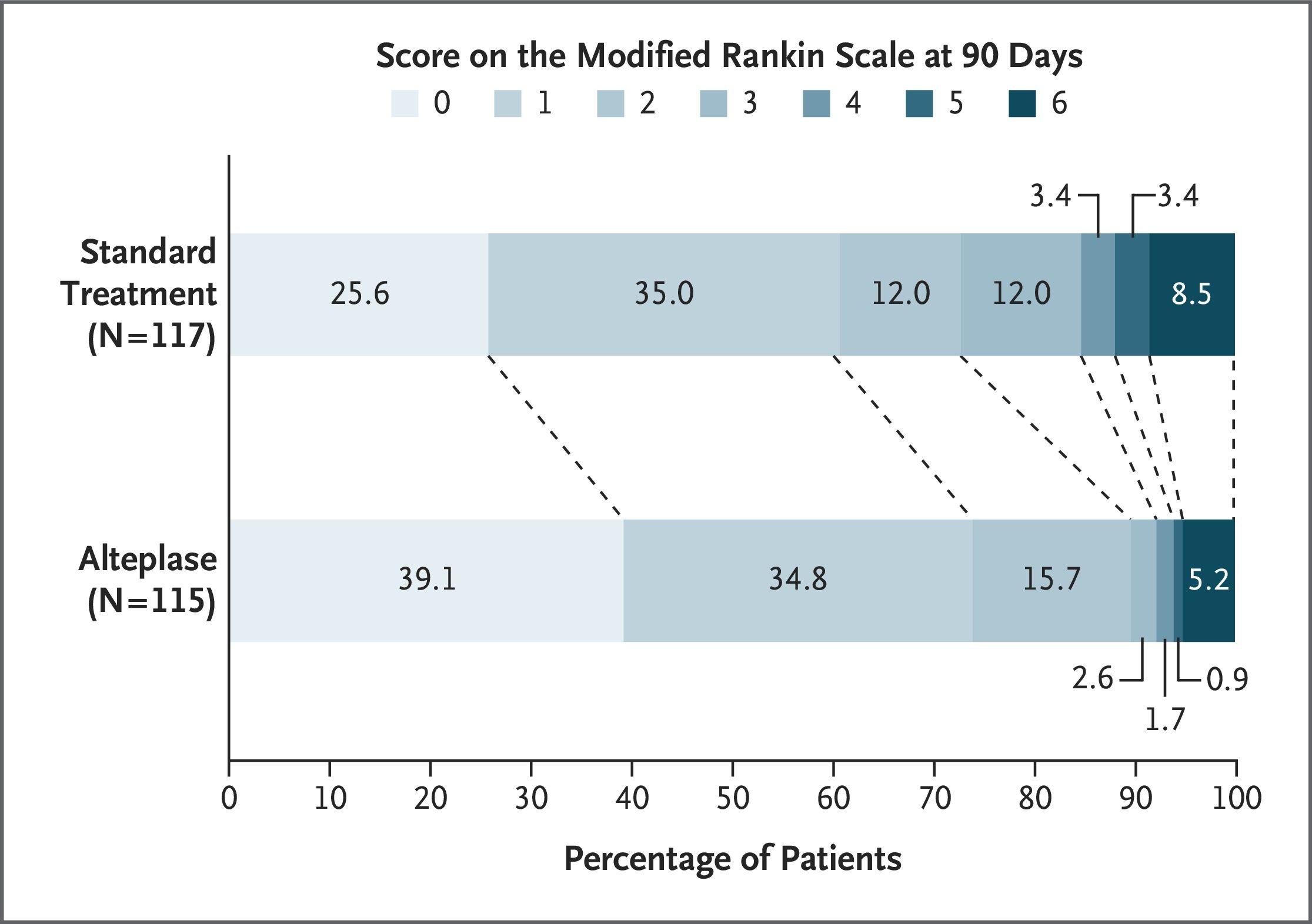
- Distribution of Scores on the Modified Rankin Scale at 90 Days (Intention-to-Treat Population).
- NEJM April 2, 2025
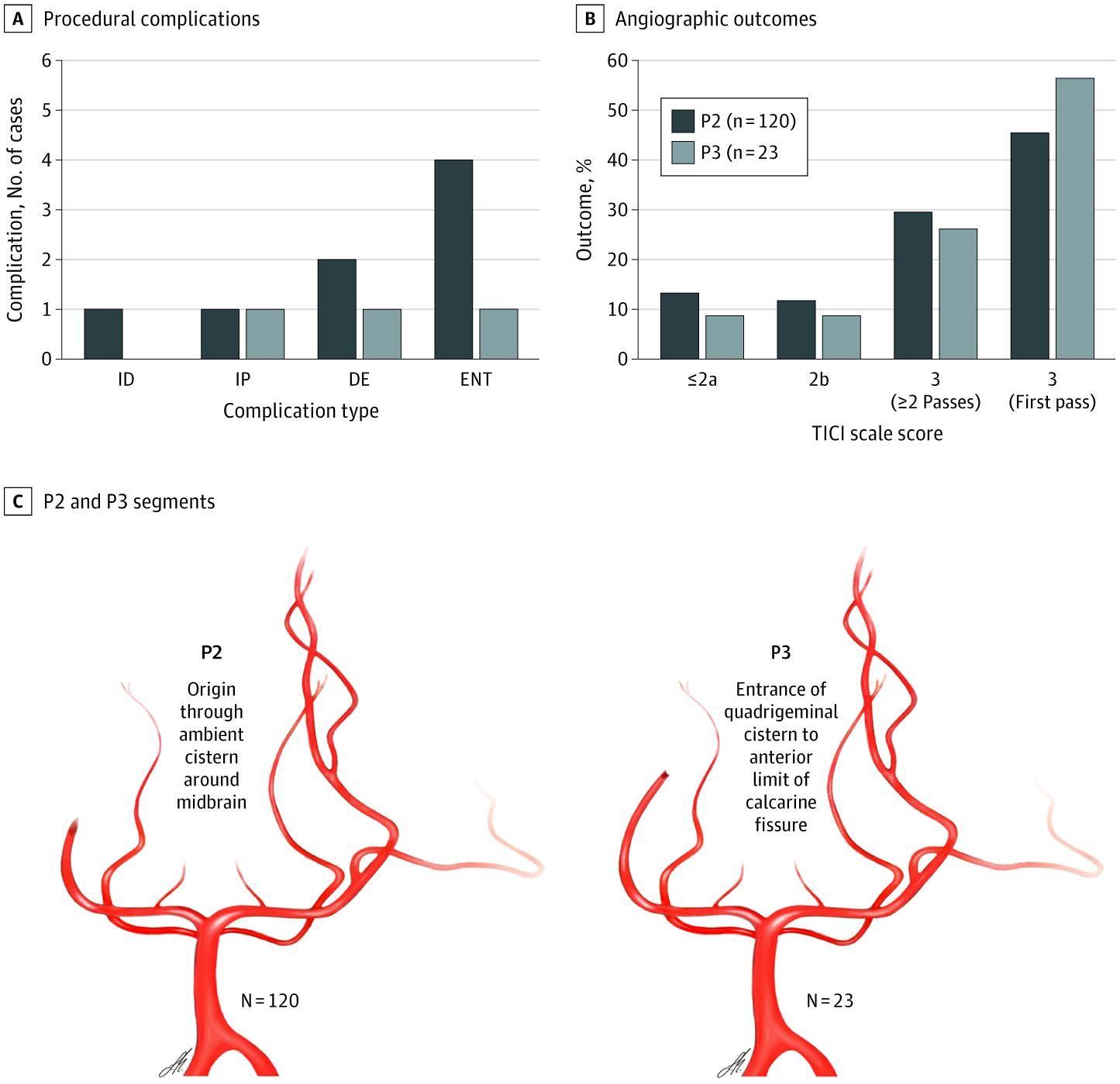
- Endovascular Complications and Angiographic Outcomes Stratified by Vessel Segment
- JAMA Neurol March 31, 2021
References
1. Weber Syndrome Secondary to Brain Stem Tuberculoma. — Parija S, Lalitha CS, Naik S. Indian Journal of Ophthalmology. 2018.
2. Pearls & Oy-Sters: Looking Up the Anatomy of Looking Up. — Abid MB, Soon D, Rathakrishnan R, et al. Neurology. 2016.
3. Pure Midbrain Infarction: Clinical Syndromes, MRI, and Etiologic Patterns. — Bogousslavsky J, Maeder P, Regli F, Meuli R. Neurology. 1994.
4. Mesencephalic and Associated Posterior Circulation Infarcts. — Kumral E, Bayulkem G, Akyol A, et al. Stroke. 2002.
5. Clinical Reasoning: A 60-Year-Old Man With Rapidly Progressive Left Hemibody Weakness and Vision Loss. — Rock M, Shipley SC, Little JN, Berger JR, Xu DJ. Neurology. 2025.
6. Ethmoid Abscess With Findings Simulating Weber Syndrome. — Luo JJ, Jacobson M, Kamal AK, Azizi SA. Neurology. 2005.
7. Basilar Artery Occlusion. — Mattle HP, Arnold M, Lindsberg PJ, Schonewille WJ, Schroth G. The Lancet. Neurology. 2011.
8. Endovascular Management of Acute Stroke. — Nguyen TN, Abdalkader M, Fischer U, et al. Lancet. 2024.
9. FDA Orange Book. — FDA Orange Book. 2026.
10. Alteplase for Posterior Circulation Ischemic Stroke at 4.5 to 24 Hours. — Yan S, Zhou Y, Lansberg MG, et al. The New England Journal of Medicine. 2025.
11. A Case of Behçet's Disease With Weber's Syndrome. — Emura A, Takeuchi A, Hashimoto T, et al. The Journal of Rheumatology. 1986.
12. Acute Ischemic Stroke. — Powers WJ. The New England Journal of Medicine. 2020.
13. Clinical Reasoning: A 74-Year-Old Woman Presenting With Monocular Ptosis and Binocular Diplopia. — Liu Z, Zhang WW, Dai P, et al. Neurology. 2023.
14. Midbrain Infarction: Associations and Aetiologies in the New England Medical Center Posterior Circulation Registry. — Martin PJ, Chang HM, Wityk R, Caplan LR. Journal of Neurology, Neurosurgery, and Psychiatry. 1998.
15. 2026 Guideline for the Early Management of Patients With Acute Ischemic Stroke: A Guideline From the American Heart Association/American Stroke Association. — Prabhakaran S, Gonzalez NR, Zachrison KS, et al. Stroke. 2026.
16. Weber Syndrome Caused by Intracerebral Hemorrhage in a Hemophiliac Boy. — Mizuguchi M, Kano H, Narita M, Chen RF, Bessho F. Brain & Development. 1993.
17. Care of the Patient With Acute Ischemic Stroke (Prehospital and Acute Phase of Care): Update to the 2009 Comprehensive Nursing Care Scientific Statement: A Scientific Statement From the American Heart Association. — Ashcraft S, Wilson SE, Nyström KV, et al. Stroke. 2021.
18. Acute Stroke Diagnosis. — Choi EY, Nieves GA, Jones DE. American Family Physician. 2022.
19. Pure Midbrain Infarction: Clinical, Radiologic, and Pathophysiologic Findings. — Kim JS, Kim J. Neurology. 2005.
20. Teaching NeuroImages: Stroke Presenting With Isolated Superior Branch of Cranial Nerve III Palsy. — Kapoor G, Shah YD, Libman R. Neurology. 2020.
21. Posterior Circulation Ischaemic Stroke and Transient Ischaemic Attack: Diagnosis, Investigation, and Secondary Prevention. — Markus HS, van der Worp HB, Rothwell PM. The Lancet. Neurology. 2013.
22. Trial of Thrombectomy 6 to 24 Hours after Stroke Due to Basilar-Artery Occlusion. — Jovin TG, Li C, Wu L, et al. The New England Journal of Medicine. 2022.
23. Recommendations for the Management of Cerebral and Cerebellar Infarction With Swelling: A Statement for Healthcare Professionals From the American Heart Association/American Stroke Association. — Wijdicks EF, Sheth KN, Carter BS, et al. Stroke. 2014.
24. Aspiration versus stent retriever for posterior circulation stroke: A meta‐analysis. — Guo X, Xiong Y, Huang X, et al. CNS Neuroscience & Therapeutics. 2023.
25. Thrombectomy for Primary Distal Posterior Cerebral Artery Occlusion Stroke: The TOPMOST Study. — Meyer L, Stracke CP, Jungi N, et al. JAMA Neurology. 2021.