Ischemic Colitis
Ischemic colitis (IC) is the most common form of intestinal ischemia, resulting from sudden, often transient reduction in mesenteric blood flow to the colon, predominantly affecting watershed areas…
Ischemic colitis (IC) is the most common form of intestinal ischemia, resulting from sudden, often transient reduction in mesenteric blood flow to the colon, predominantly affecting watershed areas (splenic flexure/Griffith point and rectosigmoid junction/Sudeck point). [1-2] It is the second most common cause of colonic hematochezia, accounting for up to 19% of lower GI bleeding. [2] Median age is 70 years, with a female predominance (F:M ~3.5:1). [1][3] Over 95% of cases are non-occlusive in etiology. [1]
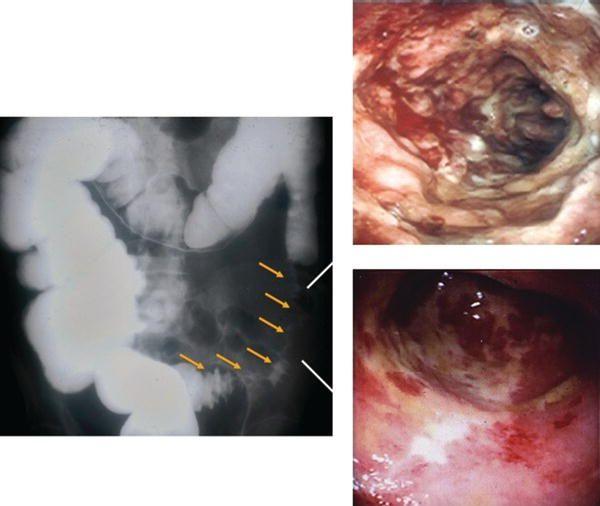
The following figure demonstrates the classic radiographic and endoscopic appearance of ischemic colitis, including thumbprinting on barium enema and the ulcerated, hemorrhagic mucosal pattern on colonoscopy:
1. History
- Classic triad (temporal sequence): Sudden cramping left lower abdominal pain → urgent desire to defecate → passage of bright red/maroon blood or bloody diarrhea within 24 hours of pain onset [5]
- Pain is typically mild-to-moderate and precedes bleeding [5]
- Most common symptoms: abdominal pain (87%), rectal bleeding (84%), diarrhea (56%), nausea (30%) [5]
- Symptom onset is rapid — manifests within hours, unlike IBD or infectious colitis [6]
- Ask about recent hypotensive episodes, dehydration, recent surgery (especially aortic), recent colonoscopy prep, new medications, constipation, illicit drug use (cocaine, methamphetamine)
- Important negative: Isolated right colon ischemia (IRCI) often presents with pain but without rectal bleeding (only 25–46% have hematochezia) — maintain suspicion in patients with acute severe abdominal pain, especially with dialysis, sepsis, or shock [5]
2. Alarm Features
- Peritoneal signs on exam (guarding, rigidity, rebound)
- Hemodynamic instability: hypotension (SBP <90 mmHg), tachycardia (HR >100)
- Abdominal pain without rectal bleeding (suggests IRCI or acute mesenteric ischemia [AMI])
- Isolated right-sided colitis — 48.4% adverse outcome rate vs. 12.1% for non-right-sided; >50% require surgery [2][7]
- Pancolonic involvement — mortality rate ~21% [1]
- Pneumatosis intestinalis or portal venous gas on CT (transmural infarction) [5]
- Gangrene on colonoscopy (blue-black nodules, dusky mucosa) [6]
- Lactic acidosis, rising WBC, worsening pain despite treatment
- Features suggesting AMI: atrial fibrillation + severe pain + IRCI [5]
3. Medications
Contributing medications
- Constipation-inducing drugs (opioids, anticholinergics, calcium channel blockers) — most common precipitant in older adults [1]
- Diuretics, digoxin, NSAIDs [1]
- Vasoconstrictors: triptans (naratriptan, sumatriptan), ergotamines, vasopressors [8]
- IBS drugs: alosetron, tegaserod (highest reported ORs for drug-induced IC) [8]
- Immunomodulators, antipsychotics, oral contraceptives/hormonal therapy [5][9]
- Illicit drugs: cocaine, methamphetamine [5]
- Colonoscopy prep agents (PEG 3350, sodium phosphate/Osmoprep) [1][8]
Treatment medications
- IV fluids for resuscitation
- Broad-spectrum antibiotics for moderate-to-severe disease (e.g., ciprofloxacin + metronidazole or piperacillin-tazobactam) [5]
- No antibiotics needed for mild disease [1][5]
Contraindicated/avoid
- NSAIDs, vasoconstrictors, opioids (worsen ischemia/constipation)
- Glucocorticoids are not recommended for IC (unless treating underlying vasculitis) [5]
- Antithrombotic therapy is not needed in >95% of cases (non-occlusive etiology) [1]
4. Diet
- Acute phase: NPO / bowel rest with IV hydration until symptoms improve [5]
- Advance to clear liquids, then low-residue diet as tolerated
- Long-term: Adequate hydration to prevent dehydration-triggered recurrence; high-fiber diet to prevent constipation [1]
- Avoid excessive caffeine or alcohol that may contribute to dehydration
5. Review of Systems
- GI: Abdominal pain character/location, bloody vs. non-bloody diarrhea, nausea/vomiting, constipation history
- Cardiovascular: Chest pain, palpitations, dyspnea (screen for MI, arrhythmia, CHF)
- Vascular: Claudication, prior DVT/PE (peripheral arterial disease, hypercoagulable state)
- Constitutional: Fever, dizziness, syncope (6% present with syncope) [5]
- Urologic: Decreased urine output (dehydration, shock)
- Neurologic: Altered mental status (sepsis, hypoperfusion)
6. Collateral History and Family History
- Confirm medication list with pharmacy/family — especially recent additions or dose changes of antihypertensives, opioids, or constipation-inducing agents
- Recent procedures: aortic surgery, cardiac catheterization, colonoscopy [1]
- Recent illness with dehydration, hypotension, or prolonged immobility
- Family history: Hypercoagulable disorders (Factor V Leiden, antiphospholipid syndrome) — more relevant in younger patients or those with recurrent IC [1]
- Social history: cocaine/methamphetamine use, smoking, functional status
7. Risk Factors
- Age ≥65 years (3.7× relative risk at age 70–79 vs. 50–59) [1]
- Female sex [1][3]
- Cardiovascular disease: Hypertension, atrial fibrillation, CHF, coronary artery disease [1][10]
- Peripheral arterial disease (OR 4.1) [10]
- Diabetes mellitus (OR 1.76) [10]
- Dyslipidemia (OR 2.12) [10]
- COPD [1][11]
- Chronic kidney disease / dialysis [5]
- Constipation — most common precipitant in elderly [1]
- Polypharmacy — especially constipation-inducing drugs, diuretics, NSAIDs [1]
- Recent surgery: Aortoiliac instrumentation, cardiopulmonary bypass [1]
- Shock/sepsis/hypovolemia [2]
- Hypercoagulable states (younger patients) [1]
8. Differential Diagnosis
- Acute mesenteric ischemia (AMI) — cannot-miss; more severe, involves small bowel, pain out of proportion to exam; CTA required if suspected [5]
- Infectious colitis — C. difficile, E. coli O157:H7, Salmonella, Shigella, CMV; stool studies differentiate [1][6]
- Inflammatory bowel disease (Crohn's, UC) — chronic/relapsing course, younger patients, different distribution; biopsy helps distinguish [6]
- Diverticulitis — typically painless bleeding or LLQ pain with fever; CT differentiates [5]
- Colorectal malignancy — obstructing lesion; colonoscopy with biopsy [1]
- Radiation colitis — history of pelvic radiation
- Drug-induced colitis — NSAIDs, fibrates; histologically milder inflammation than IC [12]
- Distinguishing feature of IC: Abrupt onset (hours), segmental distribution with sharp demarcation, watershed area involvement, rectal sparing [2][6]
9. Past Medical History
- Prior episodes of ischemic colitis (5-year recurrence rate 7–13%) [1]
- Cardiovascular disease history (MI, CHF, atrial fibrillation, PVD)
- Prior aortic or cardiac surgery
- History of hypercoagulable disorders or DVT/PE
- Chronic constipation
- Dialysis dependence
- Prior abdominal surgeries (adhesions, altered anatomy)
10. Physical Exam
- Vitals: Hypotension (SBP <90), tachycardia (HR >100) — both predictors of severity [5][7]
- Abdomen: Mild-to-moderate tenderness over the involved segment (typically LLQ); distension
- Peritoneal signs (guarding, rigidity, rebound) → emergent surgical consultation [5]
- Rectal exam: Gross blood, maroon stool; assess for masses
- Cardiovascular: Irregular rhythm (atrial fibrillation), murmurs, signs of CHF
- Peripheral vascular: Diminished pulses, signs of PVD
- Skin: Mottling, livedo reticularis (vasculitis), signs of dehydration
11. Lab Studies
- CBC: Leukocytosis (WBC >15 × 10⁹/L is a severity marker); anemia (Hgb <12 g/dL) [5]
- BMP: BUN >20 mg/dL (severity marker), sodium <136 mEq/L, creatinine (renal function) [5]
- Lactate: Elevated suggests tissue hypoperfusion/necrosis [13]
- LDH: >350 U/L is a severity marker [5]
- CRP / Procalcitonin: Elevated; may help triage severity [11]
- D-dimer: May predict severity [11]
- Lactic acid: Critical for ruling out bowel necrosis
- Coagulation studies: PT/INR, PTT
- Blood cultures: If sepsis suspected
- Stool studies: C. difficile toxin, stool culture, ova and parasites — to rule out infectious colitis [1]
- Type and screen if significant bleeding
- Thrombophilia workup (antiphospholipid antibody, Factor V Leiden): Consider in younger patients or recurrent IC; generally not needed in elderly [1]
12. Imaging
First-line: CT abdomen/pelvis with IV and oral contrast [5]
- Findings: Segmental bowel wall thickening, thumbprinting, pericolonic fat stranding ± ascites [5]
- These findings are suggestive but not specific — also seen in diverticulitis, IBD, infectious colitis [5]
CT Angiography (CTA): Perform if: [5]
- Isolated right colon ischemia (IRCI) suspected
- AMI cannot be excluded
- Severe presentation
Ominous CT findings
- Pneumatosis intestinalis and portomesenteric venous gas → transmural infarction [5]
- Free intraperitoneal fluid (predictor of need for surgery) [13]
When imaging is unnecessary: Mild, classic left-sided presentation in a stable patient may proceed directly to colonoscopy [5]
Arteriography: Rarely needed; consider if CTA negative but AMI still suspected [5]
13. Special Tests
Colonoscopy (gold standard for diagnosis): [5][14]
- Perform within 48 hours of presentation in absence of peritoneal signs [5]
- Use minimal insufflation, preferably CO₂ [1][5]
- Obtain biopsies unless gangrene is present [5]
- Do NOT perform if peritoneal signs, pneumatosis, or evidence of gangrene on CT [5]
Key endoscopic findings: [5-6]
- Erythema (83.7%), edema (69.9%), friability (42.6%)
- Superficial ulcerations including the colon single-stripe sign (CSSS) — a linear ulcer ≥5 cm along the longitudinal axis of the left colon; indicates milder disease with better prognosis (0% surgery vs. 27% for circumferential disease) [5]
- Deep ulcerations (21.7%), blue-black nodules suggestive of gangrene (5.5%) [5]
- Segmental distribution with abrupt transition between normal and abnormal mucosa [2]
- Rectal sparing (dual blood supply) [2]
Histopathology: Mucosal/submucosal hemorrhage, edema, capillary thrombi, neutrophil infiltration; pathognomonic ghost cells rarely observed [6]
Severity scoring (ACG proposed classification): [5]
- Mild: Typical symptoms, segmental (not right-sided), no risk factors for poor outcome
- Moderate: ≤3 of: male sex, SBP <90, HR >100, pain without bleeding, BUN >20, Hgb <12, LDH >350, Na <136, WBC >15K, mucosal ulceration on colonoscopy
- Severe: >3 of the above OR peritoneal signs, pneumatosis, gangrene, pancolonic/IRCI distribution
14. ECG
- Obtain ECG in all patients to evaluate for:
- Continuous telemetry monitoring for moderate-to-severe disease
15. Assessment
- IC is self-limited in the majority of cases, resolving with supportive care [1][5]
- 15% may develop bowel necrosis or ischemic strictures [1]
- Mortality: Overall 8–10%; rises to 21% with right-sided or pancolonic involvement; surgical mortality ~39% [1-2][5]
- 5-year recurrence rate: 7–13% [1]
- Atypical presentations to recognize: IRCI without bleeding, post-surgical IC (especially after aortic surgery), young patients with drug-induced or hypercoagulable etiologies [1][5]
16. Treatment Plan
Mild disease (majority of patients)
- Bowel rest (NPO), IV fluid resuscitation [5]
- Discontinue offending medications (NSAIDs, vasoconstrictors, constipation-inducing drugs) [1]
- Treat precipitating conditions (dehydration, CHF, arrhythmia)
- Serial abdominal exams, monitor pain/fever/bleeding/WBC [1]
- No antibiotics needed for mild disease [1]
- Advance diet as symptoms improve
Moderate disease
- All of the above PLUS:
- Broad-spectrum antibiotics (e.g., ciprofloxacin + metronidazole, or piperacillin-tazobactam) [5]
- Surgical consultation [5]
- Serial labs (CBC, lactate, BMP)
Severe disease
- Emergent surgical consultation [5]
- Aggressive resuscitation, ICU admission
- Broad-spectrum antibiotics
- Surgery indicated for: peritoneal signs, pneumatosis/portal venous gas, gangrene on colonoscopy, clinical deterioration despite medical management, pancolonic or IRCI with hemodynamic instability [5]
- Surgical options: segmental colectomy, subtotal/total colectomy with diverting stoma [5]
Anticoagulation: Only if mesenteric venous thrombus or thromboembolism identified [1]
17. Disposition
Admit (most patients presenting to ED): [5]
- Hemodynamic instability or need for IV resuscitation
- Moderate or severe disease by ACG criteria
- Inability to tolerate oral intake
- Significant comorbidities (elderly, CHF, CKD, COPD)
- Need for colonoscopy within 48 hours
- Right-sided or pancolonic involvement
ICU admission
Observation/short stay
Discharge (select cases)
- Mild, self-limited symptoms that have resolved
- Tolerating oral intake, stable vitals
- Reliable outpatient follow-up with GI within 1–2 days
Surgical consultation triggers
- Any moderate or severe disease [5]
- Right-sided or pancolonic involvement [2]
- Clinical deterioration despite conservative management [5]
- Persistent symptoms >2–3 weeks or protein-losing colopathy [5]
- Recurrent sepsis after apparent recovery [5]
18. Follow Up / Return Precautions
Follow-up timing
- GI follow-up within 1–2 weeks after discharge for mild disease
- Colonoscopy with biopsy if not performed during admission (to exclude malignancy, IBD, infection) [1]
- Repeat colonoscopy in 1–2 months to assess healing and rule out underlying lesion
Return precautions — instruct patients to return immediately for:
- Worsening or recurrent abdominal pain
- Increased or recurrent bloody stools
- Fever, chills, rigors
- Dizziness, lightheadedness, syncope
- Inability to tolerate oral fluids
Patient counseling
- Avoid dehydration — maintain adequate fluid intake, especially during illness [1]
- Avoid constipation — use stool softeners, adequate fiber [1]
- Avoid overtreatment of hypertension — particularly during acute illness (risk of hypoperfusion) [1]
- Review and minimize unnecessary medications that predispose to IC [1]
- Expected recovery: Most episodes resolve within 1–2 weeks without sequelae [5]
- Recurrence risk: ~7–13% over 5 years; identify and modify individual risk factors (arrhythmia, cardiovascular disease, vasoactive drugs) [1-2]
References
1. Colorectal Cancer Screening and Surveillance and Other Colon Conditions in the Older Adult. — Calderwood AH, Shaukat A. The American Journal of Gastroenterology. 2025.
2. Gastrointestinal Surgical Emergencies Textbook. — Ashley E. Aaron, Andrea Amabile, Ciro Andolfi, et al American College of Surgeons (2021). 2021.
3. Analysis of Clinical Characteristics of 117 Cases of Ischemic Colitis. — Hong SS. BMC Gastroenterology. 2025.
4. Intestinal ischemia and vasculitides. — Juan‐Ramón Malagelada, Carolina Malagelada Yamada's Atlas of Gastroenterology. 2022.
5. ACG Clinical Guideline: Epidemiology, Risk Factors, Patterns of Presentation, Diagnosis, and Management of Colon Ischemia (CI). — Brandt LJ, Feuerstadt P, Longstreth GF, Boley SJ. The American Journal of Gastroenterology. 2015.
6. Differential Diagnosis of Inflammatory Bowel Disease: Imitations and Complications. — Gecse KB, Vermeire S. The Lancet. Gastroenterology & Hepatology. 2018.
7. The Predictors of the Severity of Ischaemic Colitis: A Systematic Review of 2823 Patients From 22 Studies. — Sun D, Wang C, Yang L, Liu M, Chen F. Colorectal Disease : The Official Journal of the Association of Coloproctology of Great Britain and Ireland. 2016.
8. Assessing the Association Between Drug Use and Ischaemic Colitis: A Retrospective Pharmacovigilance Study Using FDA Adverse Event Data. — An J, Wu K, Wu T, et al. BMJ Open. 2025.
9. Ischemic Colitis as a Complication of Medication Use: An Analysis of the Federal Adverse Event Reporting System. — Bielefeldt K. Digestive Diseases and Sciences. 2016.
10. Risk Factors Associated With the Development of Ischemic Colitis. — Cubiella Fernández J, Núñez Calvo L, González Vázquez E, et al. World Journal of Gastroenterology. 2010.
11. Bad Blood: Ischemic Conditions of the Large Bowel. — Rizwan R, Feuerstadt P. Current Opinion in Gastroenterology. 2022.
12. Triggers of Histologically Suspected Drug-Induced Colitis. — Brechmann T, Günther K, Neid M, Schmiegel W, Tannapfel A. World Journal of Gastroenterology. 2019.
13. Ischemic Colitis: Risk Factors for Eventual Surgery. — Paterno F, McGillicuddy EA, Schuster KM, Longo WE. American Journal of Surgery. 2010.
14. Diagnostic Methods and Drug Therapies in Patients With Ischemic Colitis. — Xu Y, Xiong L, Li Y, Jiang X, Xiong Z. International Journal of Colorectal Disease. 2021.