Scurvy
Scurvy is a multisystem disease caused by ascorbic acid (vitamin C) deficiency, resulting from defective collagen synthesis. It remains underdiagnosed in developed countries, frequently mimicking a…
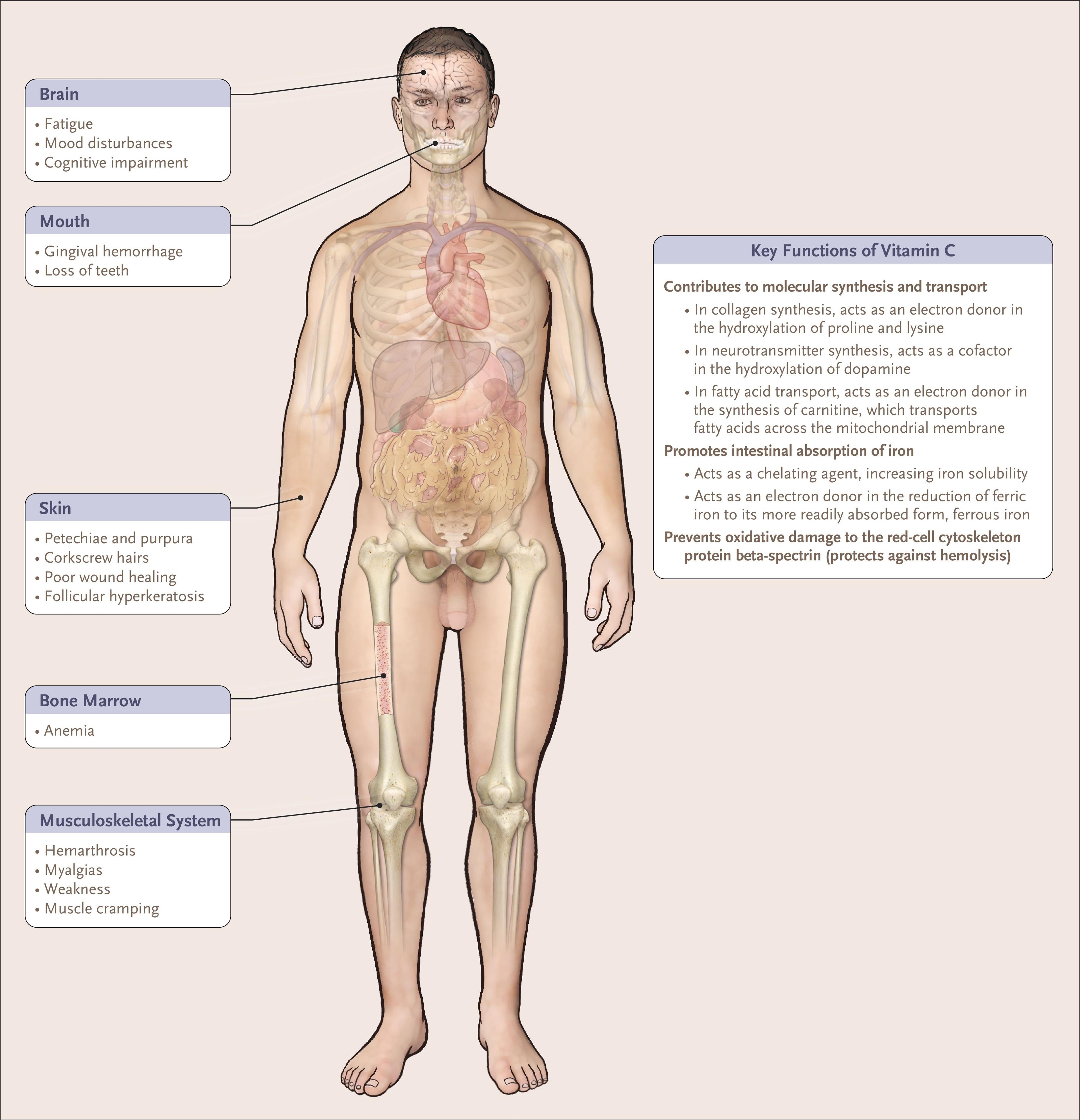
Scurvy is a multisystem disease caused by ascorbic acid (vitamin C) deficiency, resulting from defective collagen synthesis. It remains underdiagnosed in developed countries, frequently mimicking autoimmune, hematologic, and rheumatologic disorders, leading to diagnostic delays and unnecessary invasive workups.[1-2] The following figure illustrates the multisystem consequences of vitamin C deficiency:
View full figure Figure 1. Consequences of Vitamin C Deficiency. Inadequate Support. N Engl J Med. September 1, 2021.
1. History
- Dietary history is the single most important diagnostic clue — ask specifically about fruit and vegetable intake, duration of restricted diet, and food preferences[1-2][4]
- Symptom onset typically occurs after 1–3 months of deficient intake; fatigue is the earliest symptom[2][5]
- Characterize: easy bruising, bleeding gums, joint/bone pain, limb weakness, rash, poor wound healing
- Progression: fatigue → skin findings → musculoskeletal pain → hemorrhagic complications → syncope → sudden death[2][6]
- Associated symptoms: depression, irritability, myalgia, arthralgia, leg edema, hematuria[4][7]
- Important negatives: no trauma history to explain bruising, no anticoagulant use, no family history of bleeding disorders
2. Alarm Features
- Syncope or presyncope — may indicate hemodynamic instability from hemorrhage or autonomic dysfunction[2][6][8]
- Sudden death — reported in severe untreated cases[2]
- Heart failure — severe anemia can lead to high-output cardiac failure[9-10]
- Hemarthrosis, large spontaneous hematomas, or GI bleeding[7][11]
- Transfusion-dependent anemia[12]
- Coagulopathy with active hemorrhage[13]
- Refusal to walk or pseudoparalysis (especially in children) — suggests subperiosteal hemorrhage[14]
3. Medications
Contributors to vitamin C deficiency
- Proton pump inhibitors — noted in 54% of adult scurvy patients in one cohort, likely via impaired absorption[15]
- Oral contraceptives — may interfere with ascorbic acid metabolism[16]
- Dihydropyridine calcium channel blockers (nifedipine, nicardipine) — inhibit intestinal ascorbic acid accumulation in vitro[17]
- Cholestyramine — may impair vitamin absorption[16]
Drug interactions with ascorbic acid treatment
- May decrease efficacy of erythromycin, doxycycline, kanamycin, streptomycin, lincomycin; inactivates bleomycin in vitro[18]
- Acidifies urine → decreases amphetamine and fluphenazine levels[18]
- Warfarin: continue standard INR monitoring (no clinically significant interaction at therapeutic doses)[18]
- G6PD deficiency: IV vitamin C can cause hemolysis — dose reduction required[18-19]
Treatment
- Oral: 100 mg TID or 500 mg daily until resolution (~1 month)[5]
- IV (Ascor): Adults ≥11 years: 200 mg IV daily; children 1–10 years: 100 mg IV daily; infants 5–11 months: 50 mg IV daily. Maximum duration 7 days[18]
4. Diet
- Root cause is inadequate fruit and vegetable consumption[2]
- Dietary triggers for deficiency: "tea and toast" diets, processed food–only diets, ketogenic diets, self-restricted diets, heated/boiled milk (destroys vitamin C)[12][20]
- Acute management: vitamin C supplementation + dietary counseling
- Long-term: ensure daily intake of vitamin C–rich foods (citrus fruits, bell peppers, strawberries, broccoli, tomatoes)
- RDA: 90 mg/day for men, 75 mg/day for women; smokers require an additional 35 mg/day[19][21]
- Hydration: adequate fluid intake; avoid excessive doses (>1 g/day) in patients with renal insufficiency or hyperoxaluria risk[19]
5. Review of Systems
- Skin: rash, bruising, poor wound healing, dry skin, hair changes
- Oral: gum bleeding, swelling, tooth loosening (only in dentate patients)[2]
- MSK: joint pain, bone pain, limping, refusal to bear weight, muscle weakness[7][14]
- Heme: fatigue, pallor, dyspnea on exertion (anemia)
- GI: abdominal pain, GI bleeding, diarrhea[11]
- Neuro/Psych: depression, irritability, cognitive impairment[3]
- Cardiovascular: syncope, presyncope, exertional dyspnea[2][6]
6. Collateral History and Family History
- Social determinants are critical: poverty, homelessness, social isolation, food insecurity[1]
- Collateral from caregivers/family regarding actual dietary intake (patients may underreport restrictions)
- Psychiatric history: depression, eating disorders, autism spectrum disorder, developmental delay — all associated with restrictive diets[2][4][22]
- Alcohol use history — alcoholism is a classic risk factor[2][7]
- Family history of bleeding disorders (to rule out inherited coagulopathies)
- In children: assess developmental status, food preferences, and caregiver feeding practices[4]
7. Risk Factors
- Alcoholism — most common classic risk factor in adults[2][7]
- Social isolation and poverty — major contributors in 21st-century cases[1]
- Psychiatric disorders (depression, anxiety, eating disorders, OCD)[2][23]
- Developmental/behavioral disorders in children (autism, sensory processing issues)[4][22]
- Restrictive or fad diets (ketogenic, self-diagnosed food allergies)[12][23]
- Malabsorptive conditions: Crohn's disease, celiac disease, post-bariatric surgery[5-6][23]
- Elderly with limited mobility or cognitive decline[2]
- Chronic illness with poor nutritional status
- Smoking (increases vitamin C requirements)[21]
- PPI use[15]
8. Differential Diagnosis
- Scurvy is a notorious diagnostic mimicker.[1] Key differentials include:
- Vasculitis (IgA vasculitis/HSP, leukocytoclastic vasculitis) — palpable purpura, but typically with systemic inflammation; biopsy distinguishes
- Bleeding/coagulation disorders (hemophilia, von Willebrand disease, ITP, DIC) — coagulation studies and platelet counts help differentiate; scurvy typically has normal PT/PTT[7]
- Child abuse/non-accidental injury — in pediatric cases with unexplained bruising and fractures; dietary history is key[4]
- Leukemia/malignancy — bone pain, bruising, anemia overlap; peripheral smear and bone marrow biopsy distinguish
- Rheumatologic conditions (rheumatoid arthritis, reactive arthritis) — joint pain and elevated inflammatory markers overlap[1][7]
- Other nutritional deficiencies (rickets/vitamin D deficiency, pellagra) — may coexist[20]
- Hemarthrosis from other causes — hemophilia workup typically negative in scurvy[7]
9. Past Medical History
- Prior episodes of similar symptoms (scurvy can relapse if dietary habits are not corrected)[24]
- GI surgery (bariatric surgery, bowel resections) — impairs absorption[5]
- Inflammatory bowel disease (Crohn's, celiac)[6][23]
- Psychiatric diagnoses affecting eating behavior[2]
- Chronic kidney disease or dialysis (altered vitamin C metabolism)[19]
- History of iron deficiency anemia (54% comorbidity in one cohort)[15]
- Epilepsy on ketogenic diet[12]
10. Physical Exam
Pathognomonic findings
- Perifollicular hemorrhages (petechiae surrounding hair follicles, especially on legs/buttocks)[2][9]
- Corkscrew/coiled hairs[2][6]
- Follicular hyperkeratosis[2]
Other key findings
- Gingival hypertrophy, purplish discoloration, and hemorrhage (only in dentate patients)[2][25]
- Ecchymoses (often out of proportion to any reported trauma)[2]
- Leg edema[2]
- Poor wound healing, wound dehiscence[2]
- Xerosis (dry skin)[2]
- Joint swelling/effusion (hemarthrosis)[7]
- In children: limping, refusal to bear weight, pseudoparalysis, Gower sign[14]
- Vital signs: Tachycardia (anemia), hypotension (hemorrhage/autonomic dysfunction), hypertension (rarely reported)[22]
11. Lab Studies
- Serum ascorbic acid level (plasma vitamin C): <11 µmol/L (<0.2 mg/dL) confirms deficiency; often undetectable in symptomatic patients[4][12][26]
- CBC: anemia (present in up to 80% of cases, often iron deficiency), occasional leukopenia[2][9]
- Iron studies: frequently shows concomitant iron deficiency (vitamin C enhances iron absorption)[15][19]
- Inflammatory markers: ESR and CRP may be elevated — can mislead toward autoimmune/infectious workup[7][12]
- Coagulation studies (PT/PTT): typically normal; helps rule out coagulopathies[7]
- Peripheral blood smear: to exclude hematologic malignancy
- BMP/CMP: assess renal function before high-dose supplementation (oxalate risk)[19]
- Consider checking other nutritional deficiencies (folate, B12, vitamin D, iron) as they frequently coexist[13][20]
12. Imaging
First-line
- X-rays of long bones (especially in children): classic findings include Fränkel lines (dense zone of provisional calcification), Trümmerfeld zone (lucent zone beneath Fränkel line), Pelkan spurs (lateral metaphyseal beaking), Wimberger ring sign, ground-glass osteopenia, subperiosteal hemorrhage[14][20]
Advanced imaging
- MRI: multifocal bone marrow signal abnormalities, physeal irregularities, hemarthrosis, muscular signal abnormalities, subperiosteal hemorrhage[7][12]
- MRI findings can mimic malignancy or osteomyelitis — clinical correlation with dietary history is essential
When imaging is unnecessary
- In adults with classic cutaneous findings and confirmatory dietary history, imaging is generally not needed; diagnosis is clinical + serum vitamin C level[9]
13. Special Tests
- Serum vitamin C level is the confirmatory test (plasma <11 µmol/L = deficiency)[26]
- Buffy-coat leukocyte ascorbic acid level is more accurate but less widely available[22]
- Skin biopsy: may show perifollicular hemorrhage and perivascular inflammation; useful when vasculitis is in the differential
- Platelet aggregation studies: defects reported in some cases[7]
- Therapeutic trial: rapid clinical improvement with vitamin C supplementation is the most cost-effective confirmation of diagnosis[9]
14. ECG
- No specific ECG findings are pathognomonic for scurvy
- ECG indicated if: syncope, presyncope, tachycardia, or suspected cardiac involvement
- Severe anemia may produce sinus tachycardia, nonspecific ST-T wave changes
- Prolonged QTc has been described in nutritional cardiomyopathies broadly[27]
- Autonomic dysfunction from impaired catecholamine synthesis (vitamin C is a cofactor for dopamine → norepinephrine conversion) may contribute to hemodynamic instability[8]
15. Assessment
Scurvy is a clinical diagnosis supported by dietary history, physical exam findings, and confirmed by low serum vitamin C levels. It is frequently misdiagnosed as vasculitis, bleeding disorder, or rheumatologic disease, leading to extensive unnecessary workups.[1] A systematic review of 280 adult cases in the 21st century found that social determinants of health (poverty, isolation, restrictive diets) played a critical role in nearly all cases.[1]
Severity stratification
- Mild: fatigue, myalgia, follicular hyperkeratosis only
- Moderate: purpura, gingival bleeding, arthralgias, anemia
- Severe: hemarthrosis, large hematomas, GI bleeding, syncope, heart failure, coagulopathy[2][10][13]
- Complications: Transfusion-dependent anemia, high-output heart failure, wound dehiscence, secondary infections, sudden death[2][9][12]
16. Treatment Plan
Initial stabilization (ED)
- If hemodynamically unstable: IV fluids, transfuse PRBCs for severe anemia, FFP if coagulopathy with active bleeding[13]
- Begin vitamin C immediately — do not wait for confirmatory levels
Vitamin C supplementation
- Oral (preferred): 250–1000 mg daily in divided doses (commonly 100 mg TID or 500 mg daily) until symptoms resolve, typically 1–4 weeks[5][15]
- IV (Ascor) — when oral is not possible or malabsorption suspected: Adults 200 mg IV daily, max 7 days[18]
- Caution in G6PD deficiency: risk of hemolysis with IV vitamin C; do not exceed RDA[18-19]
- Caution in renal disease: limit to <200 mg/day in dialysis patients (oxalate risk)[19]
Adjunctive
- Correct concomitant deficiencies (iron, folate, vitamin D)[13][15]
- Dietary counseling and social work referral for food insecurity[1]
- In malabsorptive conditions (Crohn's, post-bariatric): may require long-term IV supplementation[26]
- Expected response: Dramatic improvement within days for fatigue, pain, and bleeding; skin findings improve within 1–2 weeks; bone changes resolve over weeks to months[2][9][12]
17. Disposition
Admission criteria
- Hemodynamic instability, active hemorrhage, or need for transfusion[13]
- Severe anemia with cardiac symptoms (heart failure, syncope)[10]
- Inability to tolerate oral intake / need for IV supplementation
- Concern for concomitant serious pathology not yet excluded
Discharge criteria
- Hemodynamically stable, tolerating oral vitamin C, adequate dietary plan in place
- Mild-to-moderate presentations can be managed entirely outpatient
Observation
- Moderate cases with anemia or significant bleeding may warrant brief observation to ensure response to supplementation
Specialist consultation triggers
- Hematology: if bleeding disorder not fully excluded
- Rheumatology: if vasculitis remains in the differential
- GI: if malabsorption suspected (Crohn's, celiac, post-surgical)
- Social work/nutrition: for all patients — address root cause[1]
18. Follow Up / Return Precautions
- Follow-up in 1–2 weeks to reassess symptoms and repeat CBC
- Recheck serum vitamin C at 4 weeks to confirm repletion
- Return precautions: worsening bruising or bleeding, new joint swelling, syncope, chest pain, shortness of breath, inability to eat or drink
- Counsel on lifelong dietary adequacy — scurvy recurs if dietary habits are not sustained[24]
- Expected recovery: fatigue and pain improve within days; skin findings within 1–2 weeks; bone changes over months[2][12]
- In children: reassess growth, development, and dietary habits at follow-up well-child visits[4]
- Address underlying social determinants — connect with community resources, food assistance programs[1]
References
1. Scurvy, an Enduring Mimicker and Diagnostic Dilemma in Adults: A Review of the 280 Relevant Published Cases in the Twenty-First Century. — Rivière E, Mathé A, Blaison F, et al. Clinical Nutrition. 2026.
2. Adult Scurvy. — Hirschmann JV, Raugi GJ. Journal of the American Academy of Dermatology. 1999.
3. Inadequate Support. — Pichan C, Dhaliwal G, Cusick A, Saint S, Houchens N. The New England Journal of Medicine. 2021.
4. Scurvy Due to Selective Diet in a Seemingly Healthy 4-Year-Old Boy. — Nastro A, Rosenwasser N, Daniels SP, et al. Pediatrics. 2019.
5. Review article: the nutritional and pharmacological consequences of obesity surgery. — Stein J, Stier C, Raab H, Weiner R. Alimentary Pharmacology & Therapeutics. 2014.
6. Curious Case of Severe Scurvy. — Henley S, Johnson L, Strickley J. Nutrition in Clinical Practice : Official Publication of the American Society for Parenteral and Enteral Nutrition. 2025.
7. Lost at Sea in Search of a Diagnosis: A Case of Unexplained Bleeding. — Amos LE, Carpenter SL, Hoeltzel MF. Pediatric Blood & Cancer. 2016.
8. Autonomic Reflexes and Vascular Reactivity in Experimental Scurvy in Man. — Abboud FM, Hood J, Hodges RE, Mayer HE. The Journal of Clinical Investigation. 1970.
9. Scurvy in a 10‐Year‐Old Boy. — Cole JA, Warthan MM, Hirano SA, Gowen CW, Williams JV. Pediatric Dermatology. 2010.
10. Severe Scurvy: An Underestimated Disease. — Levavasseur M, Becquart C, Pape E, et al. European Journal of Clinical Nutrition. 2015.
11. Scurvy: Rediscovering a Forgotten Disease. — Gandhi M, Elfeky O, Ertugrul H, Chela HK, Daglilar E. Diseases. 2023.
12. No Longer a Historical Ailment: Two Cases of Childhood Scurvy With Recommendations for Bone Health Providers. — Alten ED, Chaturvedi A, Cullimore M, et al. Osteoporosis International : A Journal Established as Result of Cooperation Between the European Foundation for Osteoporosis and the National Osteoporosis Foundation of the USA. 2020.
13. Recurrent Subcutaneous Hemorrhage and Leg Weakness: A Case of Scurvy Presenting as Simple Purpura. — Miyaguchi K, Urushidani S. The American Journal of Emergency Medicine. 2026.
14. Teaching Video NeuroImage: Scurvy Presenting as Proximal Myopathy in a Young Boy. — Garg M. Neurology. 2022.
15. Scurvy, an Old Story in a New Time: The Hematologist's Experience. — Khalife R, Grieco A, Khamisa K, et al. Blood Cells, Molecules & Diseases. 2019.
16. Drug-Nutrient Interaction. — Matsui MS, Rozovski SJ. Clinical Therapeutics. 1982.
17. Dihydropyridine Calcium Channel Blockers Inhibit Ascorbic Acid Accumulation in Human Intestinal Caco-2 Cells. — Kuo SM, Lin CP, Morehouse HF. Life Sciences. 2001.
18. FDA Drug Label. — Updated date: 2025-11-19. Food and Drug Administration.
19. Criteria and Recommendations for Vitamin C Intake. — Levine M, Rumsey SC, Daruwala R, Park JB, Wang Y. The Journal of the American Medical Association. 1999.
20. Case Report: Uncommon Cause of Limp in the 21 Century. — Thiemann S, Cimorelli V, Bajwa NM. Frontiers in Endocrinology. 2022.
21. Are the UK's Vitamin C Recommendations Evidence-Based? A Critical Comment. — Hemilä H, Chalker E. The British Journal of Nutrition. 2025.
22. An Orange a Day Keeps the Doctor Away: Scurvy in the Year 2000. — Weinstein M, Babyn P, Zlotkin S. Pediatrics. 2001.
23. Scurvy: A Disease Not to Be Forgotten. — Montalto M, Porceddu E, Pero E, et al. Nutrition in Clinical Practice : Official Publication of the American Society for Parenteral and Enteral Nutrition. 2021.
24. Nonalimental Scurvy With Relapse Symptoms After Stopping Oral Vitamin C Supplementation. — Vaezipour N, Leibundgut K. Pediatrics. 2018.
25. Difficult to Think About but Easy to Treat: Scurvy. — Küçükçongar Yavaş A, Engin Erdal A, Çıtak Kurt AN, et al. Journal of Pediatric Endocrinology & Metabolism : JPEM. 2023.
26. High-Dose Vitamin C Therapy for Symptomatic Deficiency in a Patient With Myasthenia Gravis and Crohn's Disease. — Murphree J, Mulherin DW, Morton C, Adams D. Nutrition in Clinical Practice : Official Publication of the American Society for Parenteral and Enteral Nutrition. 2022.
27. Nutritional Heart Disease And Cardiomyopathies: JACC Focus Seminar 4/4. — Sliwa K, Viljoen CA, Hasan B, Ntusi NAB. Journal of the American College of Cardiology. 2022.