Sea Urchin Injury
Sea urchin injuries result from penetration of calcareous spines (94% calcium carbonate) into the skin, most commonly affecting the hands and feet. Over 700 species exist, with approximately 80 con…
Sea urchin injuries result from penetration of calcareous spines (94% calcium carbonate) into the skin, most commonly affecting the hands and feet. Over 700 species exist, with approximately 80 containing substances toxic to humans.[1] The cornerstone of acute management is hot water immersion (~45°C for 30–90 minutes) to neutralize thermolabile venom components, followed by wound exploration, spine removal when accessible, and tetanus prophylaxis.[2-3]
1. History
- Mechanism: stepping on, handling, or brushing against a sea urchin — typically accidental during diving, snorkeling, swimming, or fishing[1]
- Location and water type (saltwater vs. brackish) — affects antibiotic selection[3]
- Number of puncture sites — systemic symptoms more likely with >15–20 spine penetrations[2]
- Timing of injury relative to presentation (acute vs. delayed granulomatous reaction, latency 1–6 months)[1]
- Severity and character of pain — intense burning pain within minutes, often out of proportion to wound size due to toxin release from hollow spines[1]
- Prior marine injuries or known allergies
- Tetanus immunization status
- Any field treatment already administered (hot water soak, attempted spine removal)
2. Alarm Features
- Systemic envenomation (>15–20 spines): paresthesias, muscular paralysis, hypotension, respiratory distress[2]
- Spine penetration into a joint (risk of severe synovitis)[2][4]
- Spine embedded near nerves or tendons (risk of neuropathy)[5]
- Deep penetration into hand, foot, or fascial compartments[2]
- Abdominal or thoracic wall penetration (requires OR exploration)[2]
- Signs of Vibrio or other marine wound infection — rapidly progressive cellulitis, necrotizing fasciitis, especially in immunocompromised patients or those with liver disease[2]
- Anaphylaxis (rare)
3. Medications
Pain control
- Hot water immersion is first-line analgesic[2][6]
- Local infiltration with 1–2% lidocaine without epinephrine for small wounds[2]
- Regional nerve block with 0.5% bupivacaine for larger areas[2]
- Opioid analgesics if refractory[2]
- Antibiotics (not routine for minor wounds in immunocompetent hosts):[2]
- Prophylaxis indicated for: deep punctures, joint involvement, retained foreign bodies, immunosuppressed patients, liver disease[2]
- Saltwater wounds: doxycycline + ceftazidime, or a fluoroquinolone (ciprofloxacin, levofloxacin)[3]
- Penicillin, ampicillin, erythromycin, and first-generation cephalosporins are not acceptable alternatives for marine infections[2]
- Tetanus prophylaxis — update as indicated[5][7]
- Not recommended: topical/systemic steroids or antihistamines acutely, cryotherapy, tight constriction bands, folk remedies (meat tenderizer, papaya)[2]
- Delayed granulomatous reactions: intralesional corticosteroids may be effective[8]
4. Diet
- No specific dietary triggers or restrictions
- Ensure adequate hydration, particularly if prolonged hot water immersion is performed
- No acute or long-term dietary management required
5. Review of Systems
- Neurologic: paresthesias, weakness, numbness distal to injury site
- Musculoskeletal: joint swelling, decreased range of motion (synovitis from intra-articular spine)
- Cardiovascular: hypotension, syncope (systemic envenomation)
- Respiratory: dyspnea (rare, severe envenomation)
- Dermatologic: delayed nodule or papule formation weeks to months later (granuloma)
- Constitutional: fever, chills (suggests secondary infection)
6. Collateral History and Family History
- Travel history — geographic location of injury (tropical/subtropical waters carry higher risk for venomous species)[7]
- Occupation — fishermen, dive instructors at higher risk for recurrent exposure
- Immunosuppression status, liver disease (elevated risk for fulminant Vibrio infection)[2]
- Family history is generally not contributory
- Witnesses may help identify the species involved
7. Risk Factors
- Recreational diving, snorkeling, wading in shallow rocky/coral areas[1]
- Walking barefoot on reef or rocky ocean floor
- Handling sea urchins
- Tropical and subtropical coastal environments
- Immunosuppression or chronic liver disease — dramatically increases risk of life-threatening Vibrio infection[2]
- Elevated serum iron levels (iron is a nutrient for Vibrio species)[2]
8. Differential Diagnosis
- Stingray envenomation — larger laceration, barb may be retained, similar hot water treatment
- Scorpionfish/lionfish/stonefish sting — puncture wound with severe pain, similar venom mechanism
- Coral cut — abrasion/laceration pattern rather than puncture
- Jellyfish/fire coral sting — dermatitis pattern (urticaria, vesicles) rather than puncture
- Marine bacterial cellulitis (Vibrio, Mycobacterium marinum) — may present days to weeks later
- Foreign body reaction from non-biologic material (glass, shell fragment)
- Gout or septic arthritis — if presenting with delayed monoarticular joint swelling[4]
- Purple discoloration from spine dye may be mistaken for retained spine fragment[2]
9. Past Medical History
- Prior sea urchin or marine injuries
- Immunocompromised state (HIV, transplant, chemotherapy)
- Chronic liver disease — critical to identify due to Vibrio risk[2]
- Diabetes or peripheral vascular disease (impaired wound healing)
- Tetanus vaccination history
- History of keloid or granuloma formation
10. Physical Exam
- Vital signs: assess for hypotension, tachycardia (systemic envenomation)
- Wound inspection: number and depth of puncture sites, erythema, edema
- Purple/blue-black discoloration at puncture site — may be dye from spine, not necessarily a retained fragment[2]
- Palpation for retained spines (firm, tender subcutaneous nodules)
- Joint exam: effusion, decreased ROM if intra-articular penetration[4]
- Neurovascular exam distal to injury — assess for neuropathy[5]
- Tendon function testing if hand/foot involvement
- Assess for fusiform swelling of digits (spine over metacarpal/metatarsal)[2]
- Lymphadenopathy (regional, suggests infection)
- Delayed presentations: skin-colored or violaceous papules/nodules <5 mm (granuloma)[1]
11. Lab Studies
- Routine labs generally not needed for minor injuries
If signs of infection
- CBC with differential
- CRP/ESR
- Blood cultures (if systemic signs)
- Wound culture — alert lab to supplement media with NaCl for marine bacteria; use alkaline enrichment broth and thiosulfate-citrate-bile-sucrose (TCBS) agar for Vibrio detection[2]
- BMP if systemic envenomation or hemodynamic instability
- Lactate if concern for sepsis/necrotizing infection
- Inflammatory markers may be mildly elevated in osteoarticular involvement[4]
12. Imaging
- X-ray of affected area — first-line to identify retained radiopaque spine fragments (calcium carbonate spines are typically visible)[2][4]
- Spines were visible on plain radiographs in 8 of 12 cases in one series of osteoarticular injuries[4]
- Ultrasound — useful adjunct for superficial retained foreign bodies not seen on X-ray
- MRI — consider if concern for joint, tendon, or nerve involvement, or chronic granulomatous reaction
- CT — rarely needed; may help localize deep fragments
- Imaging is unnecessary for superficial injuries with no retained spines and no joint involvement
13. Special Tests
- Histopathology (for delayed presentations): sarcoid-like granulomas are the most common pattern; retained spine fragments are birefringent on polarized light microscopy[1]
- Point-of-care ultrasound — bedside identification of retained foreign bodies
- No validated clinical scoring systems specific to sea urchin injury
- Arthrocentesis if joint effusion present — rule out septic arthritis vs. foreign body synovitis[4]
14. ECG
- Not routinely indicated
- Consider if systemic envenomation with cardiovascular symptoms (hypotension, syncope)
- No specific ECG patterns associated with sea urchin envenomation
15. Assessment
- Sea urchin injury is usually a benign, self-limited process that responds dramatically to hot water soaks.[5] The clinical spectrum ranges from minor puncture wounds with transient pain to rare systemic envenomation with paralysis and cardiovascular collapse. Complications arise primarily from:
- Retained spines — causing chronic granulomatous reactions (1–6 month latency), synovitis, tenosynovitis, neuropathy[1][4-5][8]
- Secondary infection — particularly dangerous in immunocompromised patients and those with liver disease due to Vibrio species[2]
- Atypical presentations include delayed monoarthritis mimicking gout or septic arthritis[4]
16. Treatment Plan
Acute stabilization
- ABCs if systemic envenomation
- Hot water immersion at ~45°C (113°F) for 30–90 minutes — may repeat if pain recurs upon removal from water[2-3][6]
- Irrigate wound thoroughly
Spine removal
- Remove accessible spine fragments by gentle traction[1]
- Avoid aggressive digging — brittle spines fragment easily, and forceful removal can worsen the reaction[9]
- Formal wound exploration and débridement under aseptic conditions after soaking[2]
- Deep wounds (hand compartments, joints, fascial planes) → surgical exploration in the OR[2]
Medications
- Analgesia as above (local anesthetic, regional block, or opioids)[2]
- Antibiotics only if deep puncture, joint involvement, retained foreign body, immunosuppression, or signs of infection[2]
- Tetanus prophylaxis[5][7]
Delayed complications
- Granulomas: options include conservative management, surgical excision, or intralesional corticosteroids[8]
- Synovectomy with spine removal for osteoarticular involvement — consistently ensures full recovery[4]
17. Disposition
- Discharge — majority of cases; minor puncture wounds with adequate pain control and no systemic symptoms
Observation/admission criteria
- Systemic envenomation (>15–20 spines, hemodynamic instability, respiratory distress)[2]
- Rapidly progressive wound infection or necrotizing soft tissue infection
- Intra-articular or deep compartment spine penetration requiring OR exploration[2]
Specialist consultation triggers
- Hand surgery — spine in joint, tendon sheath, or near neurovascular structures[4-5]
- Orthopedics — intra-articular involvement with synovitis
- Infectious disease — fulminant marine wound infection, immunocompromised host
- Dermatology — chronic granulomatous reactions[8]
18. Follow Up / Return Precautions
- Follow-up in 48–72 hours for wound check if deep puncture, retained spines, or antibiotic initiation
Return precautions — seek immediate care for
- Increasing redness, swelling, warmth, or purulent drainage (infection)
- Fever or chills
- Red streaking from wound (lymphangitis)
- Worsening pain after initial improvement
- Numbness, weakness, or loss of function distal to injury
- Joint swelling or inability to move affected digit/joint
- Expected course: pain typically resolves over hours to a few days; superficial spines may be absorbed or extruded spontaneously[5][9]
- Counsel that delayed granulomas may appear 1–6 months later as small skin-colored or violaceous nodules — these are not dangerous but may require treatment[1]
- Advise wearing protective footwear (reef shoes) and gloves when wading or diving in rocky/coral environments[7]
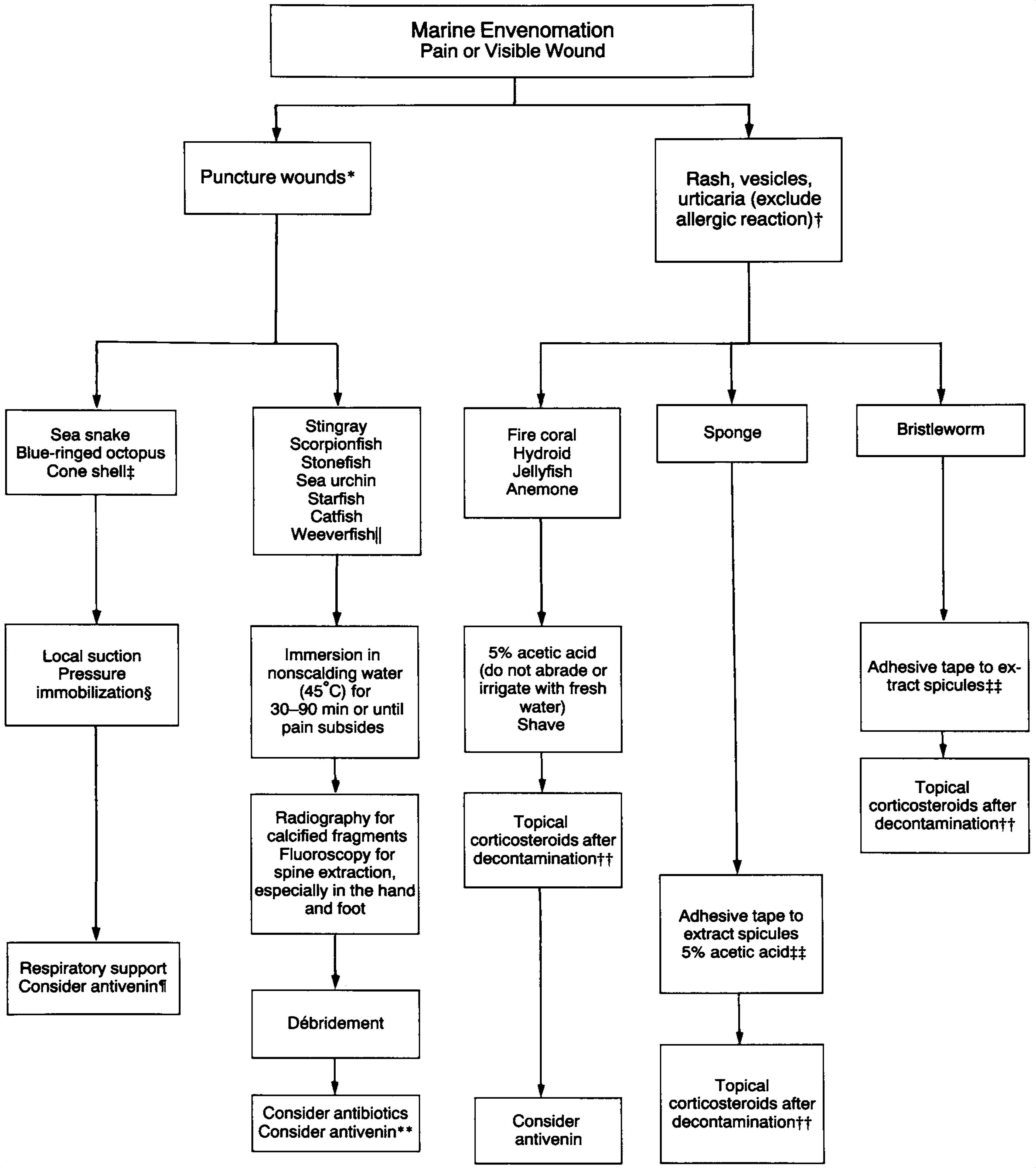
- The following algorithm from Auerbach's NEJM review summarizes the emergency approach to marine envenomations, including sea urchin puncture wounds:
- View full figure Figure 2. Approach to Emergency Management of a Marine Envenomation. Marine Envenomations. N Engl J Med. August 14, 1991.
References
1. Sea urchin spines in the stratum corneum: an early finding related to trauma. — Short JH, Sulit DJ. Journal of Cutaneous Pathology. 2014.
2. Marine Envenomations. — Auerbach PS. The New England Journal of Medicine. 1991.
3. Management of Extremity Trauma and Related Infections Occurring in the Aquatic Environment. — Noonburg GE. The Journal of the American Academy of Orthopaedic Surgeons. 2005.
4. Arthritis, Tenosynovitis, Fasciitis, and Bursitis Due to Sea Urchin Spines. A Series of 12 Cases in Réunion Island. — Guyot-Drouot MH, Rouneau D, Rolland JM, et al. Joint Bone Spine. 2000.
5. Hand Injuries From Sea Urchin Spines. — Strauss MB, MacDonald RI. Clinical Orthopaedics and Related Research. 1976.
6. Is Hot Water Immersion an Effective Treatment for Marine Envenomation?. — Atkinson PR, Boyle A, Hartin D, McAuley D. Emergency Medicine Journal : EMJ. 2006.
7. Poisonings, Envenomations, and Toxic Exposures During Travel. — Arthur Chang and Michael Yeh CDC Yellow Book. 2025.
8. Long-Term Management Options for Sea Urchin Injury: A Case Series. — James M, Bakkour W, Checkley A, Calonje E, Walker SL. Clinical and Experimental Dermatology. 2022.
9. Injuries From Sea Urchins. — Baden HP, Burnett JW. Southern Medical Journal. 1977.