Bullous Pemphigoid
Bullous pemphigoid (BP) is the most common autoimmune subepidermal blistering disease, characterized by tense bullae on erythematous or normal skin with severe pruritus, predominantly affecting adu…
Bullous pemphigoid (BP) is the most common autoimmune subepidermal blistering disease, characterized by tense bullae on erythematous or normal skin with severe pruritus, predominantly affecting adults over age 70. [1-2] It is caused by IgG autoantibodies targeting hemidesmosomal proteins BP180 and BP230 at the dermal-epidermal junction. [1][3]
1. History
- Pruritus is often the earliest and most prominent symptom — may precede blisters by weeks to months [2][4]
- Characterize blister onset: tense (not flaccid), location, number of new blisters per day, and whether they arise on erythematous or normal-appearing skin [1][3]
- Ask about a prodromal phase: urticarial plaques, eczematous patches, or excoriations without frank blistering (nonbullous BP occurs in >20% of patients) [4]
- Timing relative to new medications — especially DPP-4 inhibitors (gliptins), immune checkpoint inhibitors, loop diuretics [5-7]
- Progression: chronic relapsing-remitting course; spontaneous remission possible but unpredictable [2][8]
- Important negatives: oral/mucosal involvement (present in <30% of BP, unlike pemphigus vulgaris), absence of scarring or milia (distinguishes from epidermolysis bullosa acquisita) [9-10]
2. Alarm Features
- Extensive disease (>10 new blisters/day) — associated with higher morbidity and mortality [11-12]
- Secondary infection of erosions: cellulitis, sepsis (leading cause of death) [13-14]
- Signs of systemic corticosteroid toxicity in elderly patients on treatment (hyperglycemia, delirium, GI bleeding) [11]
- Rapid spread with hemodynamic instability or fever suggesting superinfection
- Mucosal predominance → consider mucous membrane pemphigoid (risk of scarring, blindness) [15-16]
- New neurological symptoms — BP is strongly associated with dementia, Parkinson disease, and stroke [13][17]
3. Medications
Drug-associated BP triggers (review and consider discontinuation):
- DPP-4 inhibitors (gliptins): strongest evidence — vildagliptin, linagliptin, sitagliptin (OR ~2–4) [5-6][18]
- PD-1/PD-L1 checkpoint inhibitors (nivolumab, pembrolizumab) [7][19]
- Loop diuretics (furosemide), aldosterone antagonists (spironolactone) [6-7]
- Anticholinergics, dopaminergic agents, neuroleptics/antipsychotics [6][20]
- Penicillins and derivatives [7]
First-line treatments
- Topical clobetasol propionate 0.05% (10–40 g/day, tapered) — effective and safer than systemic steroids, especially in localized/moderate disease [11][13]
- Oral prednisolone 0.5 mg/kg/day — adequate for most patients; doses >0.75 mg/kg/day offer no additional benefit and increase mortality [11-12]
- Doxycycline 200 mg/day — acceptable blister control with significantly fewer serious adverse events than prednisolone; preferred in frail elderly [21]
Steroid-sparing adjuncts: azathioprine, mycophenolate mofetil, methotrexate, dapsone (evidence limited) [11][13]
Biologics for refractory disease: rituximab, omalizumab, dupilumab (FDA-approved for BP in adults) [22-23]
Contraindicated/caution: Avoid high-dose systemic corticosteroids in elderly with multiple comorbidities when possible — associated with increased mortality [11][13]
4. Diet
- No specific dietary triggers are established for BP
- Adequate protein and caloric intake is important for wound healing in elderly patients with extensive erosions
- Monitor for corticosteroid-induced hyperglycemia — dietary counseling for diabetic patients
- Ensure adequate calcium and vitamin D supplementation if on prolonged systemic corticosteroids
5. Review of Systems
- Skin: pruritus severity, new blister count, erosions, signs of infection (warmth, purulence, odor)
- Neurological: cognitive decline, tremor, gait disturbance, seizures (strong BP-neurological disease association) [13][17]
- Ophthalmologic: eye pain, redness, visual changes (rule out ocular mucous membrane pemphigoid)
- Oral: mouth sores, dysphagia (mucosal involvement)
- Systemic: fever, weight loss, fatigue (infection, malignancy screening)
- Endocrine: polyuria, polydipsia (steroid-induced diabetes)
6. Collateral History and Family History
- Collateral from caregivers is critical — many BP patients have dementia or cognitive impairment and cannot reliably report symptom timeline or medication changes [24-25]
- Medication reconciliation with pharmacy records (especially recent DPP-4 inhibitor or checkpoint inhibitor initiation) [5][7]
- Family history of autoimmune diseases (BP itself is not strongly hereditary, but autoimmune predisposition may be relevant)
- HLA-DQA105 has been associated with DPP-4 inhibitor-induced BP [26]
- Social context: functional status, ability to apply topical medications, caregiver availability (critical for treatment planning) [11][21]
7. Risk Factors
- Age >70 years — strongest demographic risk factor [1][21]
- Neurological diseases: dementia (OR ~4–5), Parkinson disease (OR ~3), stroke (OR ~2.7), epilepsy, multiple sclerosis [13][17]
- Medication exposure: DPP-4 inhibitors, checkpoint inhibitors, loop diuretics, spironolactone, neuroleptics [6-7]
- Immobility and institutionalization [21]
- Diabetes mellitus (partly confounded by DPP-4 inhibitor use) [5][20]
- Psoriasis (independent association reported) [13]
- Low Karnofsky performance score — predicts worse outcomes [12-13]
8. Differential Diagnosis
- Pemphigus vulgaris: flaccid blisters, positive Nikolsky sign, mucosal predominance, intraepidermal acantholysis [9][15]
- Linear IgA bullous dermatosis: "string of pearls" pattern, IgA deposits on DIF; drug-induced (vancomycin) [15][27]
- Epidermolysis bullosa acquisita: acral/mechanical blisters, scarring, milia; dermal-side binding on salt-split skin [11][16]
- Dermatitis herpetiformis: grouped vesicles on extensor surfaces, granular IgA in dermal papillae, celiac association [27]
- Mucous membrane pemphigoid: mucosal predominance with scarring (ocular, oral, genital) [15-16]
- Contact dermatitis / eczema / urticaria: common misdiagnoses in the nonbullous prodromal phase [4]
- Scabies with secondary bullae: especially in institutionalized elderly [14]
- Drug eruption / Stevens-Johnson syndrome / TEN: acute onset, mucosal involvement, systemic toxicity
- Bullous diabeticorum: spontaneous blisters on extremities in diabetics, no autoantibodies
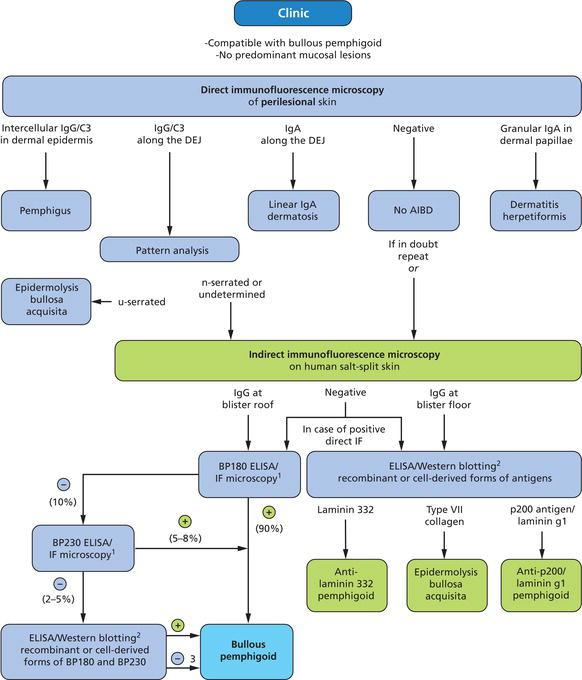
The following diagnostic algorithm from Rook's Dermatology Handbook illustrates the immunofluorescence-based approach to differentiating subepidermal autoimmune blistering diseases:
9. Past Medical History
- Prior episodes of blistering or unexplained pruritus (may represent undiagnosed nonbullous BP) [4]
- Neurological diagnoses: dementia, Parkinson disease, stroke, epilepsy, MS [13][17]
- Diabetes mellitus and current antidiabetic regimen (DPP-4 inhibitor use) [5]
- Active or prior malignancy — especially if on checkpoint inhibitor therapy [19]
- History of osteoporosis, peptic ulcer disease, diabetes (impacts corticosteroid safety)
- Immunosuppression history
- Renal/hepatic function (affects choice of steroid-sparing agents)
10. Physical Exam
- Tense, dome-shaped bullae (1–3 cm) on erythematous or normal skin — hallmark finding [1][3][8]
- Distribution: flexural surfaces of limbs, trunk, groin; may be generalized [10]
- Urticarial plaques, eczematous patches, excoriations (nonbullous phase) [2][4]
- Nikolsky sign negative (positive in pemphigus) [15]
- Erosions with serous or hemorrhagic crusting at sites of ruptured bullae
- Assess for secondary infection: erythema, warmth, purulence, malodor
- Mucosal exam: oral, conjunctival, genital (involved in <30% of BP) [9]
- No scarring or milia (distinguishes from EBA and cicatricial pemphigoid) [10]
- Count new blisters: ≤10/day = moderate; >10/day = severe [11]
- Vital signs: fever (infection), tachycardia, hypotension (sepsis)
11. Lab Studies
- CBC with differential: peripheral eosinophilia is common and supportive [19]
- Anti-BP180 NC16A ELISA: pooled sensitivity ~82%, specificity ~94% — most useful serologic test; levels correlate with disease activity and relapse risk [13][29]
- Anti-BP230 ELISA: lower sensitivity (~59%) but high specificity (~95%); best used as adjunctive/confirmatory [29]
- Combined BP180 + BP230 ELISA sensitivity reaches ~90% [13]
- Total serum IgE: often elevated in BP
- BMP, glucose, HbA1c: baseline before corticosteroid initiation
- LFTs, CBC: baseline before immunosuppressive agents
- TPMT activity: if azathioprine is considered
- Wound culture if secondary infection suspected
12. Imaging
- No specific imaging is required for diagnosis of BP
- Chest X-ray if concern for pneumonia (BP patients have 3× higher pneumonia risk) [13]
- Age-appropriate cancer screening — weak and controversial association with malignancy; routine screening beyond standard guidelines is not recommended [13][30]
- Brain imaging only if new neurological symptoms warrant evaluation
13. Special Tests
- Skin biopsy (lesional): subepidermal blister with eosinophilic infiltrate on H&E — supportive but not specific [11]
- Direct immunofluorescence (DIF) of perilesional skin: gold standard — linear IgG and/or C3 deposits along the basement membrane zone; sensitivity ~91%, specificity ~98% [11][31]
- Indirect immunofluorescence (IIF) on salt-split skin: epidermal-side binding of IgG distinguishes BP from EBA (dermal-side binding) [11]
- C3d immunohistochemistry: comparable diagnostic utility to DIF; can be performed on formalin-fixed tissue [32]
- Bullous Pemphigoid Disease Area Index (BPDAI): validated scoring system for disease severity and treatment response [12]
A proposed "2-out-of-3 rule" for diagnosis: (1) pruritus and/or predominant cutaneous blisters, (2) linear IgG/C3 on DIF, (3) positive epidermal-side staining on IIF salt-split skin [4]
14. ECG
- ECG is not part of the standard BP workup but should be obtained in elderly patients as part of baseline assessment, particularly before initiating systemic corticosteroids
- BP is associated with a 5-fold higher cardiovascular disease mortality; cardiovascular comorbidities are common in this population [14][30][33]
- Monitor for QTc prolongation if using azithromycin or other QT-prolonging agents concurrently
- Corticosteroid-induced hypokalemia may cause arrhythmias — monitor electrolytes
15. Assessment
Severity stratification: [11-12]
- Mild: localized disease, few blisters, manageable pruritus
- Moderate: ≤10 new blisters/day
- Severe/extensive: >10 new blisters/day, widespread involvement
BP is a chronic disease with a 1-year mortality of 20–40%, approximately 2–3× higher than age-matched controls. [13] Death is most commonly due to infection (pneumonia, sepsis) and cardiovascular disease, often compounded by treatment-related adverse effects. [13][30] Atypical/nonbullous presentations (urticarial, eczematous, prurigo-like) are common and frequently misdiagnosed, leading to diagnostic delay. [4]
16. Treatment Plan
Initial stabilization
- Wound care: gentle cleansing, non-adherent dressings, lance large tense bullae with sterile technique (leave roof intact)
- Antihistamines for pruritus (cetirizine, hydroxyzine)
- Discontinue suspected offending medications (DPP-4 inhibitors, checkpoint inhibitors) [5][7]
Pharmacotherapy by severity
- Mild/localized: Topical clobetasol propionate 0.05% to affected areas [3][13]
- Moderate: Whole-body clobetasol propionate (10–30 g/day, tapered over 4 months) OR oral prednisolone 0.5 mg/kg/day OR doxycycline 200 mg/day [11][21]
- Severe/extensive: Whole-body clobetasol propionate 40 g/day (tapered over 12 months) OR oral prednisolone 0.5 mg/kg/day + steroid-sparing agent [11][13]
- Refractory: Rituximab, omalizumab, dupilumab (FDA-approved), IVIG, or JAK inhibitors [22-23]
Steroid-sparing agents (for corticosteroid taper or contraindication): doxycycline, azathioprine, mycophenolate mofetil, methotrexate, dapsone [11][13]
Monitoring on treatment: glucose, blood pressure, bone density (if prolonged steroids); CBC, LFTs (if on immunosuppressants); anti-BP180 levels to guide taper (high levels at discontinuation predict relapse) [13]
17. Disposition
Admission criteria
- Extensive/severe disease (>10 new blisters/day) with inability to manage wound care at home
- Secondary infection with systemic signs (sepsis, cellulitis)
- Significant comorbidities precluding safe outpatient management (frail elderly, dementia, no caregiver)
- Need for initiation of systemic immunosuppression with close monitoring
- Fluid/electrolyte imbalance from extensive skin loss
Discharge criteria
- Disease control achieved (no new blisters for ≥2 weeks)
- Stable on oral regimen with adequate wound care plan
- Caregiver available for topical medication application if needed
Specialist consultation
- Dermatology — all suspected cases for biopsy, DIF, and treatment guidance
- Ophthalmology if ocular symptoms (rule out ocular cicatricial pemphigoid)
- Neurology if new neurological symptoms
- Infectious disease if complicated wound infections
18. Follow Up / Return Precautions
Follow-up timing
- Dermatology within 1–2 weeks of diagnosis for biopsy results and treatment adjustment
- Every 2–4 weeks during active disease until control achieved
- Monthly during taper; every 2–3 months once in remission
- Anti-BP180 ELISA levels can guide taper decisions [13]
Return precautions — instruct patients/caregivers to seek care for:
- New blister flare or worsening pruritus despite treatment
- Signs of skin infection: increasing redness, warmth, pus, fever
- Symptoms of steroid side effects: confusion, blood sugar changes, GI bleeding, leg swelling
- Shortness of breath, chest pain (pneumonia, PE — 3× increased risk) [13]
- Falls, fractures (steroid-induced osteoporosis in elderly)
Expected course: BP is chronic with exacerbations and remissions. Many patients achieve remission within 1–5 years, but relapse is common, particularly if anti-BP180 antibody levels remain elevated at treatment discontinuation. [13] Mortality is significantly elevated in the first year, driven by infection and cardiovascular events. [13][30]
References
1. Bullous Pemphigoid. — Akbarialiabad H, Schmidt E, Patsatsi A, et al. Nature Reviews. Disease Primers. 2025.
2. Bullous Pemphigoid: A Review of Its Diagnosis, Associations and Treatment. — Bernard P, Antonicelli F. American Journal of Clinical Dermatology. 2017.
3. Bullous Pemphigoid. — Bağcı IS, Horváth ON, Ruzicka T, Sárdy M. Autoimmunity Reviews. 2017.
4. Assessment of Diagnostic Strategy for Early Recognition of Bullous and Nonbullous Variants of Pemphigoid. — Meijer JM, Diercks GFH, de Lang EWG, Pas HH, Jonkman MF. JAMA Dermatology. 2019.
5. Exploration of Drugs Associated With the Development of Bullous Pemphigoid: A Nationwide Study. — Kim MJ, Kim BR, Lee KH, et al. The Journal of Dermatology. 2025.
6. Association Between Medication Use and Bullous Pemphigoid: A Systematic Review and Meta-analysis. — Liu SD, Chen WT, Chi CC. JAMA Dermatology. 2020.
7. A Systematic Review of Drug-Induced Pemphigoid. — Verheyden MJ, Bilgic A, Murrell DF. Acta Dermato-Venereologica. 2020.
8. Bullous Pemphigoid. — Korman N. Journal of the American Academy of Dermatology. 1987.
9. Bullous Autoimmune Dermatoses. — Hofmann SC, Juratli HA, Eming R. Journal Der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2018.
10. Evaluation of Clinical Criteria for Diagnosis of Bullous Pemphigoid. — Vaillant L, Bernard P, Joly P, et al. Archives of Dermatology. 1998.
11. Interventions for Bullous Pemphigoid. — Singh S, Kirtschig G, Anchan VN, et al. The Cochrane Database of Systematic Reviews. 2023.
12. International Multicentre Observational Study to Assess the Efficacy and Safety of a 0·5 Mg Kg Per Day Starting Dose of Oral Corticosteroids to Treat Bullous Pemphigoid. — Hébert V, Bastos S, Drenovska K, et al. The British Journal of Dermatology. 2021.
13. Pemphigoid Diseases. — Schmidt E, Zillikens D. Lancet. 2013.
14. Comorbid Diseases in Bullous Pemphigoid: A Population-Based Case-Control Study. — Kim BR, Lee KH, Paik K, et al. The Journal of Dermatology. 2025.
15. Review of Autoimmune Blistering Diseases: The Pemphigoid Diseases. — Daniel BS, Murrell DF. Journal of the European Academy of Dermatology and Venereology : JEADV. 2019.
16. Autoimmune Subepidermal Bullous Diseases of the Skin and Mucosae: Clinical Features, Diagnosis, and Management. — Amber KT, Murrell DF, Schmidt E, Joly P, Borradori L. Clinical Reviews in Allergy & Immunology. 2018.
17. Bullous Pemphigoid and Its Association With Neurological Diseases: A Systematic Review and Meta-Analysis. — Lai YC, Yew YW, Lambert WC. Journal of the European Academy of Dermatology and Venereology : JEADV. 2016.
18. Association Between DPPs-4 Inhibitors and Bullous Pemphigoid: Reporting Odds Ratio Analysis Using EudraVigilance Database. — Pedrero AC, Aldea-Perona A. Pharmaceuticals. 2025.
19. Association of Bullous Pemphigoid With Immune Checkpoint Inhibitor Therapy in Patients With Cancer: A Systematic Review. — Asdourian MS, Shah N, Jacoby TV, Reynolds KL, Chen ST. JAMA Dermatology. 2022.
20. Association of Statins, Gliptins, and Antipsychotics With Bullous Pemphigoid: A Case-Control Study in the Cretan Population. — Kavvalou E, Krasagakis K, Chlouverakis G, et al. The Journal of Dermatology. 2025.
21. Doxycycline Versus Prednisolone as an Initial Treatment Strategy for Bullous Pemphigoid: A Pragmatic, Non-Inferiority, Randomised Controlled Trial. — Williams HC, Wojnarowska F, Kirtschig G, et al. Lancet. 2017.
22. FDA Orange Book. — FDA Orange Book. 2026.
23. Advancements in Bullous Pemphigoid Treatment: A Comprehensive Pipeline Update. — Karakioulaki M, Eyerich K, Patsatsi A. American Journal of Clinical Dermatology. 2024.
24. Demographics and Autoantibody Profiles of Pemphigoid Patients With Underlying Neurologic Diseases. — Messingham KN, Miller AD, Narayanan NS, Connell SJ, Fairley JA. The Journal of Investigative Dermatology. 2019.
25. A Population-Based Study of the Association Between Bullous Pemphigoid and Neurologic Disorders. — Brick KE, Weaver CH, Savica R, et al. Journal of the American Academy of Dermatology. 2014.
26. Association of Genetic Variants of HLA-DQA1 With Bullous Pemphigoid Induced by Dipeptidyl Peptidase-4 Inhibitors. — Ozeki T, Muramatsu K, Yoshimoto N, et al. The Journal of Investigative Dermatology. 2023.
27. Subepithelial Autoimmune Blistering Dermatoses: Clinical Features and Diagnosis. — Montagnon CM, Tolkachjov SN, Murrell DF, Camilleri MJ, Lehman JS. Journal of the American Academy of Dermatology. 2021.
28. Immunobullous diseases. — Rook's Dermatology Handbook. 2023.
29. Sensitivity and Specificity of ELISA Tests Detecting BP180 and BP230 Antibodies in the Diagnosis of Bullous Pemphigoid: A Systematic Review and Meta-Analysis. — Grochowska-Rak M, Kulig K, Grabowska A, et al. International Journal of Dermatology. 2025.
30. Risk of All-Cause Mortality, Cardiovascular Disease Mortality, and Cancer Mortality in Patients With Bullous Pemphigoid. — Shen WC, Chiang HY, Chen PS, et al. JAMA Dermatology. 2022.
31. Comparative Study of Direct and Indirect Immunofluorescence and of Bullous Pemphigoid 180 and 230 Enzyme-Linked Immunosorbent Assays for Diagnosis of Bullous Pemphigoid. — Sárdy M, Kostaki D, Varga R, Peris K, Ruzicka T. Journal of the American Academy of Dermatology. 2013.
32. Comparison of C3d Immunohistochemical Staining to Enzyme-Linked Immunosorbent Assay and Immunofluorescence for Diagnosis of Bullous Pemphigoid. — Wang LL, Moshiri AS, Novoa R, et al. Journal of the American Academy of Dermatology. 2020.
33. A Retrospective Consecutive Case-Series Study on the Effect of Systemic Treatment, Length of Admission Time, and Co-Morbidities in 98 Bullous Pemphigoid Patients Admitted to a Tertiary Centre. — Kibsgaard L, Bay B, Deleuran M, Vestergaard C. Acta Dermato-Venereologica. 2015.