Failure to Cope (Social)
"Failure to cope" (also termed "failure to thrive" in adults, or "social admission") is a non-specific clinical label applied predominantly to older adults presenting to the ED when they can no lon…
"Failure to cope" (also termed "failure to thrive" in adults, or "social admission") is a non-specific clinical label applied predominantly to older adults presenting to the ED when they can no longer manage independently at home due to a combination of functional decline, loss of social supports, cognitive impairment, and/or unrecognized medical illness. Critically, 88% of patients admitted under this label are ultimately found to have an acute medical diagnosis at discharge, making thorough medical evaluation essential. [1]
1. History
- Functional baseline: What could the patient do independently 2 weeks ago vs. now? Assess ADLs (bathing, dressing, toileting, feeding, transferring) and IADLs (cooking, medications, finances, shopping, transportation) [2-3]
- Onset and trajectory: Acute (hours–days) vs. subacute (weeks) decline — acute onset suggests medical precipitant (infection, stroke, medication change, fall)
- Precipitating event: Recent fall, illness, hospitalization, medication change, loss of caregiver, bereavement, change in living situation
- Nutritional intake: Appetite changes, weight loss (>5% in 1 month or >10% in 6 months is significant), ability to prepare/access food [4-5]
- Medication adherence: Missed doses, confusion about regimen, recent additions/changes, polypharmacy (≥5 medications) [2]
- Mood and cognition: Screening for depression (PHQ-2), memory complaints, confusion, sleep disturbance
- Social supports: Who lives with the patient? Caregiver availability and burden? Recent loss of spouse/caregiver? Financial constraints? [6]
- Important negatives: Chest pain, dyspnea, fever, focal weakness, urinary symptoms, abdominal pain, suicidal ideation
2. Alarm Features
- Acute altered mental status or new confusion → delirium workup (infection, metabolic, medication, stroke) [7]
- New focal neurological deficits → stroke
- Fever or hypothermia → sepsis, UTI, pneumonia
- Signs of trauma inconsistent with history → elder abuse/neglect [8]
- Severe malnutrition, pressure ulcers, contractures → neglect (self or caregiver) [9]
- Suicidal ideation — elderly patients have the highest completed suicide rate
- Inability to ambulate or new immobility → fracture, spinal cord pathology, severe deconditioning
- Medication toxicity signs (bradycardia, hypotension, altered sensorium)
3. Medications
- Contributors to functional decline and falls: [10-12]
- Benzodiazepines, sedative-hypnotics (OR for falls ~2.05)
- Antipsychotics (OR ~2.30)
- Opioids (OR ~1.60)
- Anticholinergics (diphenhydramine, oxybutynin, TCAs)
- Loop diuretics (OR ~1.36–1.58)
- Antihypertensives (especially at initiation/dose change)
- Gabapentinoids, anticonvulsants
- SSRIs/SNRIs (OR ~1.48)
- Polypharmacy (≥5 medications): 21% higher fall rate; ≥10 medications: 50% higher [12]
- Medication review tools: AGS Beers Criteria, STOPPFall, Anticholinergic Burden Calculator [13]
- Common treatments to initiate (once medical causes addressed):
- Nutritional supplementation if malnourished
- Antidepressant if depression identified (prefer SSRI at lowest dose)
- Vitamin D supplementation for fall prevention
- Correct hypothyroidism, B12 deficiency, anemia [14]
- Contraindicated/avoid: New benzodiazepines, anticholinergics, unnecessary opioids
4. Diet
- Malnutrition prevalence: Up to 50% of acutely ill older adults in the ED meet GLIM criteria for malnutrition [15]
- Assessment: Mini Nutritional Assessment–Short Form (MNA-SF) is best validated; score <12 indicates risk [5]
- Key considerations:
- Ability to shop, prepare, and eat food independently
- Dental/denture problems causing dysphagia
- Financial barriers to food access (food insecurity)
- Meals on Wheels or congregate meal programs [4]
- Acute management: Oral nutritional supplements; avoid refeeding syndrome in severely malnourished
- Long-term: Dietitian referral, community food programs, address social isolation (most common social risk at 39%) [16]
5. Review of Systems
- Neuropsychiatric: Confusion, memory loss, depression, anxiety, sleep disturbance, hallucinations
- Constitutional: Weight loss, fatigue, anorexia, fever, night sweats
- Cardiovascular: Orthostasis, syncope, exertional dyspnea, edema
- Pulmonary: Cough, dyspnea
- GI: Dysphagia, abdominal pain, constipation, diarrhea, incontinence
- GU: Urinary frequency/urgency, incontinence, dysuria
- MSK: Joint pain, weakness, falls, gait instability
- Skin: Pressure injuries, rashes, poor hygiene
6. Collateral History and Family History
- Collateral is essential — contact family, caregivers, home health aides, neighbors, PCP [17-18]
- Baseline cognitive and functional status
- Timeline of decline
- Medication compliance
- Home environment safety
- Caregiver burden and fatigue (powerful predictor of institutionalization) [19]
- Family history: Dementia (Alzheimer's, frontotemporal), depression, Parkinson's disease, stroke
- Social context: Living alone (Z60.2), social isolation, financial hardship, recent bereavement, substance use
7. Risk Factors
- Age >75 years, especially >85 [20-21]
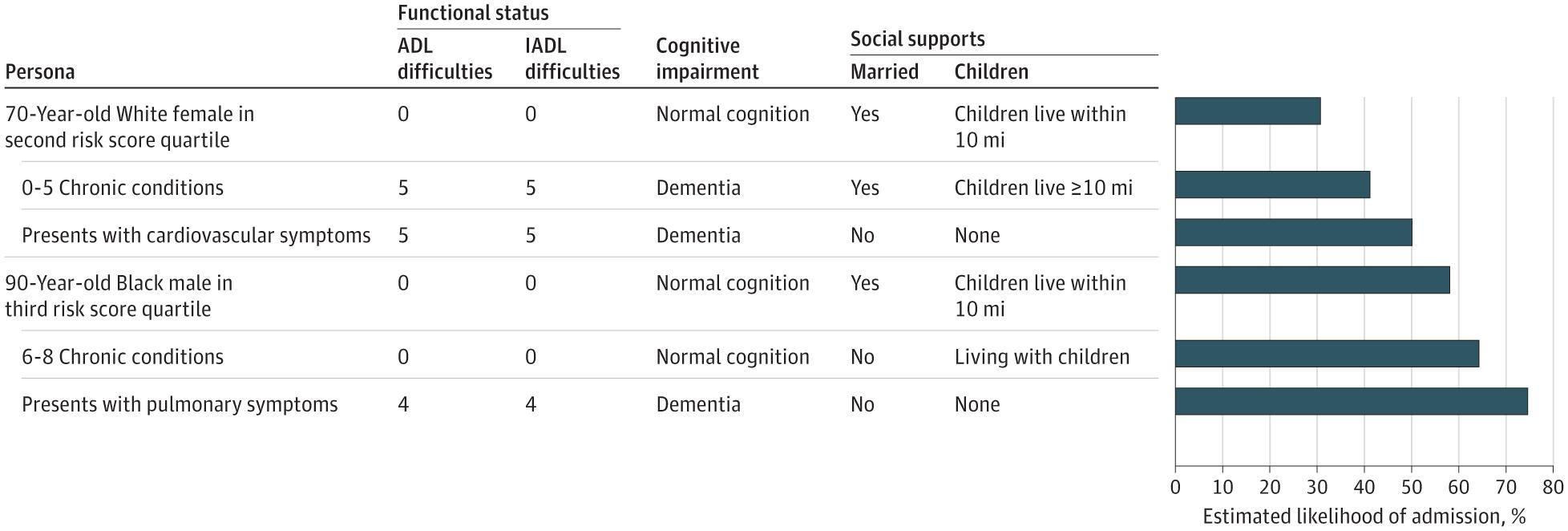
- Living alone without nearby family — children >10 miles away increases admission likelihood by 5 percentage points [6]
- Cognitive impairment/dementia — increases admission by 4.6 percentage points [6]
- Functional impairment — difficulty with 5 ADLs increases admission by 8.5 percentage points [6]
- Frailty (Clinical Frailty Scale ≥6) [14][22]
- Recent hospitalization or ED visit
- Polypharmacy
- Depression — leading cause of weight loss in long-term care [23]
- Caregiver loss or burnout [19]
- Low socioeconomic status, inadequate housing, food insecurity [16][24]
8. Differential Diagnosis
The label "failure to cope" should prompt a search for underlying medical causes — not serve as a final diagnosis.
- Infection: UTI, pneumonia, cellulitis (most common acute precipitant in elderly)
- Delirium: Medication-induced, metabolic, infectious — often superimposed on dementia [7]
- Depression: Major depressive disorder, adjustment disorder, grief
- Dementia progression: Alzheimer's, vascular, Lewy body, frontotemporal
- Medication toxicity/adverse effects: Overmedication, drug interactions, new prescriptions
- Metabolic: Hypothyroidism, hyperglycemia/hypoglycemia, hyponatremia, hypercalcemia, B12 deficiency, renal failure
- Malignancy: Occult GI, lung, hematologic (weight loss, anorexia, fatigue) [4]
- Cardiac: Heart failure exacerbation, arrhythmia, orthostatic hypotension
- Elder abuse/neglect: Physical, emotional, financial, or self-neglect [8][17]
- Stroke/TIA: Subtle presentations in elderly (confusion, falls, functional decline without classic focal signs)
- Pain: Undertreated chronic pain limiting mobility
- Substance use: Alcohol use disorder (often underrecognized in elderly)
9. Past Medical History
- Chronic diseases: CHF, COPD, CKD, diabetes, Parkinson's, arthritis — assess for decompensation [2]
- Cognitive diagnoses: Known dementia, MCI, prior delirium episodes
- Psychiatric history: Depression, anxiety, prior suicide attempts
- Surgical history: Recent procedures, hip/knee replacement, prior fractures
- Prior hospitalizations: Frequency, reasons, length of stay
- Baseline functional status: Prior level of independence, use of assistive devices, home services already in place
- Advance directives: Code status, healthcare proxy, goals of care documentation
10. Physical Exam
- Vital signs: Temperature (hypothermia in elderly sepsis), orthostatic BP (drop ≥20/10 mmHg), heart rate, SpO2, weight (compare to prior)
- General: Nutritional status, hygiene, clothing appropriateness, body habitus (BMI <22 in >70 years suggests malnutrition) [5]
- Cognitive screen: Brief cognitive assessment — Mini-Cog, 4AT (for delirium), Montreal Cognitive Assessment
- Mood: PHQ-2 or Geriatric Depression Scale
- Skin: Pressure ulcers (sacrum, heels), bruising pattern (abuse?), turgor, rashes
- MSK/Neuro: Gait assessment, Timed Up and Go test (>12 seconds = increased fall risk), grip strength, focal deficits, peripheral neuropathy [7]
- Focused exam maneuvers:
- Oral cavity (dentition, mucous membranes)
- Abdominal exam (masses, tenderness, distension)
- Cardiopulmonary (murmurs, crackles, JVD, edema)
- Rectal exam if GI symptoms or occult blood concern
11. Lab Studies
- Recommended initial labs: [2]
- CBC with differential
- BMP (electrolytes, glucose, BUN/creatinine)
- TSH
- Urinalysis
- Hepatic function panel
- Additional based on clinical suspicion:
- Vitamin B12, folate
- Calcium, phosphate, magnesium
- ESR/CRP (if infection or malignancy suspected)
- Prealbumin (though not a reliable nutritional marker per current evidence) [5]
- Blood cultures if febrile
- Drug levels (digoxin, phenytoin, lithium) if applicable
- Lactate if sepsis concern
- Toxicology screen if altered mental status
- Note: Serum albumin should not be used as a nutritional marker [5]
12. Imaging
- Chest X-ray: Low threshold — pneumonia, CHF, mass
- CT head without contrast: If new confusion, altered mental status, focal deficits, or fall with head strike
- Additional as indicated:
- CT abdomen/pelvis if abdominal complaints or concern for obstruction/mass
- Hip/pelvis X-ray if fall with pain or inability to ambulate
- Abdominal ultrasound if liver function abnormalities or abdominal mass
- When imaging is unnecessary: Stable chronic functional decline with no acute symptoms, no trauma, and normal exam
13. Special Tests
- Frailty screening: Clinical Frailty Scale (CFS) — score ≥6 indicates moderate-to-severe frailty [14][22]
- Functional assessment tools: ISAR (Identification of Seniors at Risk), TRST (Triage Risk Stratification Tool) [25]
- Cognitive screening: Mini-Cog (3-item recall + clock draw), 4AT (delirium screen), MMSE or MoCA
- Depression screening: PHQ-2/PHQ-9, Geriatric Depression Scale
- Nutritional screening: MNA-SF, GLIM criteria [5]
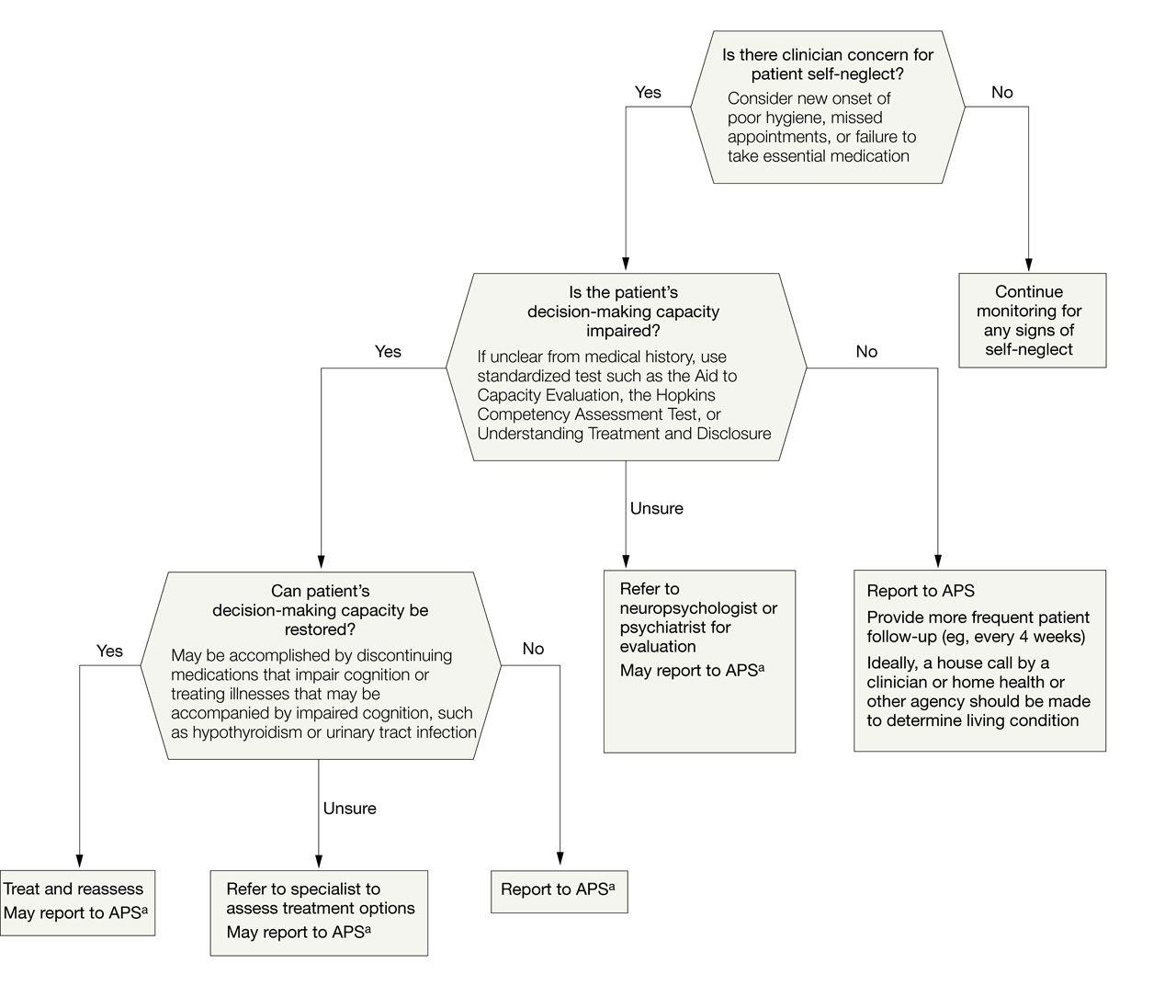
- Capacity assessment: If self-neglect suspected — Aid to Capacity Evaluation, Hopkins Competency Assessment Test [26]
- Fall risk: Timed Up and Go, STEADI algorithm
- Elder abuse screening: ED-MATS (Emergency Department Elder Mistreatment Assessment Tool) [8][27]
- Discharge risk: BRASS (Blaylock Risk Assessment Screen Scale) — identifies patients at risk of difficult discharge [28]
The following figure illustrates a clinical algorithm for approaching suspected elder self-neglect, including capacity assessment and intervention pathways:
14. ECG
- Indications: Syncope, presyncope, falls, altered mental status, chest pain, new medication, palpitations, bradycardia, or tachycardia
- Key findings to assess:
- Bradycardia (medication-related: beta-blockers, calcium channel blockers, digoxin)
- New atrial fibrillation or other arrhythmia
- QTc prolongation (antipsychotics, SSRIs, antiemetics)
- Heart block
- Ischemic changes
- Low threshold for ECG in any elderly patient with unexplained functional decline or fall
15. Assessment
"Failure to cope" is a symptom complex, not a diagnosis. The clinical summary should deconstruct the presentation into its component domains: [3]
- Medical: Identify and treat acute/subacute medical illness (present in ~88% of cases) [1]
- Functional: Quantify ADL/IADL impairments and compare to baseline
- Cognitive: Delirium vs. dementia vs. depression (the "3 Ds")
- Nutritional: Degree of malnutrition, reversible causes
- Social: Support network adequacy, caregiver status, housing, finances
Severity stratification
- Mild: IADL decline only, intact cognition, some social support → likely safe for discharge with services
- Moderate: ADL decline, mild cognitive impairment, limited support → may need observation, intensive discharge planning
- Severe: Multiple ADL dependencies, delirium/dementia, no caregiver, unsafe home → likely requires admission and/or placement
Complications: Prolonged hospitalization itself causes iatrogenic harm in elderly — deconditioning, nosocomial infection, delirium, falls, pressure injuries.
16. Treatment Plan
Initial stabilization (ED)
- Treat identified acute medical conditions (antibiotics for infection, fluids for dehydration, glucose correction, etc.)
- Medication reconciliation — discontinue or reduce FRIDs when possible [29]
- Pain management (prefer acetaminophen <3g/day; avoid new opioids/NSAIDs if possible) [10]
- Nutritional support: oral supplements, address dehydration
- Delirium prevention: reorientation, minimize tethers, avoid unnecessary sedation, correct sensory deficits (glasses, hearing aids)
Targeted interventions
- Depression: Start low-dose SSRI if appropriate; urgent psychiatric referral if suicidal
- Cognitive impairment: Avoid anticholinergics; consider cholinesterase inhibitor referral for outpatient
- Frailty: Exercise/rehabilitation referral — evidence supports multicomponent exercise programs [14]
- Malnutrition: Oral nutritional supplements, dietitian referral, address reversible causes (dental, dysphagia, depression) [5]
- Caregiver support: Assess caregiver burden, provide respite care resources [19]
Social work consultation is critical and should be initiated early — available in ~78% of EDs with SDOH response policies. [24]
17. Disposition
Admission criteria
- Acute medical illness requiring inpatient treatment
- Delirium requiring workup and monitoring
- Unsafe for discharge: no caregiver, unable to perform basic ADLs, unable to ambulate safely [7]
- Concern for elder abuse/neglect requiring safe placement
- Patients with dementia and behavioral disturbance no longer manageable at home [28]
Observation indications
- Borderline cases awaiting social work evaluation, home services setup, or family meeting
- Awaiting capacity assessment
Discharge criteria
- Acute medical issues resolved or stable
- Adequate functional status to return home safely (can ambulate, toilet, feed self or has caregiver)
- Home services arranged (home health, Meals on Wheels, PT/OT)
- Safe home environment confirmed
- Follow-up arranged within 1–2 weeks
Specialist consultation triggers
- Geriatrics: Complex frailty, goals of care, comprehensive geriatric assessment [20][22]
- Psychiatry: Depression with suicidality, psychosis, capacity concerns
- Adult Protective Services: Suspected abuse, neglect, or self-neglect [17]
- Social work: All cases — for resource coordination, discharge planning, community referrals
Postacute care options (when discharge home is not feasible): [19][30]
- Home health (skilled nursing + rehab, requires homebound status)
- Adult day programs
- Assisted living facility
- Skilled nursing facility (SNF)
- Programs of All-Inclusive Care for the Elderly (PACE)
- Area Agencies on Aging for community resources
18. Follow Up / Return Precautions
- Follow-up timing: PCP within 1–2 weeks; geriatrics referral if available; home health within 48 hours of discharge if ordered [31]
- Return precautions (counsel patient and family):
- New confusion, worsening disorientation
- Fever or signs of infection
- Falls or inability to ambulate
- Inability to eat or drink
- Medication side effects (dizziness, excessive sedation)
- Worsening depression or suicidal thoughts
- Patient/family counseling:
- "Failure to cope" often signals a turning point — discuss goals of care and advance directives [2]
- Educate on fall prevention (remove rugs, improve lighting, grab bars)
- Discuss long-term care planning proactively before the next crisis [19]
- Provide written discharge instructions in large font; ensure caregiver understands plan
- Expected course: Depends entirely on underlying etiology — reversible causes (infection, medication, depression) may allow return to baseline; progressive conditions (dementia, advanced frailty) require ongoing care escalation
Relevant ICD-10 Codes
Also code the specific underlying medical diagnosis when identified — avoid using "failure to cope" as a standalone diagnosis, as it leads to diagnostic closure and delays in care. [1]
The following figure from Smulowitz et al. illustrates how functional status, cognition, and social support cumulatively influence the probability of hospital admission from the ED in older adults:
References
1. The Diagnosis "Failure to Thrive" and Its Impact on the Care of Hospitalized Older Adults: A Matched Case-Control Study. — Tsui C, Kim K, Spencer M. BMC Geriatrics. 2020.
2. Geriatric Failure to Thrive. — Robertson RG, Montagnini M. American Family Physician. 2004.
3. "Failure to Thrive" in Older Adults. — Sarkisian CA, Lachs MS. Annals of Internal Medicine. 1996.
4. Unintentional Weight Loss in Older Adults. — Gaddey HL, Holder KK. American Family Physician. 2021.
5. Malnutrition in Older Adults. — Cruz-Jentoft AJ, Volkert D. The New England Journal of Medicine. 2025.
6. Association of Functional Status, Cognition, Social Support, and Geriatric Syndrome With Admission From the Emergency Department. — Smulowitz PB, Weinreb G, McWilliams JM, O'Malley AJ, Landon BE. JAMA Internal Medicine. 2023.
7. Geriatric Emergency Department Guidelines. — Annals of Emergency Medicine. 2014.
8. Best Practices Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Partner Violence. — Christine S. Cocanour MD FACS FCCM, Randall S. Burd MD PhD FACS, James W Davis MD FACS, et al American College of Surgeons (2019). 2019.
9. The Forensic Lens: Bringing Elder Neglect Into Focus in the Emergency Department. — DeLiema M, Homeier DC, Anglin D, Li D, Wilber KH. Annals of Emergency Medicine. 2016.
10. Risk Assessment and Prevention of Falls in Older Community-Dwelling Adults: A Review. — Colón-Emeric CS, McDermott CL, Lee DS, Berry SD. The Journal of the American Medical Association. 2024.
11. Best Practices Guidelines Geriatric Trauma Management. — Alicia Mangram MD FACS, Jessica M. Berdeja MD, Christine S. Cocanour MD FACS FCCM, et al American College of Surgeons (2023). 2023.
12. Falls in Older Adults: Approach and Prevention. — Coulter JS, Randazzo J, Kary EE, Samar H. American Family Physician. 2024.
13. American Geriatrics Society Response to the World Falls Guidelines. — Eckstrom E, Vincenzo JL, Casey CM, et al. Journal of the American Geriatrics Society. 2024.
14. Frailty in Older Adults. — Kim DH, Rockwood K. The New England Journal of Medicine. 2024.
15. Applicability of the GLIM Criteria for the Diagnosis of Malnutrition in Older Adults in the Emergency Ward: A Pilot Validation Study. — Muñoz Fernandez SS, Garcez FB, Alencar JCG, et al. Clinical Nutrition. 2021.
16. Emergency Department Comprehensive Social Risk Screening and Resource Referral Program. — Stillman K, Dahut A, Caudill A, et al. The Western Journal of Emergency Medicine. 2025.
17. Assisting Adult Protective Services in Addressing Maltreatment in Older Adults. — Unwin BK, Stubbs SL, D'Heron H. American Family Physician. 2022.
18. Self-Neglect in Older Adults: A Primer for Clinicians. — Pavlou MP, Lachs MS. Journal of General Internal Medicine. 2008.
19. Care Transition and Long-term Care Options for Older Adults. — Unwin BK, Bedsaul NB, Stubbs S. American Family Physician. 2022.
20. Comprehensive Geriatric Assessment in the Emergency Department. — Ellis G, Marshall T, Ritchie C. Clinical Interventions in Aging. 2014.
21. Factors Associated With Admission to Bed-Based Care: Observational Prospective Cohort Study in a Multidisciplinary Same Day Emergency Care Unit (SDEC). — Elias TCN, Bowen J, Hassanzadeh R, Lasserson DS, Pendlebury ST. BMC Geriatrics. 2021.
22. Implementing an Acute Frailty Service in the Emergency Department: A Mixed-Methods Service Evaluation of Feasibility, Patient Outcomes and Experience. — Zhang Y, Green V, Montagu A. Journal of Evaluation in Clinical Practice. 2026.
23. Evaluating and Treating Unintentional Weight Loss in the Elderly. — Huffman GB. American Family Physician. 2002.
24. Screening and Response for Adverse Social Determinants of Health in US Emergency Departments. — Molina MF, Cash RE, Loo SS, et al. JAMA Network Open. 2025.
25. Functional Assessments Utilised in Emergency Departments: A Systematic Review. — Bissett M, Cusick A, Lannin NA. Age and Ageing. 2013.
26. Elder Abuse and Self-neglect: “I Don't Care Anything About Going to the Doctor, to Be Honest. . . . ”. — Mosqueda L, Dong X. The Journal of the American Medical Association. 2011.
27. Identifying and Initiating Intervention for Elder Abuse and Neglect in the Emergency Department. — Rosen T, Stern ME, Elman A, Mulcare MR. Clinics in Geriatric Medicine. 2018.
28. Prevalence, Determinants and Practical Implications of Inappropriate Hospitalizations in Older Subjects: A Prospective Observational Study. — Isaia G, Brunetti E, Presta R, et al. European Journal of Internal Medicine. 2021.
29. Prevention of Falls in Community-Dwelling Older Adults. — Ganz DA, Latham NK. The New England Journal of Medicine. 2020.
30. Navigating Postacute Care Options for Patients After Hospital Discharge. — Deardorff WJ, Burke RE, Makam AN. JAMA Internal Medicine. 2026.
31. Comprehensive Discharge Planning and Home Follow-up of Hospitalized Elders: A Randomized Clinical Trial. — Naylor MD, Brooten D, Campbell R, et al. The Journal of the American Medical Association. 1999.
32. CMS.gov: R62-Lack of expected normal physiol dev in childhood and adults. — Centers for Medicare & Medicaid Services (CMS) and the National Center for Health Statistics 2024.