Appendicitis
Acute appendicitis is inflammation of the vermiform appendix and is the most common reason for emergency abdominal surgery worldwide, with an annual incidence of approximately 96.5 to 100 cases per…
Acute appendicitis is inflammation of the vermiform appendix and is the most common reason for emergency abdominal surgery worldwide, with an annual incidence of approximately 96.5 to 100 cases per 100,000 adults and a lifetime risk of 7-8%. [1-3]
Clinical Presentation and Diagnosis
The diagnosis is based on history, physical examination, laboratory evaluation, and imaging, achieving accurate diagnosis in more than 90% of patients. [1] Key clinical findings include:
- Right lower quadrant pain, abdominal rigidity, and periumbilical pain radiating to the right lower quadrant are the best signs for ruling in appendicitis in adults [2]
- In children, absent or decreased bowel sounds, positive psoas sign, positive obturator sign, and positive Rovsing sign are most reliable [2]
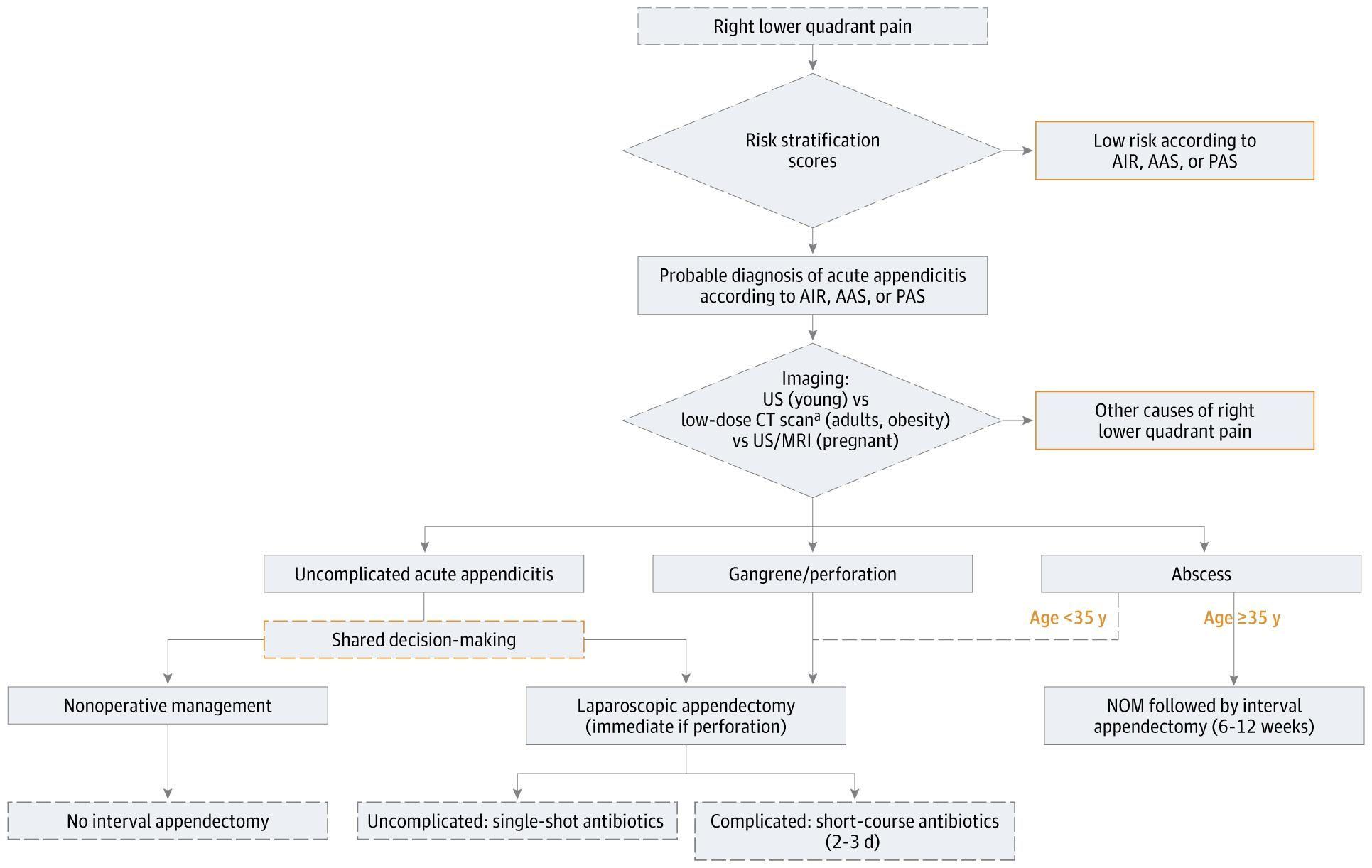
- Clinical risk scores (Alvarado, Pediatric Appendicitis Score, Appendicitis Inflammatory Response score) can stratify patients as low, moderate, or high risk [2][4]
Imaging: CT is more reliable than ultrasound for diagnosis in adults, with intravenous contrast generally recommended. [5] Ultrasound is preferred in pregnant women and children to minimize radiation exposure; if equivocal, MRI is the next choice. [5]
Management
The 2025 World Society of Emergency Surgery Jerusalem Guidelines provide a comprehensive management algorithm:
Surgical Management
Laparoscopic appendectomy is the gold standard and procedure of choice for acute appendicitis. [1][5] Compared to open appendectomy, laparoscopy offers shorter hospitalization (2.6 vs 3.4 days), earlier return to activity (14 vs 21 days), shorter duration of parenteral analgesia, and lower surgical site infection rates (48-70% decrease). [1]
- Preoperative antibiotics (single dose of cefoxitin, cefotetan, or cefazolin plus metronidazole) should be administered as soon as diagnosis is made [1][5]
- Postoperative antibiotics are not necessary for uncomplicated appendicitis [1][5]
- Appendectomy can be safely delayed within 24 hours without increased risk of adverse outcomes [4][6]
Nonoperative Management
Approximately 60% of adult patients with acute uncomplicated appendicitis can be treated successfully with antibiotics alone. [1] This approach is now acknowledged as a safe option and is included in guidelines from the American Association for the Surgery of Trauma, World Society of Emergency Surgery, and Eastern Association for the Surgery of Trauma. [1][4]
Key considerations for antibiotic therapy:
- Appropriate for selected patients with uncomplicated appendicitis who wish to avoid surgery and accept risk of recurrence [5-6]
- Typical regimens include ertapenem (parenteral) followed by oral antibiotics such as cefdinir and metronidazole for 7-10 days [3]
- Patients with appendicolith (present in ~25% of cases) are less likely to respond to antibiotics, with higher appendectomy rates (41% vs 25%) and complication rates (20.2% vs 3.5%) [1][3]
- Improvement should be expected within 48 hours; worsening symptoms, diffuse peritonitis, or sepsis indicate need for appendectomy [3]
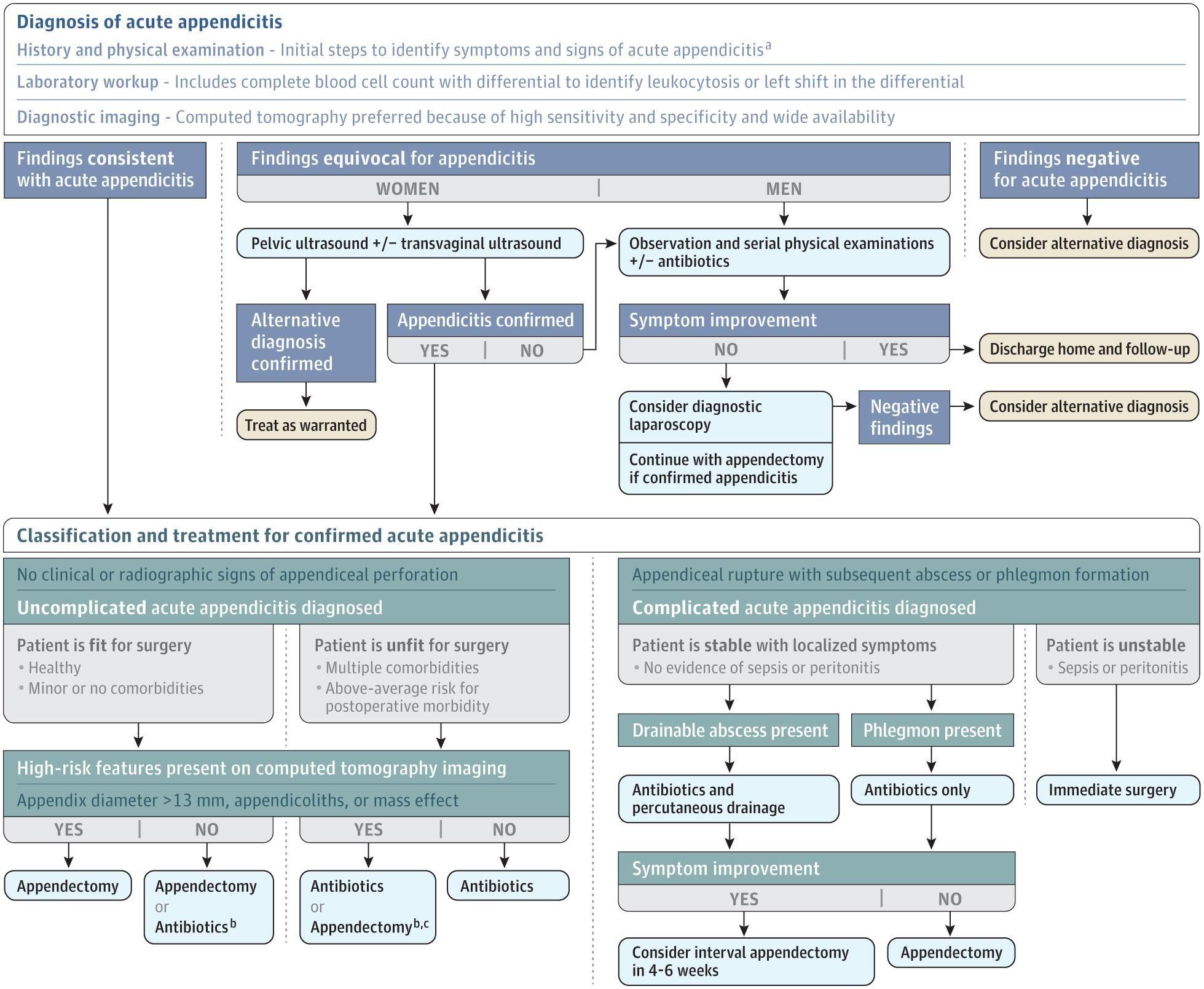
The following algorithm from JAMA illustrates the diagnostic and management approach:
Complicated Appendicitis
For patients with appendiceal abscess, stable patients may benefit from percutaneous drainage plus antibiotics rather than immediate surgery. [1] Postoperative antibiotics should be limited to short courses (2-3 days) in complicated disease. [4] Follow-up strategies are essential after nonoperative management of complicated appendicitis to detect potential neoplasms, particularly in patients ≥35 years. [4]
Pain Management
Pain control with scheduled NSAIDs, acetaminophen, and opioids as needed should be a priority and does not result in delayed or unnecessary intervention. [2-3]
References
1. Diagnosis and Management of Acute Appendicitis in Adults: A Review. — Moris D, Paulson EK, Pappas TN. The Journal of the American Medical Association. 2021.
2. Acute Appendicitis: Efficient Diagnosis and Management. — Snyder MJ, Guthrie M, Cagle S. American Family Physician. 2018.
3. Treatment of Acute Uncomplicated Appendicitis. — Talan DA, Di Saverio S. The New England Journal of Medicine. 2021.
4. Diagnosis and Treatment of Acute Appendicitis. — Podda M, Ceresoli M, De Simone B, et al. JAMA Surgery. 2026.
5. American Association for the Surgery of Trauma Emergency General Surgery Guideline Summaries 2018: Acute Appendicitis, Acute Cholecystitis, Acute Diverticulitis, Acute Pancreatitis, and Small Bowel Obstruction. — Schuster KM, Holena DN, Salim A, Savage S, Crandall M. Trauma Surgery & Acute Care Open. 2018.
6. Gastrointestinal Surgical Emergencies Textbook. — Ashley E. Aaron, Andrea Amabile, Ciro Andolfi, et al American College of Surgeons (2021). 2021.