Cyanide Poisoning
Cyanide is one of the most rapidly lethal poisons, inhibiting mitochondrial cytochrome oxidase and blocking cellular respiration (oxidative phosphorylation), leading to cellular hypoxia despite nor…
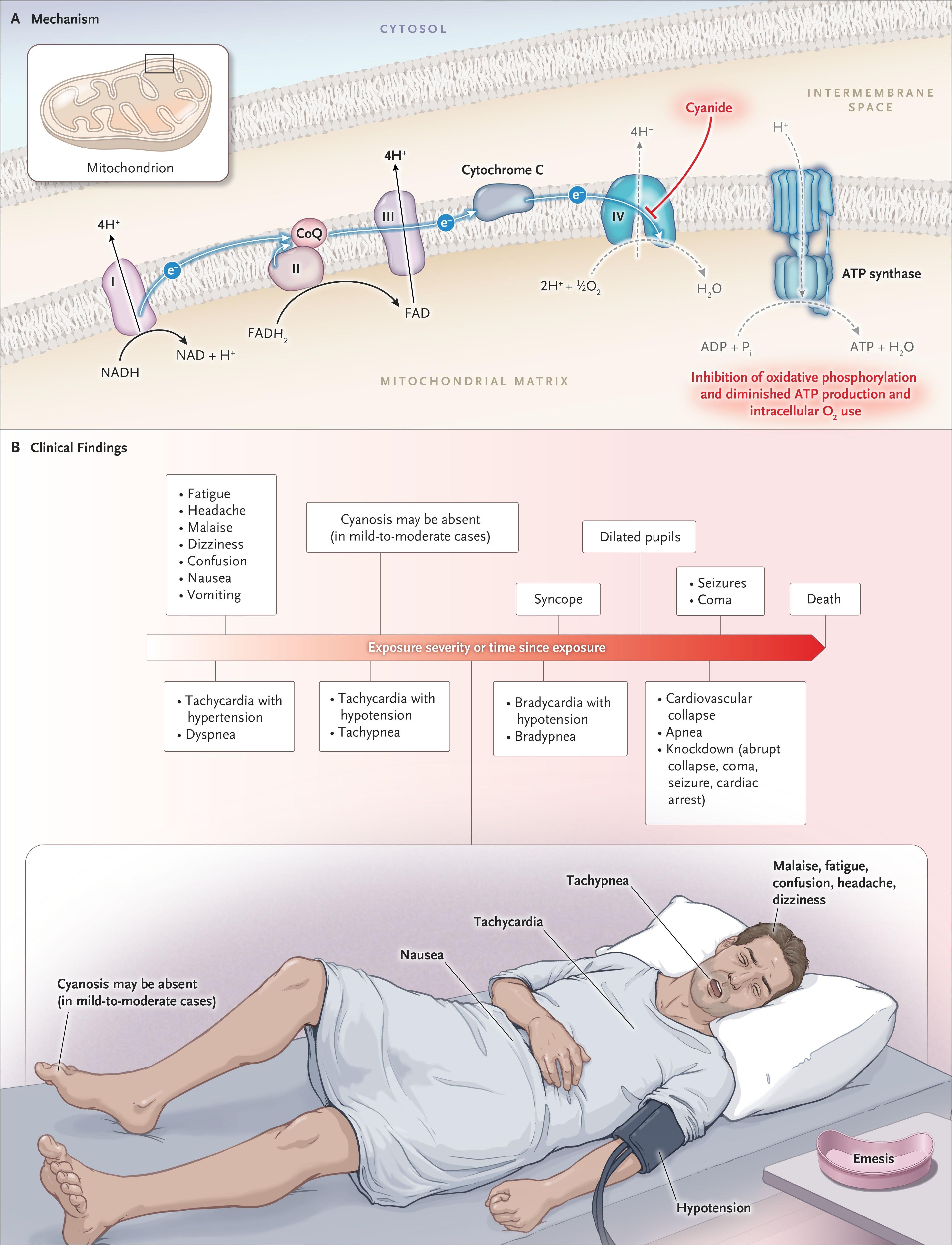
Cyanide is one of the most rapidly lethal poisons, inhibiting mitochondrial cytochrome oxidase and blocking cellular respiration (oxidative phosphorylation), leading to cellular hypoxia despite normal arterial oxygen levels. [1-2] The most common source of exposure in clinical practice is smoke inhalation from structure fires, where concomitant carbon monoxide poisoning is frequent. [1][3-4] Diagnosis is clinical — there is no widely available rapid confirmatory test — and empirical antidote administration should not be delayed. [3][5]
The following figure from the NEJM illustrates the mechanism of cyanide toxicity at the mitochondrial level and the clinical progression from early symptoms to cardiovascular collapse:
1. History
- Exposure context: Structure fire/smoke inhalation in enclosed space, industrial/laboratory accident (electroplating, metallurgy, jewelry cleaning), ingestion of cyanide salts or cyanogenic compounds (amygdalin, acetonitrile, apricot pits), sodium nitroprusside infusion, intentional self-harm [1-2]
- Route: Inhalation (most rapid onset — seconds to minutes), ingestion, dermal absorption [5]
- Timing: Inhalation → symptoms within seconds; ingestion of salts → minutes; ingestion of cyanogenic compounds (e.g., acetonitrile) → delayed onset up to hours [2]
- Symptom progression: Headache, confusion, dizziness, nausea/vomiting → dyspnea, chest tightness → altered mental status, seizures → cardiovascular collapse, apnea [5-6]
- Important negatives: Ask about co-exposures (CO, other toxic gases), duration in enclosed space, presence of soot in airway
2. Alarm Features
- Cardiac arrest (OR 36.4 for fatal outcome) [7]
- Hypotension (OR 15.8 for fatal outcome) [7]
- Coma/unresponsiveness (OR 10.8 for fatal outcome) [7]
- Lactic acidosis (OR 7.8 for fatal outcome); lactate >10 mmol/L in smoke inhalation strongly associated with cyanide toxicity [2][7]
- Seizures — indicate severe poisoning [1]
- Apnea/bradypnea — late finding indicating imminent arrest [5]
- Rapid progression from initial symptoms to cardiovascular collapse can occur within minutes [8]
3. Medications
Antidotes (see Treatment Plan for dosing)
- Hydroxocobalamin (Cyanokit) — first-line, preferred agent [1][3]
- Sodium nitrite + sodium thiosulfate (Cyanide Antidote Kit) — alternative when hydroxocobalamin unavailable [1][6]
- Sodium thiosulfate alone — too slow for monotherapy in life-threatening cases but may be used adjunctively [1]
Medication contributors to cyanide toxicity
- Sodium nitroprusside[2]
Contraindications/cautions
- Sodium nitrite is relatively contraindicated in smoke inhalation with suspected CO co-poisoning (methemoglobin formation further reduces O₂-carrying capacity) [1]
- Sodium nitrite dosing must be precise in children and anemic patients to avoid excessive methemoglobinemia [1][3]
- Hydroxocobalamin and sodium thiosulfate are chemically incompatible — do not administer through the same IV line [6]
4. Diet
- Cyanogenic foods: Cassava (linamarin), bitter almonds, apricot/peach/cherry pits (amygdalin), lima beans — chronic ingestion can cause subacute cyanide toxicity [1][9]
- Not applicable in the acute ED setting; relevant for chronic/subacute exposure history and public health counseling
5. Review of Systems
- Neuro: Headache, dizziness, confusion, agitation, seizures, loss of consciousness
- Cardiovascular: Chest tightness, palpitations, syncope
- Respiratory: Dyspnea, tachypnea (early), apnea (late)
- GI: Nausea, vomiting
- Skin: Ask about burns, soot exposure (smoke inhalation context)
- Psychiatric: Suicidal ideation (intentional ingestion)
6. Collateral History and Family History
- Critical collateral: Bystanders, EMS, fire department — nature of fire, enclosed vs. open space, duration of exposure, materials burning (plastics, vinyl, wool = higher cyanide risk) [1]
- Coworkers in industrial/laboratory exposures — identify the specific cyanide compound
- Family/friends for intentional ingestion — access to cyanide salts, suicide note, psychiatric history
- Family history is generally not relevant in acute poisoning
7. Risk Factors
- Smoke inhalation in enclosed-space fires — most common clinical scenario [1][4]
- Occupational exposure: Electroplating, metallurgy, jewelry cleaning, photography, laboratory work, mining [1-2]
- Intentional self-harm or criminal poisoning (rare) [1]
- Sodium nitroprusside therapy — especially prolonged infusions [2]
- Ingestion of cyanogenic plants/compounds — most common in children <5 years (plant material ingestion), though usually mild [7]
8. Differential Diagnosis
- Carbon monoxide poisoning — overlapping presentation in fire victims; check COHb level; can coexist with cyanide [2][4]
- Hydrogen sulfide poisoning — occupational (sewers, enclosed spaces); rotten-egg odor; "gas eye" corneal ulcerations [2]
- Methemoglobinemia — cyanosis, chocolate-brown blood; check co-oximetry
- Severe sepsis/septic shock — lactic acidosis, hypotension, altered mental status; but different exposure history
- Other mitochondrial toxins: Azide poisoning, metformin-associated lactic acidosis
- Opioid overdose — CNS depression, apnea, miosis (vs. mydriasis in cyanide) [1]
- Cardiac arrest from other causes — in fire victims, consider thermal airway injury, hypoxia from O₂ displacement
Key distinguishing feature: Cyanide causes elevated mixed venous O₂ saturation (cells cannot extract oxygen) — this is uncharacteristic of most other causes of shock [2]
9. Past Medical History
- Anemia — increases risk from sodium nitrite (reduced O₂-carrying capacity reserve) [1][3]
- Cardiac disease — lower threshold for cardiovascular collapse
- Chronic cyanide exposure — may cause thyroid dysfunction [8]
- Psychiatric history — relevant for intentional ingestion
- Previous episodes of poisoning or self-harm
10. Physical Exam
Vital signs
- Early: Tachycardia, hypertension, tachypnea/hyperpnea [5-6]
- Late: Bradycardia, hypotension, bradypnea/apnea [5-6]
Focused exam
- Neuro: GCS, pupil exam (mydriasis is suggestive), seizure activity [5-6]
- Airway: Soot around mouth/nose/oropharynx (smoke inhalation), stridor, hoarseness [6]
- Skin: Burns, soot; cherry-red skin is classically described but rare (11% of cases) and unreliable; cyanosis may be absent in mild-moderate cases [2][10]
- Odor: Bitter-almond breath odor — described but uncommon (15% of cases), and ~40% of the population cannot detect it genetically [10]
- Most patients in published case series were unresponsive (78%), had respiratory failure (73%), and were hypotensive (54%) [10]
11. Lab Studies
- ABG/VBG: Severe high-anion-gap metabolic acidosis — the most consistent laboratory finding [1-2][10]
- Lactate: The single most useful lab value
- ≥8 mmol/L — sensitive (94%) for toxic cyanide levels; moderately specific (70%), improved to 85% in patients not on vasopressors [11]
- >10 mmol/L in smoke inhalation — strongly associated with cyanide toxicity [2]
- >11 mmol/L — associated with fatal outcome (sensitivity 74%, specificity 80%) [7]
- Serial lactate monitoring is useful for tracking treatment response [12]
- Co-oximetry: COHb level (rule out concomitant CO poisoning); note hydroxocobalamin interferes with colorimetric COHb measurement [2][5]
- BMP: Anion gap, electrolytes, renal function
- Mixed venous O₂ saturation: Elevated (narrowed arteriovenous O₂ gap) — cells cannot utilize oxygen [2]
- Blood cyanide level: Confirmatory but not available in real time in most hospitals; >1.0 mg/L is toxic. Do not delay treatment awaiting results [3][5][11]
- CBC: Baseline hemoglobin (relevant for sodium nitrite dosing)
12. Imaging
- CXR: Evaluate for concomitant inhalation injury, pulmonary edema, aspiration (especially in smoke inhalation)
- CT head: Consider if prolonged altered mental status persists after treatment — evaluate for anoxic brain injury
- Imaging is generally not diagnostic for cyanide poisoning itself; it is used to evaluate complications and co-injuries
13. Special Tests
- Point-of-care lactate — most critical bedside test for supporting diagnosis and monitoring treatment [11-12]
- Co-oximetry — essential in smoke inhalation to assess COHb and methemoglobin levels
- Poison Control Center consultation (1-800-222-1222 in the US) — recommended for all suspected cases [1][5]
- Whole blood cyanide level — send if available, but results are typically delayed hours to days [3]
14. ECG
- Obtain ECG on all patients — cardiac complications are common (reported in 84% of fire-related cyanide cases) [13]
- Findings:
- Sinus tachycardia (early) → bradycardia (late/ominous) [5]
- Supraventricular tachycardia — most common rhythm disturbance (35% in one series) [13]
- Repolarization abnormalities (ST-T wave changes) [13]
- Conduction delays [13]
- Asystole — most common arrest rhythm (95% of cardiac arrests in one series were asystole, 5% VF) [13]
- Pulseless electrical activity (PEA) — described at higher levels of intoxication [14]
- Cyanide itself may prolong APD and depolarize resting membrane potential at the cellular level [15]
15. Assessment
Severity stratification
- Mild: Headache, dizziness, nausea, anxiety, tachypnea — may mimic panic symptoms [5]
- Moderate: Confusion, disorientation, mydriasis, vomiting, tachycardia, hypertension
- Severe: Coma, seizures, cardiovascular collapse, apnea, cardiac arrest, lactate ≥8 mmol/L [5-6]
Key clinical pearls
- Diagnosis is clinical and presumptive — do not wait for confirmatory testing [3][5]
- Cherry-red skin and bitter-almond odor are unreliable — absent in the majority of cases [10]
- The presence of altered mental status and/or mydriasis is more suggestive of true cyanide poisoning than panic-related tachypnea/vomiting [5]
- In smoke inhalation, always consider dual CO + cyanide poisoning [1][4]
- Survivors of significant poisoning can have long-term neurologic dysfunction [16]
16. Treatment Plan
Initial stabilization (do not delay for antidote)
- Airway: Intubate if GCS depressed, apneic, or airway compromise (66% of cases required intubation) [10]
- 100% FiO₂: Administer to all patients — beneficial despite normal PaO₂ [1]
- Decontamination: Remove from exposure, remove clothing, dermal decontamination for liquid exposure [2]
- GI decontamination: Consider for cyanide/cyanogenic compound ingestion [2]
- Vasopressors: 39% of cases required vasopressor support for refractory hypotension [10]
- Seizure management: Benzodiazepines
Antidote therapy
- Redosing: If signs recur, repeat half the original dose of sodium nitrite and sodium thiosulfate [6]
- Hydroxocobalamin may be repeated at full dose (5 g) for severe cases [2][5]
- Monitor blood pressure during all antidote administration [6]
17. Disposition
Admit to ICU
- Cardiac arrest, hemodynamic instability, or vasopressor requirement
- Seizures, coma, or persistent altered mental status
- Severe lactic acidosis (lactate ≥8 mmol/L)
- Required antidote administration
- Concomitant significant CO poisoning or inhalation injury
Observation
- Mild symptoms with rapid resolution after decontamination and supportive care
- Asymptomatic patients with concerning exposure history — observe minimum 4–6 hours (longer for cyanogenic compound ingestion due to delayed metabolism)
Discharge considerations
- Asymptomatic after observation period with normal lactate and no acidosis
- Psychiatric evaluation mandatory before discharge for intentional ingestions
Consult triggers
- Toxicology/Poison Control (1-800-222-1222) — all suspected cases [1]
- Burn surgery — concomitant burns
- Pulmonology/critical care — inhalation injury
- Hyperbaric medicine — if significant concomitant CO poisoning [2]
- Psychiatry — intentional ingestion
Prognosis: Mortality is high once cardiac arrest occurs — only 13% survival in patients who received hydroxocobalamin while in cardiac arrest. [3] Among non-arrest patients treated with hydroxocobalamin, survival is approximately 72–78%. [3]
18. Follow Up / Return Precautions
- Survivors of significant poisoning should be monitored for delayed neurologic sequelae (parkinsonian features, cognitive deficits, personality changes) — similar to post-anoxic injury [16]
- Follow-up timing: Neurology follow-up within 1–2 weeks for patients with any period of altered consciousness
- Occupational exposure: Ensure workplace safety evaluation and OSHA reporting before return to work
- Return precautions: Return immediately for recurrent headache, confusion, dizziness, chest pain, shortness of breath, or any neurologic symptoms
- Thyroid function: Consider monitoring in patients with chronic/subacute cyanide exposure [8]
- Psychiatric follow-up: Mandatory for intentional ingestions
References
1. 2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Lavonas EJ, Akpunonu PD, Arens AM, et al. Circulation. 2023.
2. Hazardous Chemical Emergencies and Poisonings. — Henretig FM, Kirk MA, McKay CA. The New England Journal of Medicine. 2019.
3. Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Cao D, Arens AM, Chow SL, et al. Circulation. 2025.
4. Smoke-Inhalation Victims in a Tertiary ED: Prevalence of Presumed Hydrogen-Cyanide Co-Poisoning and Clinical Correlates. — Lobo-Antuña V, Lobo-Antuña M, Fernández-Soro A, et al. Internal and Emergency Medicine. 2026.
5. FDA Drug Label. — Updated date: 2023-04-27. Food and Drug Administration.
6. FDA Drug Label. — Updated date: 2025-10-06. Food and Drug Administration.
7. Potential Cyanide Poisoning Reported to the UK National Poisons Information Service: 2008-2019. — Haden M, Wheatley N, Gray LA, et al. Clinical Toxicology. 2022.
8. Cyanide Toxicity. Agency for Toxic Substances and Disease Registry. — American Family Physician. 1993.
9. Cyanide and Cyanogenic Compounds-Toxicity, Molecular Targets, and Therapeutic Agents. — Lachowicz JI, Alexander J, Aaseth JO. Biomolecules. 2024.
10. Challenges in the Diagnosis of Acute Cyanide Poisoning. — Parker-Cote JL, Rizer J, Vakkalanka JP, Rege SV, Holstege CP. Clinical Toxicology. 2018.
11. Value of Lactic Acidosis in the Assessment of the Severity of Acute Cyanide Poisoning. — Baud FJ, Borron SW, Mégarbane B, et al. Critical Care Medicine. 2002.
12. A Case Report of Acute Cyanide Poisoning Treated With Lactate as an Indicator. — Suzuki M, Takeda S, Sugaya K, et al. Medicine. 2025.
13. Cyanide Poisoning and Cardiac Disorders: 161 Cases. — Fortin JL, Desmettre T, Manzon C, et al. The Journal of Emergency Medicine. 2010.
14. Circulatory Failure During Noninhaled Forms of Cyanide Intoxication. — Haouzi P, Tubbs N, Rannals MD, et al. Shock. 2017.
15. Methylene Blue Counteracts Cyanide Cardiotoxicity: Cellular Mechanisms. — Cheung JY, Wang J, Zhang XQ, et al. Journal of Applied Physiology. 2018.
16. Cyanides. — Morocco AP. Critical Care Clinics. 2005.