Radial Nerve Injury
The radial nerve (C5–T1, posterior cord of the brachial plexus) is the most commonly injured nerve in peripheral nerve trauma, primarily serving the extensor compartment of the upper limb. [1-3] In…
The radial nerve (C5–T1, posterior cord of the brachial plexus) is the most commonly injured nerve in peripheral nerve trauma, primarily serving the extensor compartment of the upper limb. [1-3] Injury classically presents with wrist drop and finger drop with sensory loss over the posterior forearm and dorsal hand. The most common causes are external compression (40%) and humeral fractures (18%), with the arm (spiral groove) being the most frequent site of injury. [1]
1. History
- Mechanism of injury: trauma (fracture, laceration, gunshot wound), compression (sleeping on arm, "Saturday night palsy," crutch use, tourniquet), or repetitive activity [1-2]
- Onset: hyperacute (within 24 hours) in most traumatic and compressive cases; subacute/chronic in entrapment or tumors [1]
- Symptom characterization: inability to extend wrist/fingers, difficulty gripping objects (paradoxically, grip requires wrist extension), numbness/tingling over dorsal hand [2]
- Timing: sudden onset after waking (compression), immediately post-fracture, or progressive (tumor, entrapment)
- Associated symptoms: pain (more common in radial tunnel syndrome), arm swelling (fracture), preceding alcohol/sedative use (Saturday night palsy) [1]
- Important negatives: neck pain, bilateral symptoms, bowel/bladder dysfunction (to exclude cervical myelopathy/radiculopathy)
2. Alarm Features
- Open fracture with nerve deficit — suggests neurotmesis requiring urgent surgical exploration [4]
- Vascular compromise (absent radial pulse, expanding hematoma) — associated with brachial artery injury in humeral fractures
- Progressive weakness or new-onset deficit after fracture fixation — suggests iatrogenic injury [4-5]
- Bilateral wrist drop — consider lead poisoning, multifocal motor neuropathy, or central lesion [6]
- Associated signs of posterior cord or brachial plexus injury (deltoid weakness) — suggests more proximal lesion [6]
- Wrist drop with constitutional symptoms (weight loss, fever) — consider malignancy or nerve sheath tumor [7]
3. Medications
- Relevant contributors to compressive neuropathy: sedatives, alcohol, opioids, general anesthesia (prolonged positioning) — all increase risk of Saturday night palsy [1]
- Neurotoxic medications that may cause generalized peripheral neuropathy (not specific to radial nerve): chemotherapeutics (vincristine, cisplatin, paclitaxel), amiodarone, metronidazole, isoniazid, statins, nitrofurantoin [8-9]
- Common treatments:
- Contraindicated: injection of neurotoxic substances near the nerve; avoid intramuscular injections in the deltoid region on the affected side (reported cause of iatrogenic radial nerve injury) [11]
4. Diet
- No specific dietary triggers for radial nerve injury
- Alcohol excess is a major risk factor for compressive radial neuropathy (Saturday night palsy) and should be addressed [1]
- Nutritional deficiencies (B12, B6, thiamine) can contribute to generalized neuropathy and impair nerve recovery
- Adequate protein intake supports nerve regeneration
5. Review of Systems
- Neurologic: weakness in other distributions (brachial plexus, cervical radiculopathy), bilateral symptoms, gait abnormalities
- Musculoskeletal: arm/forearm pain, history of fracture, joint instability
- Constitutional: weight loss >10% body weight (identified as a risk factor for radial mononeuropathy), fevers, night sweats [1]
- Vascular: cold hand, color changes (compartment syndrome, vascular injury)
- Rheumatologic: joint swelling (synovitis causing PIN compression) [2]
6. Collateral History and Family History
- Witnesses to mechanism (e.g., position during sleep, duration of compression)
- Alcohol or substance use history (critical for Saturday night palsy) [1]
- Occupational history: repetitive pronation/supination, use of crutches, prolonged arm positioning [12]
- Family history of hereditary neuropathy with liability to pressure palsies (HNPP) — autosomal dominant, predisposes to recurrent compressive neuropathies
- Family history of Charcot-Marie-Tooth disease
7. Risk Factors
- Humeral shaft fracture (especially middle-to-distal third) — 8.5–16% incidence of radial nerve palsy [4][10]
- External compression: prolonged arm positioning during sleep, anesthesia, intoxication [1-2]
- Male sex — male predominance in both traumatic and nontraumatic groups [1]
- Diabetes mellitus — increases susceptibility to compressive neuropathy [1]
- Significant weight loss (>10% body weight in 2–3 months) — loss of protective soft tissue [1]
- Excessive alcohol use [1]
- Repetitive forearm pronation/supination — risk for radial tunnel syndrome [10]
- Arm wrestling — 26–28% incidence of radial nerve palsy with humeral shaft fractures [10]
8. Differential Diagnosis
- C7 radiculopathy: wrist drop with radial deviation weakness, but also involves median-innervated muscles (pronator teres, FCR); triceps reflex diminished; neck pain with dermatomal sensory loss [6]
- Posterior cord brachial plexopathy: involves deltoid (axillary nerve) in addition to radial nerve distribution [6]
- Posterior interosseous nerve (PIN) syndrome: finger drop without wrist drop (ECRL spared); no sensory loss; often caused by lipoma or synovitis [2]
- Lateral epicondylitis (tennis elbow): pain without motor weakness; tenderness at lateral epicondyle rather than distal to radial head [10]
- Multifocal motor neuropathy (MMN): chronic progressive finger/wrist extension weakness; conduction block on NCS; treatable with IVIG [1]
- Neuralgic amyotrophy (Parsonage-Turner syndrome): acute severe shoulder/arm pain followed by weakness; may selectively involve PIN [1]
- Lead poisoning: bilateral wrist drop, abdominal pain, basophilic stippling on blood smear
- Central lesion (stroke, brain tumor): upper motor neuron signs, face/leg involvement
9. Past Medical History
- Prior fractures of the humerus or forearm
- Previous episodes of compressive neuropathy (consider HNPP)
- Diabetes mellitus, hypothyroidism
- Malignancy (nerve sheath tumors, metastatic disease) [7]
- Rheumatologic conditions (rheumatoid arthritis — synovitis causing PIN compression)
- Prior surgeries on the arm (iatrogenic injury during ORIF) [4-5]
- Alcohol use disorder
10. Physical Exam
Vital signs: generally normal unless associated polytrauma
Motor examination (localize the lesion level)
Sensory examination
- Posterior forearm and dorsal hand (main trunk lesion) — absent in pure PIN syndrome [2]
- Dorsal radial hand only (superficial radial nerve/handcuff neuropathy) [2]
Special maneuvers
- Tinel sign over spiral groove or radial tunnel
- Maudsley test (resisted middle finger extension) — positive in radial tunnel syndrome [10]
- Resisted forearm supination — pain in radial tunnel syndrome [10]
- Assess for wrist drop with gravity-eliminated and against-gravity testing (MRC grading)
11. Lab Studies
- Routine labs are generally not required for isolated traumatic radial nerve injury
- If etiology unclear:
- If MMN suspected: anti-GM1 ganglioside antibodies [1]
12. Imaging
- X-ray of humerus: first-line if fracture suspected; evaluate for mid-to-distal shaft fractures [2][4]
- MRI of the arm/forearm: indicated for suspected space-occupying lesion (lipoma, nerve sheath tumor, ganglion cyst), or to exclude mimicking diagnoses [2][10]
- Ultrasound (neuromuscular): increasingly used for point-of-care evaluation of nerve continuity, compression sites, and space-occupying lesions [10]
- MRI of cervical spine: if C7 radiculopathy is in the differential [6]
- Imaging is unnecessary in classic Saturday night palsy with clear compressive history and expected recovery trajectory
13. Special Tests
Electrodiagnostic studies (EDX) — the cornerstone of evaluation:
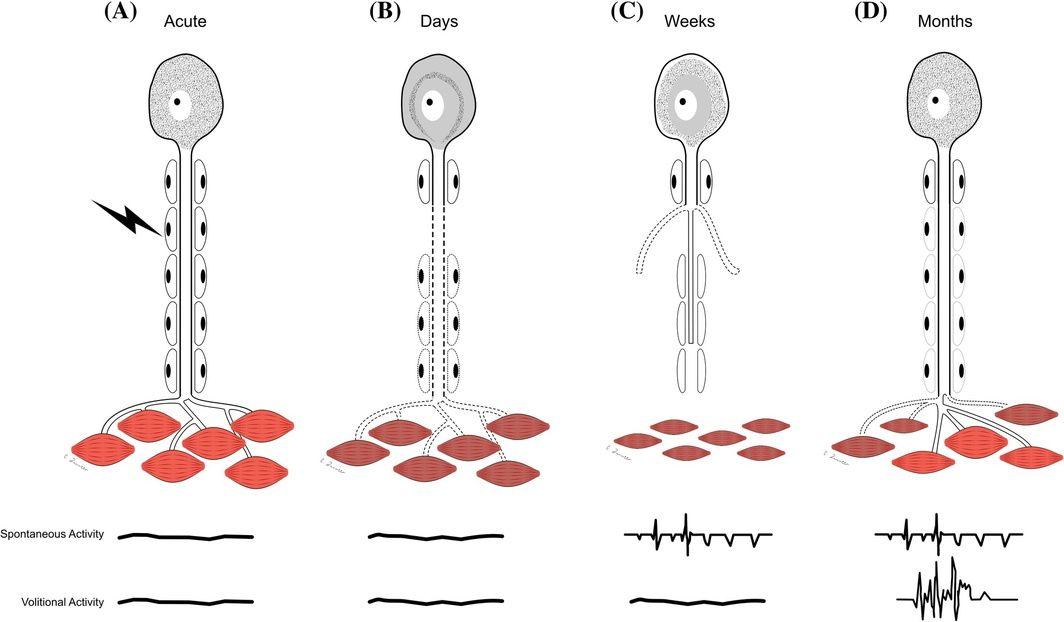
- Optimal timing: at least 3–4 weeks post-injury to allow Wallerian degeneration to manifest; fibrillation potentials and positive sharp waves become evident [13-14]
- Nerve conduction studies (NCS): radial motor NCS recording from both EIP and EDC recommended; assess for conduction block across the spiral groove [1]
- Needle EMG: assess radial-innervated muscles (EIP, EDC, brachioradialis, ECRL, triceps) plus non-radial C7 muscles (pronator teres, FCR) and cervical paraspinals to exclude radiculopathy [1]
- Key prognostic EDX findings: brachioradialis recruitment (full = 100% good outcome); preserved CMAP amplitude; conduction block (favorable, suggests demyelination) [3]
The following figure illustrates the temporal evolution of nerve injury pathophysiology and why EDX has limited utility immediately post-injury:
Nerve injury classification (Seddon/Sunderland): [13][15]
14. ECG
- ECG is not routinely indicated for isolated radial nerve injury
- Consider ECG in the setting of polytrauma, crush injury, or if compartment syndrome is suspected (hyperkalemia from rhabdomyolysis)
- If lead poisoning is suspected as a cause of bilateral wrist drop, ECG may show conduction abnormalities
15. Assessment
Clinical summary: Radial nerve injury most commonly presents as acute wrist and finger drop following humeral fracture or external compression. The arm (spiral groove) is the most common site, accounting for 89% of cases in a large series. [1]
Severity stratification
- Neurapraxia (most compressive injuries): excellent prognosis, recovery within 3 months [13][15]
- Axonotmesis: recovery depends on distance to target muscles; rate of 1 mm/day [15-16]
- Neurotmesis: no spontaneous recovery; requires surgical intervention [13][15]
Typical vs. atypical presentations
- Typical: acute wrist/finger drop after fracture or compression, with sensory loss over dorsal hand
- Atypical: isolated finger drop without wrist drop (PIN syndrome), pure pain without weakness (radial tunnel syndrome), chronic progressive weakness (MMN, tumor) [1-2][10]
Complications: joint contractures from prolonged immobilization, chronic neuropathic pain, permanent motor deficit if surgical window missed
16. Treatment Plan
Initial stabilization
- Immobilize any associated fracture
- Cock-up wrist splint (volar) to maintain wrist in 20–30° extension — prevents contracture and improves grip function [2]
Conservative management (first-line for most cases)
- Avoidance of repeat compression [2]
- Physical/occupational therapy: passive ROM to prevent contractures, progressive strengthening as reinnervation occurs
- NSAIDs for pain; gabapentin/pregabalin for neuropathic pain [9-10]
- For radial tunnel syndrome: activity modification, bracing, corticosteroid injection (diagnostic and therapeutic) [10]
- Saturday night palsy: physical therapy is nearly 100% effective at 6 months [2]
Surgical options (when conservative management fails)
- Neurolysis: for lesions in continuity; 98% achieved motor recovery ≥ Grade 3 [17]
- Primary/secondary nerve repair: 83–91% good outcomes [17]
- Nerve grafting (sural nerve graft): for nerve gaps; optimal timing ≤6.9 months post-injury; shorter defect length and more graft cables predict better outcomes [5][18]
- Nerve transfer (median to radial): median nerve branches (FCR, FDS) coapted to PIN and ECRB; M4+ wrist extension in all patients in one series; optimal within 6 months [11]
- Tendon transfer: considered the gold standard for late or irreversible radial nerve palsy; faster recovery but lacks independent finger function [11]
- Early surgical exploration (within 3 weeks): for humeral fracture-associated palsy, recovery rate of 89.8% vs. 77.2% with nonsurgical management and 68.1% with late exploration [4]
Prognosis by timing (humeral fracture-associated palsy): if nerve has not recovered by 7 months, probability of recovery by 18 months is 56%; if not recovered by 1 year, probability drops to 17% [19]
17. Disposition
Admission criteria
- Associated humeral fracture requiring operative fixation
- Open fracture with nerve deficit (urgent surgical exploration)
- Polytrauma
- Vascular compromise
Discharge criteria
- Isolated compressive radial neuropathy (Saturday night palsy) with no fracture
- Stable neurovascular exam
- Adequate pain control and splinting in place
Observation indications
Specialist consultation triggers
- Orthopedic surgery: humeral fracture management
- Hand/peripheral nerve surgery: open injury with nerve transection, no improvement after 3 months of conservative treatment, progressive deficit [2][13]
- Neurology/electrodiagnostic medicine: EDX at 3–4 weeks for prognostication and localization [14]
- Neurosurgery: complex nerve reconstruction, nerve transfer consideration [11][17]
18. Follow Up / Return Precautions
Follow-up timing
- Clinical reassessment at 2–4 weeks for early signs of recovery (Tinel sign advancement)
- EDX at 3–4 weeks post-injury (optimal timing for diagnostic accuracy) [14]
- Repeat clinical and/or EDX assessment at 3 months — if no recovery from suspected neurapraxia, escalate to surgical consultation [13]
- For axonotmetic injuries: serial assessments every 4–6 weeks monitoring for advancing Tinel sign and clinical reinnervation
Symptoms requiring immediate reassessment
- Worsening weakness or new sensory loss
- Increasing pain, swelling, or signs of compartment syndrome
- New deficit after fracture fixation (iatrogenic injury)
- Development of weakness in other nerve distributions
Patient counseling points
- Wear the wrist splint consistently to prevent contractures and maintain hand function
- Avoid positions that compress the arm (do not sleep with arm draped over chair)
- Avoid alcohol excess
- Recovery timeline: neurapraxia typically resolves within 3 months; axonotmesis recovery occurs at ~1 mm/day from the injury site [13][15]
- Most nontraumatic compressive radial neuropathies (~90%) have a good outcome [3]
Expected recovery course: spontaneous recovery occurs in 77–90% of humeral fracture-associated palsies. [4][19] Compressive (Saturday night palsy) injuries have the best prognosis, with demyelinating pathophysiology and expected full recovery. [1][13]
References
1. Radial Mononeuropathy: Clinical and Electrodiagnostic Characteristics in 177 Patients. — Sinthuwong C, Katirji B. Muscle & Nerve. 2026.
2. Peripheral Nerve Entrapment and Injury in the Upper Extremity. — Silver S, Ledford CC, Vogel KJ, Arnold JJ. American Family Physician. 2021.
3. How electrodiagnosis predicts clinical outcome of focal peripheral nerve lesions. — Robinson LR. Muscle & Nerve. 2015.
4. Radial Nerve Palsy Recovery With Fractures of the Humerus: An Updated Systematic Review. — Ilyas AM, Mangan JJ, Graham J. The Journal of the American Academy of Orthopaedic Surgeons. 2020.
5. Management of Radial Nerve Lesions After Trauma or Iatrogenic Nerve Injury: Autologous Grafts and Neurolysis. — Schwaiger K, Abed S, Russe E, et al. Journal of Clinical Medicine. 2020.
6. Distinguishing Radiculopathies From Mononeuropathies. — Robblee J, Katzberg H. Frontiers in Neurology. 2016.
7. Clinical Reasoning: A 65-Year-Old Woman With Cancer History and Wrist Drop. — Merrill R, Puckett M, Morrow WP, et al. Neurology. 2022.
8. Peripheral Neuropathy: Evaluation and Differential Diagnosis. — Castelli G, Desai KM, Cantone RE. American Family Physician. 2020.
9. Peripheral Neuropathy. — Mauermann ML, Staff NP. The Journal of the American Medical Association. 2026.
10. Sports‐related peripheral nerve injuries of the upper limb. — Dutton RA, Norbury J, Colorado B. Muscle & Nerve. 2024.
11. Median to Radial Nerve Transfer: An 8-Year Experience From a Lower-Middle Income Country. — Ahmed KS, Rajput BU, Siddiqui MAI, Nadeem A, Rahman MF. The Journal of Surgical Research. 2023.
12. Occupational nerve injuries. — Hearn SL, Jorgensen SP, Gabet JM, Carter GT. Muscle & Nerve. 2025.
13. Assessment, management, and rehabilitation of traumatic peripheral nerve injuries for non‐surgeons. — Bateman EA, Pripotnev S, Larocerie-Salgado J, Ross DC, Miller TA. Muscle & Nerve. 2025.
14. Optimal timing of needle electromyography to diagnose lesion severity in traumatic radial nerve injury. — Steenbeek ED, Pondaag W, Tannemaat MR, et al. Muscle & Nerve. 2023.
15. Traumatic injury to peripheral nerves. — Robinson LR. Muscle & Nerve. 2022.
16. Peripheral Nerve Reconstruction after Injury: A Review of Clinical and Experimental Therapies. — Grinsell D, Keating CP. BioMed Research International. 2014.
17. Surgical Management and Outcome in Patients With Radial Nerve Lesions. — Kim DH, Kam AC, Chandika P, Tiel RL, Kline DG. Journal of Neurosurgery. 2001.
18. Rehabilitation Outcomes and Prognostic Factors of Nerve Grafting Combined With Exercise Therapy for High-Level Radial Nerve Injury: Results of a Retrospective Study. — Cen Y, Zhao H, Wu L. Injury. 2025.
19. What Is the Probability of Radial Nerve Recovery After Surgical Repair of Humerus Fractures Accounting for Time Since Injury?. — Krijnen NA, Comerci AJ, Head LK, et al. Clinical Orthopaedics and Related Research. 2026.