Loading...
Wolff-Parkinson-White Syndrome
Wolff-Parkinson-White (WPW) syndrome is defined by the combination of ventricular preexcitation on ECG (delta wave, short PR interval, widened QRS) and cardiac symptoms or documented arrhythmias, c…
Dr. Lucas Mastropaolo
Wolff-Parkinson-White (WPW) syndrome is defined by the combination of ventricular preexcitation on ECG (delta wave, short PR interval, widened QRS) and cardiac symptoms or documented arrhythmias, caused by an accessory pathway (AP) that bypasses the AV node.[1-2] Prevalence of the WPW ECG pattern is 0.1–0.3% in the general population.[1][3] The critical danger is rapid anterograde conduction during atrial fibrillation, which can degenerate into ventricular fibrillation and sudden cardiac death (SCD).[2][4]
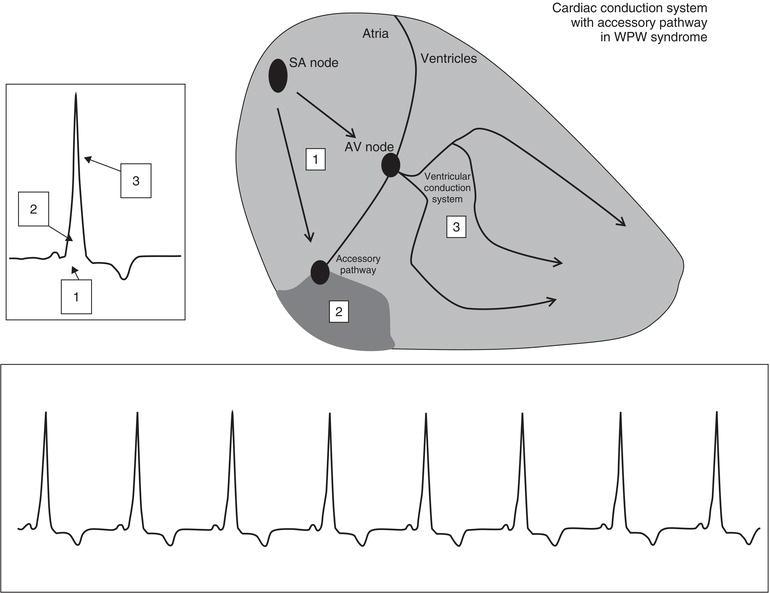
The following figure illustrates the classic ECG triad of WPW — shortened PR interval, delta wave, and widened QRS — along with the anatomical basis of the accessory pathway:
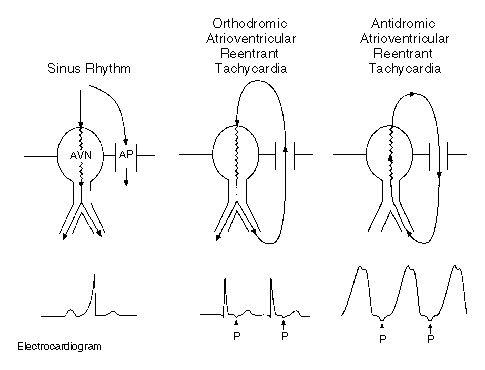
The mechanism of atrioventricular reentrant tachycardia (AVRT) in WPW, including orthodromic and antidromic circuits, is shown below:
1. History
- Palpitations — sudden onset, rapid, regular; often described as "racing heart" or "fluttering"
- Onset and offset — characteristically abrupt (paroxysmal), distinguishing AVRT from sinus tachycardia
- Syncope or presyncope — suggests hemodynamic compromise or rapid ventricular rates; a red flag for high-risk pathway[3]
- Chest discomfort or dyspnea during episodes
- Duration and frequency of episodes; prior ED visits or cardioversions
- Triggers — exercise, caffeine, alcohol, emotional stress, catecholamine surges[3]
- Age at first episode — risk of life-threatening events (LTEs) is "front-loaded" in the young, with SCD risk higher in children (1.93/1000 person-years) vs. adults (0.86/1000 person-years)[3]
- Important negatives — absence of structural heart disease symptoms, no family history of sudden death
2. Alarm Features
- Syncope — independent predictor of adverse outcomes[3]
- Cardiac arrest or aborted SCD — may be the sentinel event, especially in children (65% of pediatric LTEs)[3]
- Irregular wide-complex tachycardia — suggests preexcited AF, which can degenerate to VF[2][4]
- Heart rates >250 bpm during tachycardia
- Hemodynamic instability — hypotension, altered mental status, signs of shock
- Male sex, age <30 years — additional risk factors for adverse outcomes[3]
3. Medications
Contraindicated in preexcited AF (Class III: Harm)
- Verapamil, diltiazem (non-dihydropyridine CCBs)
- Adenosine
- Digoxin
- IV amiodarone
- Beta-blockers
- These agents block AV nodal conduction without prolonging AP refractoriness, which can accelerate ventricular rate via the AP and precipitate VF.[7-9]
Safe for acute preexcited AF (hemodynamically stable)
- IV procainamide or IV ibutilide — slow AP conduction and may terminate AF[7]
- Safe for orthodromic AVRT (narrow-complex, no preexcitation on resting ECG):
- Vagal maneuvers → adenosine → IV diltiazem/verapamil/beta-blockers[10]
Chronic pharmacotherapy (if ablation deferred)
- Flecainide, propafenone, sotalol, or amiodarone (oral) may be used[11]
- Beta-blockers (e.g., propranolol, atenolol) have been used as first-line in pediatric patients too young for ablation[11]
4. Diet
- Caffeine and alcohol may trigger episodes of SVT or AF; moderation is generally advised
- Stimulant-containing supplements (energy drinks, pre-workout formulas) should be avoided
- No specific long-term dietary management beyond avoidance of triggers
5. Review of Systems
- Cardiovascular — palpitations, chest pain, syncope, exercise intolerance, dyspnea
- Neurological — lightheadedness, presyncope, loss of consciousness
- Psychiatric — anxiety (often comorbid with recurrent palpitations)
- Musculoskeletal — episodes of muscle weakness (consider hypokalemic periodic paralysis if associated)[12]
- Developmental — intellectual disability (consider Danon disease if WPW + HCM in a young male)[12]
6. Collateral History and Family History
- Family history of sudden cardiac death, especially in young relatives
- Family history of WPW — approximately 3% of affected individuals have a symptomatic first-degree relative[13]
- Familial HCM — WPW + HCM + progressive conduction disease suggests PRKAG2 mutation[12][14]
- Congenital heart disease in family — Ebstein anomaly is the most commonly associated structural defect[3][12]
- Genetic syndromes — Pompe disease, Danon disease, tuberous sclerosis complex[12][15]
7. Risk Factors
- Male sex[3]
- Age <30 years — risk is front-loaded in the young[3]
- Symptomatic tachycardia — higher risk of LTEs compared to asymptomatic preexcitation[3][16]
- Multiple accessory pathways[2][4]
- Short AP refractory period (<250 ms)[1][4]
- Ebstein anomaly — APs present in ≥10% of patients[12][17]
- PRKAG2 gene variants — associated with WPW + HCM + conduction disease[12][14]
- Congenital heart disease — Ebstein anomaly, congenitally corrected TGA[3]
8. Differential Diagnosis
- AVNRT — most common SVT; narrow-complex, no delta wave in sinus rhythm; pseudo-R' in V1 or pseudo-S in inferior leads
- Atrial flutter/fibrillation — preexcited AF can mimic polymorphic VT; irregular wide-complex tachycardia is the hallmark
- Ventricular tachycardia — antidromic AVRT produces wide-complex tachycardia that must be distinguished from VT; when in doubt, treat as VT[6]
- Mahaim fiber tachycardia — atriofascicular pathway producing LBBB-morphology wide-complex tachycardia
- Lown-Ganong-Levine syndrome — short PR without delta wave (enhanced AV nodal conduction)
- Fasciculoventricular pathway — mimics WPW on ECG but does not participate in reentrant circuits and is benign; does NOT require ablation[3]
- Hypertrophic cardiomyopathy — can produce pseudo-preexcitation patterns on ECG
9. Past Medical History
- Prior episodes of SVT, AF, or cardiac arrest
- Previous catheter ablation attempts (recurrence rate ~11.6% for RF ablation of septal pathways)[18]
- Known congenital heart disease (Ebstein anomaly, corrected TGA)[3][19]
- Cardiomyopathy — tachycardia-induced or dyssynchrony-related (especially right-sided pathways)[3]
- Glycogen storage disorders (Pompe, Danon, PRKAG2-related)[12]
10. Physical Exam
- Often entirely normal between episodes
During tachycardia
- Tachycardia (regular in AVRT, irregular in preexcited AF)
- Hypotension if hemodynamically compromised
- Cannon A waves in JVP (during AVRT with simultaneous atrial and ventricular contraction)
- Signs of heart failure if tachycardia-induced cardiomyopathy
Structural heart disease clues
- Tricuspid regurgitation murmur, widely split S1 (Ebstein anomaly)
- Systolic murmur at LLSB (HCM)
- Hepatomegaly, developmental delay (storage diseases)
11. Lab Studies
- Routine labs — BMP (electrolytes, particularly K+ and Mg2+), CBC
- Troponin — if chest pain or prolonged tachycardia
- TSH — to exclude hyperthyroidism as a trigger for AF/SVT
- BNP/NT-proBNP — if concern for heart failure or cardiomyopathy
- Genetic testing — indicated only when WPW is combined with HCM and/or progressive conduction disease (PRKAG2 testing)[12]
- Labs are primarily used to rule out metabolic triggers and dangerous mimics, not to diagnose WPW itself
12. Imaging
- Echocardiography — recommended in all patients with WPW pattern on ECG to evaluate for structural heart disease (Ebstein anomaly, HCM, LV dysfunction from dyssynchrony)[3]
- Cardiac MRI — if echocardiography is inconclusive or concern for cardiomyopathy
- Imaging is not required for diagnosis of WPW itself (ECG is diagnostic)
- CT coronary angiography — generally not indicated unless evaluating for other pathology
13. Special Tests
- Electrophysiology study (EPS) — gold standard for risk stratification and pathway characterization[4]
- High-risk features: SPERRI ≤250 ms, APERP ≤240 ms, inducible AVRT, multiple APs[3]
- Recommended for all symptomatic patients and for risk stratification in asymptomatic patients, especially children, athletes, and high-risk occupations[3-4]
- Exercise stress testing — abrupt loss of preexcitation during exercise suggests a longer AP refractory period and lower risk[3-4]
- Ambulatory (Holter) monitoring — intermittent preexcitation may suggest lower risk, though this is imperfect[3-4]
- Adenosine testing — for right anteroseptal pathways to rule out fasciculoventricular pathway before ablation[3]
14. ECG
Classic WPW triad in sinus rhythm
- Short PR interval (<120 ms) — impulse bypasses AV nodal delay
- Delta wave — initial slurring of QRS upstroke from early ventricular activation via AP
- Widened QRS (>120 ms) — fusion beat from AP and normal conduction[5]
Tachycardia patterns
- Orthodromic AVRT — narrow-complex tachycardia (anterograde via AV node, retrograde via AP); delta wave disappears during tachycardia; retrograde P waves may be visible after QRS[6]
- Antidromic AVRT — wide-complex tachycardia (anterograde via AP, retrograde via AV node); maximally preexcited, broad QRS; must distinguish from VT[6]
- Preexcited AF — irregularly irregular wide-complex tachycardia with varying QRS morphology; the most dangerous arrhythmia in WPW[2][7]
Dangerous ECG patterns
- Irregular wide-complex tachycardia at very rapid rates (>250 bpm)
- Shortest preexcited R-R interval <250 ms during AF → high risk for VF[2-4]
Low-risk features
- Intermittent preexcitation on resting ECG or Holter (though not absolute)[3]
- Abrupt loss of delta wave during exercise[4]
15. Assessment
- WPW is usually an isolated abnormality in a structurally normal heart[3]
- WPW pattern (preexcitation on ECG without symptoms) vs. WPW syndrome (preexcitation + arrhythmias/symptoms) — an important distinction for risk stratification[1][3]
- Lifetime SCD risk approaches up to 4%, with recent estimates of ~2%[4][20]
- SCD can be the first manifestation in ~50% of cases[4]
- Risk is highest in the first two decades of life[2-3]
- Complications: VF/SCD, tachycardia-induced cardiomyopathy, preexcitation-induced cardiomyopathy (dyssynchrony, especially right-sided pathways)[3]
16. Treatment Plan
- Acute management — Hemodynamically unstable (any arrhythmia):
- Synchronized cardioversion (50–100 J initial)[7][10][18]
- Acute management — Orthodromic AVRT (narrow-complex), hemodynamically stable:
- Vagal maneuvers (Valsalva, carotid sinus massage)[10]
- IV adenosine 6 mg → 12 mg (effective in 90–95%)[10][21]
- Caution: adenosine may precipitate AF; have defibrillator ready[21]
- IV diltiazem/verapamil or beta-blockers if no preexcitation on resting ECG[2][10]
- Acute management — Preexcited AF (wide-complex, irregular), hemodynamically stable:
- IV procainamide or IV ibutilide[7]
- AVOID: adenosine, verapamil, diltiazem, digoxin, IV amiodarone, beta-blockers[7-8]
Acute management — Antidromic AVRT (wide-complex, regular)
- Antiarrhythmic agents (procainamide, ibutilide) preferred over AV nodal blockers[18]
- Cardioversion if unstable[18]
Definitive treatment
- Catheter ablation — first-line therapy for WPW syndrome (Class I recommendation)[3][7]
- Success rate >90%, major complication rate <1%[3]
- 0.3% risk of AV block requiring pacemaker[18]
- Cryoablation reasonable for anteroseptal/midseptal pathways to reduce risk of AV node injury[3]
- RF ablation recurrence ~11.6% over ~37 months for septal pathways[18]
- Ablation reduced arrhythmic events by 92% (RR 0.08) in high-risk patients over 5 years[18]
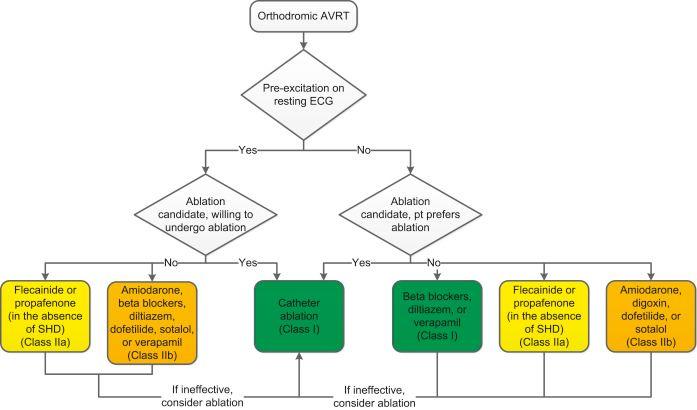
- The ACC/AHA/HRS 2015 SVT guideline provides the following algorithm for ongoing management of orthodromic AVRT:
17. Disposition
Admission criteria
- Hemodynamic instability or cardiac arrest
- Preexcited AF requiring monitoring after cardioversion
- Recurrent tachycardia refractory to acute treatment
- New diagnosis with syncope or high-risk features pending EP consultation
Discharge criteria
- Stable orthodromic AVRT that converts with vagal maneuvers or adenosine
- Known WPW with brief, self-limited episode and established follow-up
- Asymptomatic WPW pattern discovered incidentally (with outpatient referral)
Specialist consultation triggers
- All patients with WPW pattern or syndrome should be referred to electrophysiology[3][22]
- Urgent EP consultation for syncope, cardiac arrest, or preexcited AF
- Pediatric electrophysiology referral for all children with WPW pattern, regardless of symptoms[22]
18. Follow Up / Return Precautions
- Post-ablation: cardiology follow-up for at least 1 year to evaluate for AP recurrence[3]
- If ablation deferred or unsuccessful: periodic cardiology follow-up regardless of symptoms[3]
Return precautions — return immediately for
- Recurrent palpitations, syncope, or presyncope
- Chest pain or dyspnea
- Sensation of irregular or very rapid heartbeat
Patient counseling
- Avoid known triggers (caffeine, alcohol, stimulants)
- Teach vagal maneuvers (Valsalva, bearing down) for self-termination of episodes
- Carry a medical alert card or bracelet noting WPW and contraindicated medications
- Expected recovery after ablation: 1–2 weeks activity restriction, then return to full activity[3]
- Athletes: return to play is recommended during evaluation if asymptomatic; after successful ablation, return to all sports after a 1–2 week healing period[3]
References
1. Sudden Cardiac Death in Young Athletes: JACC State-of-the-Art Review. — Finocchiaro G, Westaby J, Sheppard MN, Papadakis M, Sharma S. Journal of the American College of Cardiology. 2024.
2. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Page RL, Joglar JA, Caldwell MA, et al. Heart Rhythm. 2016.
3. 2024 HRS Expert Consensus Statement on Arrhythmias in the Athlete: Evaluation, Treatment, and Return to Play. — Lampert R, Chung EH, Ackerman MJ, et al. Heart Rhythm. 2024.
4. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) Expert Consensus on Risk Assessment in Cardiac Arrhythmias: Use the Right Tool for the Right Outcome, in the Right Population. — Nielsen JC, Lin YJ, de Oliveira Figueiredo MJ, et al. Heart Rhythm. 2020.
5. Wolff–Parkinson–White Syndrome. — William J. Brady The Electrocardiagram in Emergency and Acute Care. 2023.
6. Supraventricular Tachycardia. — Ganz LI, Friedman PL. The New England Journal of Medicine. 1995.
7. 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. — Writing Committee Members, Joglar JA, Chung MK, et al. Journal of the American College of Cardiology. 2024.
8. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. — January CT, Wann LS, Alpert JS, et al. Journal of the American College of Cardiology. 2014.
9. 2014 AHA/ACC/HRS Guideline for the Management of Patients With Atrial Fibrillation: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. — January CT, Wann LS, Alpert JS, et al. Circulation. 2014.
10. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Page RL, Joglar JA, Caldwell MA, et al. Journal of the American College of Cardiology. 2016.
11. What an anesthesiologist should know about pediatric arrhythmias. — Kuntz MT, Eagle SS, Dalal A, et al. Paediatric Anaesthesia. 2024.
12. European Heart Rhythm Association (EHRA)/Heart Rhythm Society (HRS)/Asia Pacific Heart Rhythm Society (APHRS)/Latin American Heart Rhythm Society (LAHRS) Expert Consensus Statement on the State of Genetic Testing for Cardiac Diseases. — Wilde AAM, Semsarian C, Márquez MF, et al. Heart Rhythm. 2022.
13. Wolff–Parkinson–White syndrome: De novo variants and evidence for mutational burden in genes associated with atrial fibrillation. — Coban-Akdemir ZH, Charng WL, Azamian M, et al. American Journal of Medical Genetics. Part A. 2020.
14. PRKAG2. — National Library of Medicine (MedlinePlus) 2007.
15. Wolff-Parkinson-White syndrome. — National Library of Medicine (MedlinePlus) 2022.
16. Abandoning Non Invasive Risk Stratification in WPW: There Is no Such Thing as a Free Lunch. — Krumerman A. Journal of Cardiovascular Electrophysiology. 2025.
17. Is Wolff‐Parkinson‐White Syndrome a Genetic Disease?. — Ehtisham J, Watkins H. Journal of Cardiovascular Electrophysiology. 2005.
18. Diagnosis and Management of Paroxysmal Supraventricular Tachycardia. — Peng G, Zei PC. The Journal of the American Medical Association. 2024.
19. Congenital Heart Disease in the Older Adult: A Scientific Statement From the American Heart Association. — Bhatt AB, Foster E, Kuehl K, et al. Circulation. 2015.
20. Risk Stratification for Arrhythmic Events in Patients With Asymptomatic Pre-Excitation: A Systematic Review for the 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Arshad A, Balk EM, et al. Journal of the American College of Cardiology. 2016.
21. 2015 ACC/AHA/HRS Guideline for the Management of Adult Patients With Supraventricular Tachycardia: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Page RL, Joglar JA, Caldwell MA, et al. Journal of the American College of Cardiology. 2016.
22. Sudden Death in the Young: Information for the Primary Care Provider. — Erickson CC, Salerno JC, Berger S, et al. Pediatrics. 2021.