Anthrax (Gastrointestinal)
Gastrointestinal anthrax is a rare but potentially fatal form of anthrax infection caused by Bacillus anthracis following ingestion of contaminated meat from infected animals. The disease has a mor…
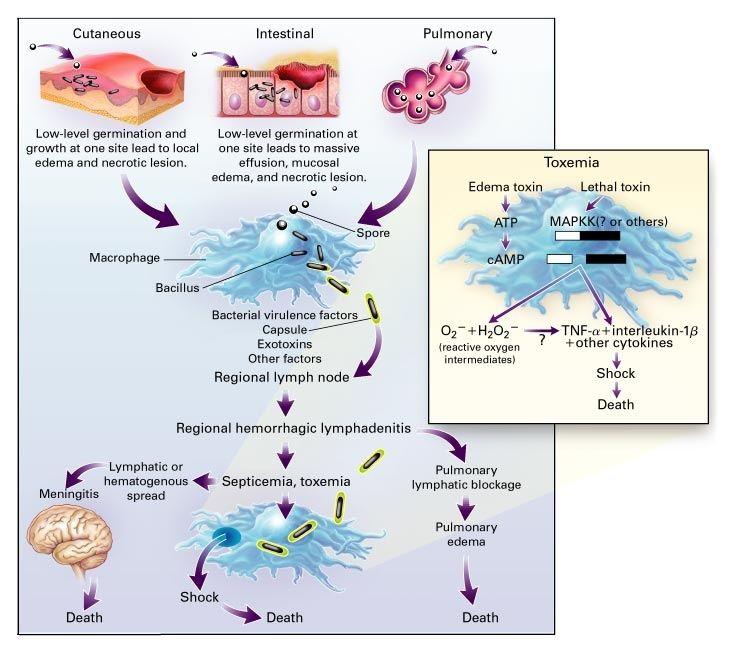
Gastrointestinal anthrax is a rare but potentially fatal form of anthrax infection caused by Bacillus anthracis following ingestion of contaminated meat from infected animals. The disease has a mortality rate of 25-60% if untreated and requires aggressive systemic antibiotic therapy similar to inhalational anthrax. [1-3]
The following figure illustrates the pathophysiology of anthrax infection, showing how spores germinate within macrophages and progress to systemic toxemia:
1. History
Key HPI questions
• Recent consumption of undercooked or raw meat, particularly from herbivores (sheep, goats, cattle)
• Travel to endemic areas (sub-Saharan Africa, central/southwestern Asia, southern/eastern Europe)
• Onset and progression of symptoms over 1-7 days
• Characterization of abdominal pain (location, severity, progression)
• Associated nausea, vomiting, diarrhea (bloody vs non-bloody)
• Fever pattern and constitutional symptoms
Symptom characterization
• Initial phase: nausea, vomiting, malaise, anorexia, fever
• Progressive phase: severe abdominal pain, bloody diarrhea, abdominal distention
• Oropharyngeal variant: sore throat, dysphagia, neck swelling
Timing and progression
• Incubation period: 1-7 days (median 3 days) after ingestion [1][3-4]
• Rapid progression from initial symptoms to systemic illness within days
• Two-phase progression: initial GI symptoms followed by acute abdomen presentation
Important negatives
• No recent antibiotic use that might alter presentation
• No known exposure to anthrax spores or bioterrorism events
• No concurrent respiratory symptoms (to distinguish from inhalational anthrax)
2. Alarm Features
Red flag symptoms/signs
• Bloody diarrhea with severe abdominal pain
• Signs of acute abdomen with rebound tenderness
• Hematemesis or coffee-ground emesis
• Rapid development of ascites
• Signs of sepsis or shock
• Massive cervical lymphadenopathy (oropharyngeal variant)
• Respiratory distress from pharyngeal edema
Features suggesting life-threatening pathology
• Hemodynamic instability
• Signs of intestinal perforation
• Altered mental status suggesting meningitis
• Mediastinal widening on chest imaging (can occur with GI anthrax) [4]
Indications for urgent escalation
• Any suspicion of anthrax requires immediate infectious disease consultation and CDC notification
• ICU-level care for systemic symptoms
• Surgical consultation for acute abdomen presentation
3. Medications
Relevant medication contributors
• Recent antibiotic use may alter bacterial culture results
• Immunosuppressive medications increase risk of severe disease
• Proton pump inhibitors may theoretically increase susceptibility
Primary treatments
• IV ciprofloxacin 400 mg q12h (preferred for systemic disease) [1][5]
• IV doxycycline 100 mg q12h (alternative if ciprofloxacin contraindicated)
• Combination therapy required for systemic disease: bactericidal agent + protein synthesis inhibitor + CNS-penetrating agent [6]
Contraindicated medications
• Penicillin or ampicillin as monotherapy (β-lactamase concerns) [7]
• Avoid doxycycline in pregnancy and young children when alternatives available
Key medication considerations
• Clindamycin strongly recommended as adjunctive therapy to reduce toxin production [5]
• Duration: 60 days for bioterrorism exposure, 2-3 weeks for naturally acquired disease [1]
• Switch to oral therapy once clinically stable
4. Diet
Acute management
• NPO initially if severe nausea/vomiting or signs of acute abdomen
• Clear liquids once stable, advance as tolerated
• Monitor for GI bleeding
Dietary triggers
• Undercooked meat from herbivores (primary risk factor)
• Stored meat products from endemic areas
• Traditional meat preparations in high-risk regions
Hydration considerations
• Aggressive IV fluid resuscitation for shock
• Monitor for fluid and electrolyte imbalances from GI losses
• Blood product support if significant GI bleeding
5. Review of Systems
Important ROS questions
• Respiratory: dyspnea, chest pain (rule out inhalational anthrax)
• Neurologic: headache, altered mental status, neck stiffness (meningitis)
• Genitourinary: oliguria (shock/dehydration)
• Skin: any cutaneous lesions (concurrent cutaneous anthrax)
• Constitutional: fever pattern, weight loss, night sweats
High-yield associated systems
• Cardiovascular: signs of shock, fluid overload
• Pulmonary: pleural effusions can occur with GI anthrax
• Hematologic: bleeding tendency, coagulopathy
6. Collateral History and Family History
Important collateral information
• Household members with similar symptoms (common source exposure)
• Travel companions or dining partners
• Source and preparation of suspected meat
• Occupational exposure to animal products
Relevant hereditary conditions
• Immunodeficiency syndromes
• No specific genetic predisposition to anthrax
Social context
• Immigration from endemic areas
• Traditional food practices
• Veterinary or agricultural occupation
7. Risk Factors
Major epidemiologic risk factors
• Consumption of undercooked meat from herbivores
• Travel to or residence in endemic areas
• Agricultural or veterinary occupation
• Bioterrorism exposure (intentional release)
Clinical risk factors
• Immunocompromised state
• Advanced age
• Delayed recognition and treatment
Geographic considerations
• Sub-Saharan Africa, central/southwestern Asia
• Southern and eastern Europe
• Southwestern United States (sporadic wildlife cases)
8. Differential Diagnosis
Most important alternative diagnoses
• Acute gastroenteritis (viral, bacterial, parasitic)
• Inflammatory bowel disease exacerbation
• Ischemic bowel disease
• Appendicitis or other surgical abdomen
• Peptic ulcer disease with bleeding
Dangerous cannot-miss diagnoses
• Intestinal perforation
• Mesenteric ischemia
• Sepsis from other bacterial causes
• Toxic megacolon
• Anthrax meningitis (up to 77% of systemic cases) [5]
Mimics and distinguishing features
• Massive ascites development distinguishes from typical gastroenteritis [4][8-9]
• Hemorrhagic mesenteric lymphadenitis on imaging
• Large gram-positive bacilli in blood cultures or ascites fluid
• Epidemiologic clues (meat consumption, travel history)
9. Past Medical History
Relevant prior conditions
• Previous episodes of anthrax (rare but possible)
• Immunocompromising conditions
• Chronic GI diseases
• Previous abdominal surgeries
Surgical history
• Prior bowel resections
• Previous exploratory laparotomy
• Appendectomy (to distinguish from appendicitis)
Chronic illnesses impacting management
• Diabetes mellitus
• Chronic kidney disease (affects antibiotic dosing)
• Heart failure (fluid management considerations)
10. Physical Exam
Key exam findings
• Vital signs: fever, tachycardia, hypotension (shock)
• Abdominal exam: diffuse tenderness, rebound tenderness, distention
• Ascites: shifting dullness, fluid wave
• Lymphadenopathy: mesenteric (not palpable), cervical (oropharyngeal variant)
Oropharyngeal variant findings
• Oral or esophageal ulcers with pseudomembrane
• Massive cervical lymphadenopathy and neck edema
• Dysphagia and potential airway compromise
Expected vs concerning findings
• Expected: fever, abdominal tenderness, ascites
• Concerning: signs of perforation, hemodynamic instability, altered mental status
Focused exam maneuvers
• Careful abdominal examination for peritoneal signs
• Assessment for ascites
• Neurologic examination for meningeal signs
11. Lab Studies
Recommended labs
• Blood cultures (high yield - B. anthracis grows rapidly) [1-2]
• Complete blood count with differential
• Comprehensive metabolic panel
• Liver function tests
• Coagulation studies (PT/PTT/INR)
• Lactate (sepsis marker)
Expected abnormalities
• Hemoconcentration from fluid losses
• Elevated transaminases
• Anemia from GI bleeding
• Thrombocytopenia and coagulopathy in severe cases [1]
Ascites fluid analysis
• Cell count and differential
• Gram stain and culture (may show large gram-positive bacilli) [4]
• Protein, glucose, LDH
• Appearance ranges from clear to purulent
12. Imaging
First-line imaging
• CT abdomen/pelvis with contrast: bowel wall thickening, ascites, mesenteric lymphadenopathy [1]
• Chest X-ray: may show mediastinal widening (reported in GI anthrax) [4]
Key imaging findings
• Inflammatory changes in bowel wall
• Massive ascites
• Hemorrhagic mesenteric lymphadenitis
• Terminal ileum and cecum involvement most common [8-9]
When imaging is unnecessary
• Stable patients with clear clinical picture
• When immediate surgical intervention is needed
13. Special Tests
Diagnostic confirmation
• PCR testing at reference laboratories (state health departments)
• Immunohistochemistry on tissue specimens
• Serology (late in disease course, limited utility) [1]
Point-of-care tests
• Gram stain of blood, ascites, or tissue (large gram-positive bacilli)
• Rapid antigen tests (if available)
Laboratory Response Network (LRN)
• State and local health departments have access for rapid identification [3]
• Immediate notification required for suspected cases
14. ECG
ECG considerations
• Generally not specific for anthrax
• May show signs of shock (tachycardia, ischemic changes)
• Monitor for arrhythmias in severe sepsis
Indications for ECG
• Hemodynamic instability
• Chest pain or respiratory symptoms
• Elderly patients or those with cardiac risk factors
15. Assessment
Clinical summary
• Gastrointestinal anthrax is a rare, toxin-mediated disease with high mortality
• Rapid progression from initial GI symptoms to systemic illness
• Two main presentations: oropharyngeal and lower GI tract involvement
Severity stratification
• Mild: localized GI symptoms without systemic signs
• Moderate: systemic symptoms with hemodynamic stability
• Severe: shock, ascites, signs of perforation, or meningitis
Typical vs atypical presentations
• Typical: recent meat consumption, rapid progression, massive ascites
• Atypical: isolated oropharyngeal involvement, concurrent respiratory symptoms
Complications to consider
• Intestinal perforation
• Anthrax meningitis (up to 77% of systemic cases)
• Septic shock and multi-organ failure
• Coagulopathy and bleeding
16. Treatment Plan
Initial stabilization
• Aggressive fluid resuscitation for shock
• Vasopressor support if needed
• Blood product transfusion for significant bleeding
• Airway management for oropharyngeal edema
Antimicrobial therapy (systemic disease)
• Primary regimen: IV ciprofloxacin 400 mg q12h + clindamycin 600-900 mg q8h + meropenem 1-2g q8h [5-6]
• Alternative: IV doxycycline 100 mg q12h (if ciprofloxacin contraindicated)
• Duration: 2-3 weeks for naturally acquired, 60 days if bioterrorism suspected
Adjunctive therapies
• Antitoxin therapy (if available through CDC) [6]
• Corticosteroids for severe edema or suspected meningitis [1][4]
• Supportive care per sepsis protocols
17. Disposition
Admission criteria
• All suspected cases of gastrointestinal anthrax
• Systemic symptoms or hemodynamic instability
• Need for IV antibiotics and monitoring
ICU criteria
• Hemodynamic instability requiring vasopressors
• Respiratory compromise
• Signs of meningitis or altered mental status
• Multi-organ dysfunction
Discharge criteria
• Clinical improvement on oral antibiotics
• Hemodynamic stability
• Ability to tolerate oral intake
• Completion of IV antibiotic course
Specialist consultation
• Infectious disease: mandatory for all cases
• Surgery: if signs of perforation or acute abdomen
• Critical care: for severe systemic disease
18. Follow Up / Return Precautions
Follow-up timing
• 24-48 hours after discharge for clinical reassessment
• Weekly during antibiotic course
• Infectious disease follow-up within 1 week
Return precautions
• Worsening abdominal pain or distention
• Recurrent fever or signs of infection
• Neurologic symptoms (headache, confusion, neck stiffness)
• Respiratory distress
• Signs of bleeding or shock
Patient counseling
• Complete full antibiotic course (60 days if bioterrorism exposure)
• Avoid undercooked meat, especially from herbivores
• Report any household contacts with similar symptoms
• Understand that this is a reportable disease
Expected recovery
• Symptoms typically resolve in 10-14 days with appropriate treatment [4]
• Mortality significantly reduced with early, aggressive treatment
• Long-term sequelae rare with appropriate therapy
References
1. Clinical Management of Potential Bioterrorism-Related Conditions. — Adalja AA, Toner E, Inglesby TV. The New England Journal of Medicine. 2015.
2. Anthrax Infection. — Sweeney DA, Hicks CW, Cui X, Li Y, Eichacker PQ. American Journal of Respiratory and Critical Care Medicine. 2011.
3. CDC Issues Guidelines on Illnesses Associated With Intentional Release of Biologic Agents. — Ressel G. American Family Physician. 2001.
4. Anthrax. — Dixon TC, Meselson M, Guillemin J, Hanna PC. The New England Journal of Medicine. 1999.
5. Conference Report on Public Health and Clinical Guidelines for Anthrax. — Stern EJ, Uhde KB, Shadomy SV, Messonnier N. Emerging Infectious Diseases. 2008.
6. CDC Guidelines for the Prevention and Treatment of Anthrax, 2023. — William A. Bower MD, Yon Yu PharmD, Marissa K. Person MSPH, et al United States Centers for Disease Control and Prevention. 2025.
7. ACCF/AHA/CDC Conference Report on Emerging Infectious Diseases and Biological Terrorism Threats. Task Force III: Prevention and Control of Cardiovascular Complications of Emerging Infectious Diseases and Potential Biological Terrorism Agents and Diseases. — Cooper LT, Mensah GA, Baddour LM, et al. Journal of the American College of Cardiology. 2007.
8. Anthrax as a Biological Weapon, 2002: Updated Recommendations for Management. — Inglesby TV, O'Toole T, Henderson DA, et al. The Journal of the American Medical Association. 2002.
9. Anthrax as a Biological Weapon: Medical and Public Health Management. — Inglesby TV, Henderson DA, Bartlett JG, et al. The Journal of the American Medical Association. 1999.