Loading...
Zygomaticomaxillary Complex Fracture
The zygomaticomaxillary complex (ZMC) fracture — also called a "tripod" or "tetrapod" fracture — involves disruption of the zygoma at its four articulations: the zygomaticofrontal suture, zygomatic…
Dr. Lucas Mastropaolo
The zygomaticomaxillary complex (ZMC) fracture — also called a "tripod" or "tetrapod" fracture — involves disruption of the zygoma at its four articulations: the zygomaticofrontal suture, zygomaticomaxillary buttress, zygomaticotemporal suture, and zygomaticosphenoid suture. It is the second most common facial fracture after nasal fractures and accounts for approximately 40% of all facial fractures.[1-2] The following is a comprehensive clinical summary organized for emergency medicine and primary care workflows.
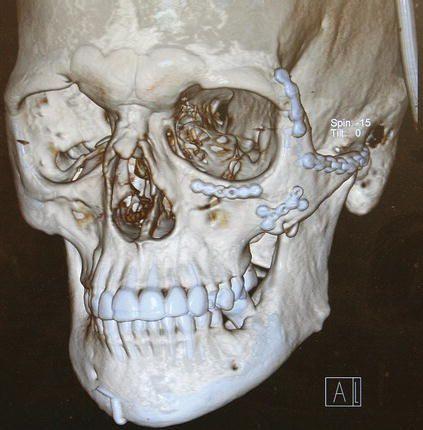
The following 3D CT reconstruction demonstrates a ZMC fracture with disruption of the zygomatic articulations and displacement of the malar eminence:
View full figure Figure 28. Postoperative 3D reconstruction demonstrating adequate reduction and plating of the zygomaticomaxillary complex and arch fractures. Isolated Zygoma and Zygomaticomaxillary Complex (ZMC) Fractures. Atlas of Operative Oral and Maxillofacial Surgery. December 31, 2021.
1. History
- Mechanism of injury: Direct blow to the cheek/malar eminence — assault (most common in many series), motor vehicle accidents, falls, and sports injuries[4-6]
- Characterize the force vector: lateral, anterior, or inferior impact
- Timing: When did the injury occur? Delay >2 weeks complicates reduction due to early bony union
Key symptoms to elicit
- Facial asymmetry or "flattening" of the cheek
- Numbness/tingling of the ipsilateral cheek, upper lip, upper teeth, or side of nose (infraorbital nerve [V2] distribution)
- Double vision (diplopia), especially on upward gaze
- Trismus or difficulty opening the mouth
- Unilateral epistaxis
- Pain with chewing
- Important negatives: Loss of vision, visual acuity changes, clear rhinorrhea (CSF leak), loss of consciousness, neck pain
2. Alarm Features
- Acute vision loss or decreasing visual acuity → retrobulbar hematoma or traumatic optic neuropathy (6% incidence); requires emergent lateral canthotomy/cantholysis[7]
- Afferent pupillary defect (APD) → optic nerve compromise
- Proptosis with tense orbit, pain with eye movement, and elevated IOP → retrobulbar hematoma
- Globe rupture (10% incidence of major/blinding injuries in ZMC fractures)[7]
- Extraocular muscle entrapment with restricted gaze and nausea/vomiting (especially in pediatric patients — "white-eyed blowout")
- Subcutaneous emphysema — suggests sinus communication; instruct patient not to blow nose
- CSF rhinorrhea — suggests associated skull base fracture
- Significant malocclusion — suggests concomitant Le Fort or mandible fracture
3. Medications
- Analgesics: NSAIDs (ibuprofen, ketorolac) and/or acetaminophen for mild-moderate pain; opioids for severe pain acutely
Antibiotics
- Non-operative management: No prophylactic antibiotics indicated[8]
- Operative (closed, non-contaminated): Single preoperative dose of a first-generation cephalosporin (e.g., cefazolin 2 g IV); no postoperative antibiotics needed beyond 24 hours[8-10]
- Open/contaminated fractures: Prophylactic antibiotics ≤24 hours; consider amoxicillin/clavulanate for oral flora coverage[9][11]
- Penicillin allergy: Clindamycin[11]
- Nasal decongestants: Oxymetazoline spray or pseudoephedrine to promote sinus drainage
- Antiemetics: Ondansetron if nausea/vomiting (especially with diplopia or muscle entrapment)
- Contraindicated: Avoid anticoagulants acutely if possible; avoid nasal packing on the affected side without surgical consultation
4. Diet
- Soft/liquid diet for 2–4 weeks if trismus or occlusal disturbance is present[12]
- Avoid hard, chewy foods that require forceful mastication
- Adequate hydration and caloric intake, especially if jaw opening is limited
- Long-term: Resume normal diet as trismus resolves (typically within days to weeks post-repair)
5. Review of Systems
- Eyes: Visual acuity changes, diplopia, eye pain, tearing, periorbital swelling
- ENT: Epistaxis, nasal obstruction, clear rhinorrhea, anosmia, hearing changes
- Neurologic: Facial numbness (V2 distribution), headache, altered mental status, neck pain
- MSK/Dental: Trismus, malocclusion, loose teeth, jaw pain
- Constitutional: Fever (late — suggests infection), weight loss (difficulty eating)
6. Collateral History and Family History
- Collateral: Witnesses to mechanism (assault vs. fall vs. MVC); alcohol or substance use at time of injury (>1/3 of ZMC fractures involve alcohol); loss of consciousness; anticoagulant use[6]
- Social context: Intimate partner violence screening — facial fractures are a sentinel injury
- Family history: Generally not contributory; however, connective tissue disorders (e.g., Ehlers-Danlos, osteogenesis imperfecta) may predispose to fractures with minimal force
7. Risk Factors
- Male sex (male-to-female ratio approximately 3–6:1)[4-6]
- Age 20–40 years (peak incidence)[4-5]
- Alcohol/substance use — present in up to 70% of assault-related cases[6][13]
- Interpersonal violence — leading cause in many Western populations[4][14]
- Motor vehicle accidents — leading cause in developing countries[15-16]
- Contact sports (boxing, martial arts, rugby, hockey)
- Falls — increasingly common in elderly populations[5]
- Osteoporosis — lower-energy mechanisms in elderly patients
8. Differential Diagnosis
- Isolated zygomatic arch fracture — trismus and cheek flattening without orbital involvement
- Orbital blowout fracture (floor/medial wall) — diplopia and enophthalmos without malar flattening
- Le Fort II fracture — pyramidal fracture with midface mobility, bilateral involvement
- Le Fort III fracture — craniofacial disjunction with CSF leak risk
- Naso-orbito-ethmoid (NOE) fracture — telecanthus, CSF leak, medial canthal tendon disruption
- Mandibular condyle/subcondylar fracture — trismus and malocclusion without malar findings
- Isolated maxillary sinus fracture — epistaxis without cheek deformity
- Soft tissue contusion without fracture — swelling and ecchymosis but no bony step-off, no paresthesia
9. Past Medical History
- Prior facial fractures or facial surgery
- Pre-existing ocular conditions (baseline diplopia, strabismus, prior orbital surgery)
- Bleeding disorders or anticoagulant/antiplatelet use
- Dental history (dentures, implants, prior malocclusion)
- History of osteoporosis or metabolic bone disease
- Immunosuppression (increases infection risk post-operatively)
10. Physical Exam
Inspection
- Periorbital ecchymosis ("raccoon eye") — present in ~77%[17]
- Malar flattening (cheek depression) — most common sign (73.6%); may be masked by edema acutely[18]
- Facial asymmetry — compare both sides from above (bird's-eye view)
- Lateral subconjunctival hemorrhage with no posterior limit (highly specific)[19]
- Subcutaneous emphysema
- Unilateral epistaxis
Palpation
- Palpable bony step-off at infraorbital rim, zygomaticofrontal suture, or zygomatic arch (highly specific)[19]
- Tenderness over malar eminence
- Crepitus (subcutaneous emphysema)
Neurologic
- Infraorbital nerve (V2) sensation: Test light touch over ipsilateral cheek, upper lip, upper gingiva, and lateral nose — paresthesia/anesthesia in 44–83%[17][20-21]
Ophthalmologic
- Visual acuity (Snellen chart — mandatory before any intervention)
- Pupillary exam (APD screening)
- Extraocular movements — restriction suggests muscle entrapment; forced duction test if concern
- Diplopia assessment (especially upward gaze)
- Enophthalmos (may be masked by edema acutely; becomes apparent as swelling resolves)
- Unequal pupil heights (vertical dystopia)[20]
- Intraocular pressure if retrobulbar hematoma suspected
Oral
- Trismus (limited mouth opening due to impingement of depressed arch on coronoid process)[20]
- Malocclusion
- Ecchymosis of the maxillary buccal sulcus
- Clinical decision rule: The presence of any one of (a) palpable bony step, (b) lateral subconjunctival hemorrhage with no posterior limit, (c) infraorbital nerve paresthesia, or (d) palpable emphysema has 100% sensitivity for displaced ZMC fracture[19]
11. Lab Studies
- Routine labs are generally not required for isolated ZMC fractures
- Pre-operative labs if surgical repair planned: CBC, BMP, coagulation studies, type and screen
- Blood alcohol level / urine drug screen — if altered mental status or medicolegal concerns
- Troponin — only if concomitant blunt chest trauma or cardiac symptoms
- No specific lab abnormalities are diagnostic of ZMC fracture
12. Imaging
- First-line: Maxillofacial CT with thin-cut (1–2 mm) axial and coronal reconstructions — gold standard for diagnosis, classification, and surgical planning[1][12][22]
- 3D reconstructions are helpful for surgical planning and assessing degree of displacement
- Evaluate: fracture lines at all four articulations, degree of displacement/rotation, orbital floor integrity, orbital volume, sinus opacification
- Plain radiographs (Waters view, submentovertex): Largely supplanted by CT; may show zygomatic arch depression or sinus opacification but miss significant pathology
- When imaging is unnecessary: If clinical exam shows no bony step-off, no subconjunctival hemorrhage, no paresthesia, and no emphysema, the clinical decision rule has 100% sensitivity for ruling out displaced fracture, potentially avoiding imaging[19]
Important CT findings
- Disruption of the zygomaticofrontal, zygomaticomaxillary, and zygomaticotemporal sutures
- Lateral orbital wall angulation → increased orbital volume → enophthalmos[22]
- Orbital floor fracture with herniation of orbital contents
- Hemosinus (maxillary sinus opacification)
- Posterior displacement ≥3 mm associated with 40% probability of needing orbital floor repair[2]
13. Special Tests
- Forced duction test: Performed under local anesthesia to differentiate mechanical entrapment from edema/paresis of extraocular muscles
- Hess chart / diplopia charting: Documents fields of diplopia for surgical planning and follow-up
- Hertel exophthalmometry: Quantifies enophthalmos (>2 mm difference is clinically significant)
Zingg classification (commonly used)
- Type A: Incomplete (isolated arch [A1], lateral wall [A2], or infraorbital rim [A3])
- Type B: Complete tetrapod fracture (all four articulations, monofragment)
- Type C: Comminuted multifragment fracture (worst prognosis)[23-24]
14. ECG
- Not routinely indicated for isolated ZMC fractures
Obtain ECG if
- Concomitant blunt chest trauma or high-energy mechanism (MVC)
- Elderly patient or known cardiac history
- Hemodynamic instability
- Pre-operative assessment for general anesthesia
- No specific ECG patterns are associated with facial fractures alone
15. Assessment
- ZMC fractures disrupt the structural integrity of the midface and orbit, affecting facial projection, orbital volume, mastication, and infraorbital nerve function
Severity stratification (Zingg classification)
- Type A (incomplete): Often managed conservatively or with closed reduction
- Type B (tetrapod): Most common; typically requires ORIF[6]
- Type C (comminuted): Highest complication rate (facial asymmetry, enophthalmos, persistent nerve injury); often requires multi-point fixation and orbital floor reconstruction[23-24]
- Typical presentation: Young male after assault or MVC with periorbital ecchymosis, cheek flattening, infraorbital numbness, and trismus
- Atypical presentations: Elderly patients after ground-level falls; bilateral ZMC fractures (rare, associated with high-energy mechanisms)
- Complications: Persistent infraorbital nerve paresthesia (most common, 37–45%), facial asymmetry (14%), enophthalmos (7%), persistent diplopia (7%), malunion, infection (4%)[17][24]
16. Treatment Plan
Initial Stabilization (ED)
- ABCs; assess for concomitant cervical spine, intracranial, and ocular injuries
- Control epistaxis with nasal packing if needed
- Ice and elevation of head of bed to 30°
- Analgesia (NSAIDs ± opioids)
- Instruct patient not to blow nose (risk of orbital emphysema and infection)
- Emergent lateral canthotomy/cantholysis if retrobulbar hematoma with vision threat
- Conservative Management (non-displaced or minimally displaced fractures):
- Soft diet, analgesics, nasal decongestants, sinus precautions
- Close follow-up in 1–2 weeks with repeat exam after swelling resolves[12]
Surgical Management (displaced fractures)
- Open reduction and internal fixation (ORIF) is the standard of care[25-26]
- Timing: Ideally within 7–14 days of injury; delay beyond 2–3 weeks increases difficulty due to early bony union
Fixation approaches
- Zygomaticofrontal suture (lateral brow incision or upper eyelid crease)
- Zygomaticomaxillary buttress (intraoral vestibular incision)
- Infraorbital rim (transconjunctival or subciliary approach)
- Fixation points: 3-point fixation is conventionally accepted and may be superior to 2-point for reducing malar asymmetry, though recent evidence suggests 2-point fixation may be adequate in selected cases[27-29]
- Orbital floor reconstruction: Indicated when orbital dystopia, significant posterior displacement (≥3 mm), or large orbital floor defect is present[2][12]
- Closed reduction (Gillies or Carroll-Girard approach): May be used for minimally displaced, non-comminuted fractures with stable reduction[12]
- Antibiotics: Single preoperative dose of cefazolin; no postoperative antibiotics beyond 24 hours for non-contaminated fractures[8-10]
17. Disposition
Discharge criteria (from ED)
- Isolated, non-displaced or minimally displaced ZMC fracture
- Normal visual acuity, no entrapment, no retrobulbar hematoma
- Adequate pain control
- Reliable follow-up arranged with oral and maxillofacial surgery (OMFS) or plastic surgery/facial trauma within 5–7 days
Admission criteria
- Concomitant intracranial injury, polytrauma, or hemodynamic instability
- Retrobulbar hematoma or acute vision-threatening injury
- Inability to protect airway (severe bilateral fractures, massive edema)
- Need for urgent surgical intervention
Observation indications
- Borderline visual acuity changes requiring serial exams
- Significant periorbital edema with inability to perform adequate eye exam
Specialist consultation triggers
- OMFS or plastic surgery: All displaced ZMC fractures
- Ophthalmology: All ZMC fractures warrant ophthalmologic evaluation, ideally preoperatively; urgent if vision changes, APD, globe injury, or entrapment[7]
- Neurosurgery: If associated skull base fracture or intracranial injury
18. Follow Up / Return Precautions
Follow-up timing
- OMFS/plastic surgery: Within 5–7 days for surgical planning (allows initial edema to subside)
- Ophthalmology: Within 1–2 weeks, or sooner if visual symptoms
- Post-operative: 1 week, 1 month, 3 months, 6 months to assess nerve recovery, symmetry, and ocular function
Return precautions — seek immediate care for
- Worsening or new vision changes (blurring, double vision, vision loss)
- Increasing eye pain, proptosis, or inability to open the eye
- Increasing facial swelling, redness, warmth, or fever (infection)
- New or worsening difficulty opening the mouth
- Clear fluid draining from the nose (CSF leak)
Patient counseling
- Do not blow nose for at least 2–4 weeks
- Sneeze with mouth open
- Avoid contact sports for 6–8 weeks minimum
- Avoid strenuous activity and heavy lifting for 2–4 weeks
- Sleep with head elevated
- Infraorbital nerve numbness may persist for months and is the most common long-term sequela (persists in ~37–45% at 6 months)[17][24]
Expected recovery
- Periorbital edema and ecchymosis: Resolves over 2–4 weeks
- Diplopia: Resolves in most cases within 3 months post-repair (drops from 16% to 2%)[7]
- Trismus: Typically resolves within weeks of reduction[17]
- Infraorbital nerve recovery: Variable; may take 6–12 months; some patients have permanent deficit[17][24]
References
1. ACR Appropriateness Criteria® Imaging of Facial Trauma Following Primary Survey. — Expert Panel on Neurological Imaging, Parsons MS, Policeni B, et al. Journal of the American College of Radiology : JACR. 2022.
2. Refining Indications for Orbital Floor Reconstruction in Zygomaticomaxillary Complex Fractures. — Soliman L, Menville JE, Rhee BS, et al. The Journal of Craniofacial Surgery. 2025.
3. Isolated Zygoma and Zygomaticomaxillary Complex (ZMC) Fractures. — Christopher J. Haggerty Atlas of Operative Oral and Maxillofacial Surgery. 2022.
4. The "European Zygomatic Fracture" Research Project: The Epidemiological Results From a Multicenter European Collaboration. — Brucoli M, Boffano P, Broccardo E, et al. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2019.
5. Retrospective Analysis of 471 Surgically Treated Zygomaticomaxillary Complex Fractures. — Blumer M, Kumalic S, Gander T, et al. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2018.
6. Characteristics and Epidemiology of Zygomaticomaxillary Complex Fractures. — Bogusiak K, Arkuszewski P. The Journal of Craniofacial Surgery. 2010.
7. Ophthalmic Injuries in Patients With Zygomaticomaxillary Complex Fractures Requiring Surgical Repair. — Jamal BT, Pfahler SM, Lane KA, et al. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2009.
8. Antibiotic Prophylaxis in Injury: An American Association for the Surgery of Trauma Critical Care Committee Clinical Consensus Document. — Appelbaum RD, Farrell MS, Gelbard RB, et al. Trauma Surgery & Acute Care Open. 2023.
9. Antibiotic Prophylaxis in Trauma: Global Alliance for Infection in Surgery, Surgical Infection Society Europe, World Surgical Infection Society, American Association for the Surgery of Trauma, and World Society of Emergency Surgery Guidelines. — Coccolini F, Sartelli M, Sawyer R, et al. The Journal of Trauma and Acute Care Surgery. 2024.
10. The Role of Postoperative Prophylactic Antibiotics in the Treatment of Facial Fractures: A Randomised, Double-Blind, Placebo-Controlled Pilot Clinical Study. Part 3: Le Fort and Zygomatic Fractures in 94 Patients. — Soong PL, Schaller B, Zix J, et al. The British Journal of Oral & Maxillofacial Surgery. 2014.
11. Antibiotic prophylaxis for traumatic facial fractures. — Erstad BL, Kopp BJ, Tang AL. Journal of Clinical Pharmacy and Therapeutics. 2022.
12. Investigation of infraorbital nerve injury following zygomaticomaxillary complex fractures. — Sakavicius D, Juodzbalys G, Kubilius R, Sabalys GP. Journal of Oral Rehabilitation. 2008.
13. Etiology and Injury Patterns of Maxillofacial Fractures From the Years 2010 to 2013 in Mecklenburg-Western Pomerania, Germany: A Retrospective Study of 409 Patients. — Schneider D, Kämmerer PW, Schön G, et al. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2015.
14. Epidemiological Analysis of Zygomatic Bone Fractures in North-Western Romanian Population: A 10-Year Retrospective Study. — Ţent PA, Juncar RI, Juncar M. In Vivo. 2020.
15. Changing Patterns of Zygomaticomaxillary Complex Fractures: A Retrospective Study. — Umakant Chodankar N, Dhupar V, Akkara F, Satish Kumar P. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2023.
16. Facial Fractures: Large Epidemiologic Survey in Northern Brazil Reveals Some Unique Characteristics. — Ribeiro Ribeiro AL, da Silva Gillet LC, de Vasconcelos HG, et al. Journal of Oral and Maxillofacial Surgery : Official Journal of the American Association of Oral and Maxillofacial Surgeons. 2016.
17. Correlation Between Clinical Findings and CT-measured Displacement in Patients With Fractures of the Zygomaticomaxillary Complex. — Mueller CK, Zeiß F, Mtsariashvili M, Thorwarth M, Schultze-Mosgau S. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2012.
18. Direct or Indirect Surgical Approach of Zygomatic Complex Fracture: A Comparative Study. — Alshalah ME, Enezei HH, Aldaghir OM, et al. The Journal of Craniofacial Surgery. 2023.
19. A Clinical Decision Rule to Predict Zygomatico-Maxillary Fractures. — Haworth S, Bates A, Beech A, Knepil G. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2017.
20. Anatomic, Clinical, Surgical, and Radiographic Correlation of the Zygomatic Complex Fracture. — Gerlock AJ, Sinn DP. AJR. American Journal of Roentgenology. 1977.
21. Infraorbital Nerve Posttraumatic Deficit and Displaced Zygomatic Fractures: A Double-Center Study. — Boffano P, Roccia F, Gallesio C, Karagozoglu KH, Forouzanfar T. The Journal of Craniofacial Surgery. 2013.
22. Spectrum of Critical Imaging Findings in Complex Facial Skeletal Trauma. — Winegar BA, Murillo H, Tantiwongkosi B. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2013.
23. Treatment Complications Analysis of Zygomatic Complex Fractures: A Retrospective Study. — Tong Y, Jie B, Zhang Y, He Y. The Journal of Craniofacial Surgery. 2026.
24. Surgical Treatment of Unilateral Zygomaticomaxillary Complex Fractures: A 7-Year Observational Study Assessing Treatment Outcome in 153 Cases. — van Hout WM, Van Cann EM, Koole R, Rosenberg AJ. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2016.
25. Evidence-Based Medicine: Evaluation and Treatment of Zygoma Fractures. — Birgfeld CB, Mundinger GS, Gruss JS. Plastic and Reconstructive Surgery. 2017.
26. Surgical Approaches and Postoperative Outcomes in Zygomatic Fractures: A Systematic Review. — Anyikwa CL, Okoroafor FC, Onyebuchi EP, et al. The British Journal of Oral & Maxillofacial Surgery. 2025.
27. Comparative Evaluation of 2-Point vs 3-Point Fixation in the Treatment of Zygomaticomaxillary Complex Fractures - A Systematic Review. — Gadkari N, Bawane S, Chopra R, Bhate K, Kulkarni D. Journal of Cranio-Maxillo-Facial Surgery : Official Publication of the European Association for Cranio-Maxillo-Facial Surgery. 2019.
28. Modeling Stability Post Zygomatic Fracture Reconstruction. — Arjmand H, Fialkov JA, Whyne CM. Journal of Plastic, Reconstructive & Aesthetic Surgery : JPRAS. 2024.
29. Advances in Facial Fracture Care in Patients With Zygomaticomaxillary Complex Fractures. — Swift WM, Marston AP, Tollefson TT. Current Opinion in Otolaryngology & Head and Neck Surgery. 2025.