Diverticulitis
Diverticulitis is inflammation of colonic diverticula (outpouchings of the intestinal wall), affecting approximately 180 per 100,000 people annually in the US and resulting in about 200,000 hospita…
Diverticulitis is inflammation of colonic diverticula (outpouchings of the intestinal wall), affecting approximately 180 per 100,000 people annually in the US and resulting in about 200,000 hospitalizations per year. [1-2]
Clinical Presentation
Patients typically present with left lower quadrant pain associated with nausea, vomiting, fever, and leukocytosis. [1] Rectal bleeding is not commonly seen in acute diverticulitis. [3] Approximately 85% of cases are uncomplicated (localized inflammation without abscess, perforation, fistula, or obstruction), while 12-15% are complicated. [1][3]
Diagnosis
Contrast-enhanced CT scan of the abdomen and pelvis is the recommended diagnostic test, with sensitivity of 98-99% and specificity of 99-100%. [1] Abdominal ultrasound may also be used, particularly in the emergency department. [2] Clinical diagnosis alone is only accurate in 40-65% of patients, making imaging essential for confirmation. [3]
Management
The following algorithm illustrates the comprehensive approach to diverticulitis management:
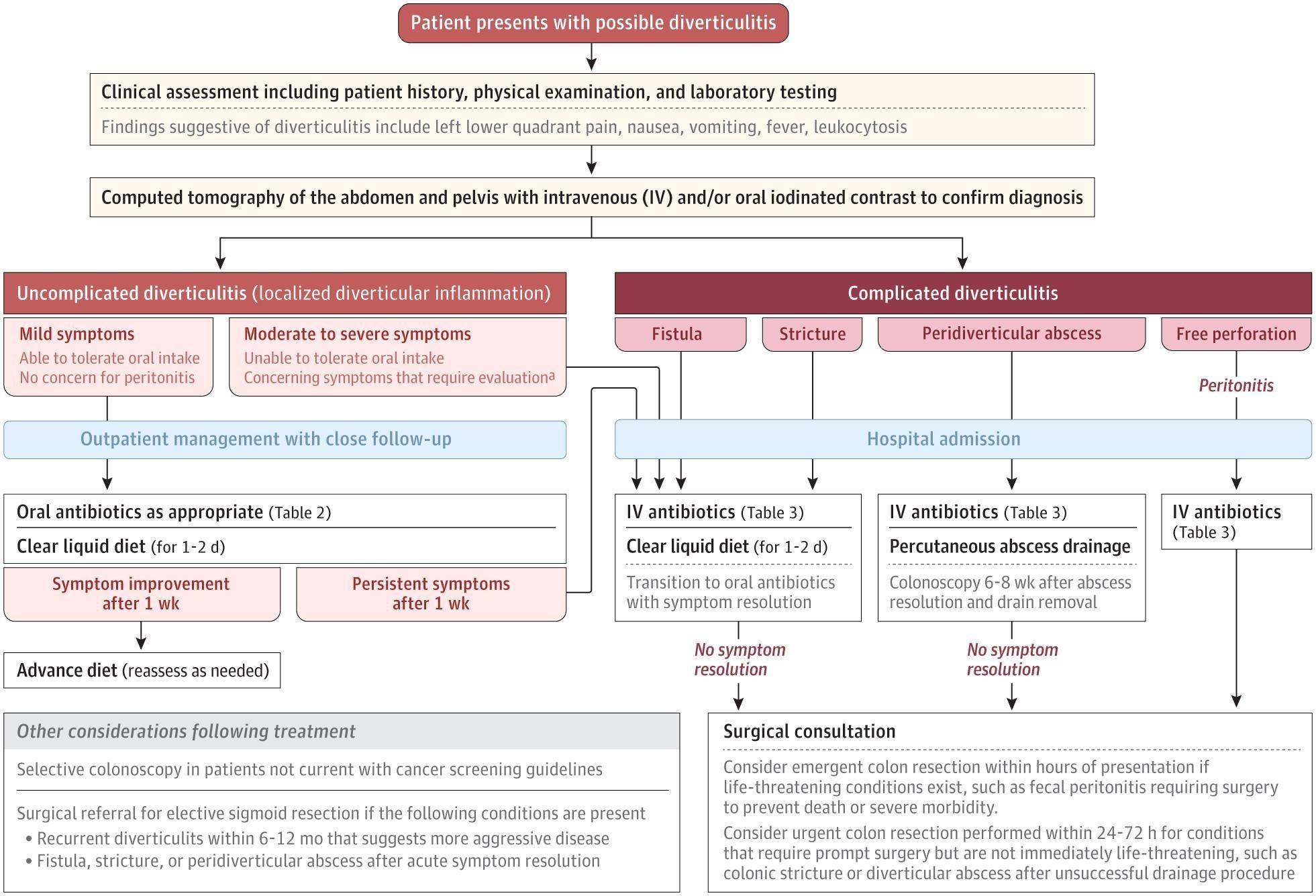
Uncomplicated Diverticulitis
- First-line therapy: Observation with pain management (typically acetaminophen) and dietary modification (clear liquid diet for 1-2 days) [1-2]
- Selective antibiotic use is recommended for patients with: [1][4-5]
- Persistent fever or systemic symptoms
- Age >80 years
- Pregnancy
- Immunocompromise (chemotherapy, high-dose steroids, organ transplant)
- Chronic medical conditions (cirrhosis, chronic kidney disease, heart failure, poorly controlled diabetes)
- High-risk features: CRP >140 mg/L, WBC >15 × 10⁹/L, symptoms >5 days, vomiting, or CT findings of fluid collection or longer inflamed segment
- Outpatient oral antibiotics (7-10 days): [1][6]
- Amoxicillin-clavulanate 875 mg twice daily, OR
- Ciprofloxacin 500 mg twice daily plus metronidazole 500 mg three times daily, OR
- Cephalexin plus metronidazole
- Inpatient management indicated for high fever (>101.5°F), leukocytosis, complicated disease, immunosuppression, serious comorbidities, or inability to tolerate oral intake [6]
Complicated Diverticulitis
- Intravenous antibiotics: [1]
- Ceftriaxone plus metronidazole, OR
- Piperacillin-tazobactam, OR
- Ampicillin-sulbactam
- Percutaneous drainage for abscesses ≥3-5 cm [7-8]
- Emergent surgery (colonic resection) for generalized peritonitis or failure of non-operative management [1][7]
Follow-up
Colonoscopy is recommended 6-8 weeks after diagnosis to exclude colon malignancy, particularly in complicated diverticulitis (6-8% CRC risk) or when suspicious features are present on CT. [3][7-8]
Risk Factors
Age >65 years, obesity (BMI ≥30), genetic factors (TNFSF15 gene variants), connective tissue disorders, NSAID/opioid/steroid use, hypertension, and type 2 diabetes. [1]
References
1. Diverticulitis. — Brown RF, Lopez K, Smith CB, Charles A. The Journal of the American Medical Association. 2025.
2. What Is Diverticulitis?. — Narayanan S, Jackson CD. The Journal of the American Medical Association. 2025.
3. Colorectal Cancer Screening and Surveillance and Other Colon Conditions in the Older Adult. — Calderwood AH, Shaukat A. The American Journal of Gastroenterology. 2025.
4. AGA Clinical Practice Update on Medical Management of Colonic Diverticulitis: Expert Review. — Peery AF, Shaukat A, Strate LL. Gastroenterology. 2021.
5. Diagnosis and Management of Acute Left-Sided Colonic Diverticulitis: A Clinical Guideline From the American College of Physicians. — Qaseem A, Etxeandia-Ikobaltzeta I, Lin JS, et al. Annals of Internal Medicine. 2022.
6. Diverticulitis. — Young-Fadok TM. The New England Journal of Medicine. 2018.
7. The Management of Diverticulitis: A Review of the Guidelines. — You H, Sweeny A, Cooper ML, Von Papen M, Innes J. The Medical Journal of Australia. 2019.
8. Management of Colonic Diverticulitis. — Peery AF. BMJ. 2021.