Sedative-Hypnotic Toxicity
Sedative-hypnotic toxicity encompasses poisoning from benzodiazepines, barbiturates, non-benzodiazepine "Z-drugs" (zolpidem, zaleplon, zopiclone), GHB, chloral hydrate, and older agents (glutethimi…
Sedative-hypnotic toxicity encompasses poisoning from benzodiazepines, barbiturates, non-benzodiazepine "Z-drugs" (zolpidem, zaleplon, zopiclone), GHB, chloral hydrate, and older agents (glutethimide, ethchlorvynol, meprobamate). The hallmark is CNS depression ranging from drowsiness to coma, with respiratory compromise as the primary mechanism of death.[1-3] Isolated benzodiazepine overdose rarely causes life-threatening hemodynamic instability; most fatalities involve co-ingestion with opioids, alcohol, or other CNS depressants.[1-2] Barbiturates carry a significantly narrower therapeutic index and higher lethality than benzodiazepines.[4-5]
1. History
- Substance identification: Which agent(s), dose, formulation (immediate vs. extended release), route (oral, IV, rectal)
- Timing: Time of ingestion relative to presentation; single acute vs. staggered ingestion
- Intent: Accidental, recreational, or intentional (suicidal) — critical for disposition[6]
- Co-ingestants: Opioids, alcohol, TCAs, acetaminophen, other OTC medications — polysubstance ingestion is the rule, not the exception[2]
- Symptom progression: Drowsiness → confusion → slurred speech → ataxia → stupor → coma[3][5]
- Associated symptoms: Nausea/vomiting, anterograde amnesia, paradoxical agitation (rare)[3][5]
- Important negatives: Chest pain, seizure activity, trauma/falls during intoxication
2. Alarm Features
- Respiratory depression or apnea — the primary killer[1-2]
- Loss of protective airway reflexes (absent gag, pooling secretions)
- Hemodynamic instability (hypotension, bradycardia) — suggests barbiturate overdose, massive ingestion, or co-ingestant[5][7]
- Hypothermia[3][8]
- Markedly abnormal vital signs (lowered or elevated BP, HR, or RR) raise concern for additional drugs or alcohol[3]
- Fluctuating level of consciousness — classic for highly lipophilic older agents (glutethimide, ethchlorvynol) due to enterohepatic recirculation[4]
- Pulmonary edema or circulatory collapse — seen with massive barbiturate exposure[9-10]
3. Medications
Causative agents (by class)
- Benzodiazepines: alprazolam, diazepam, lorazepam, midazolam, clonazepam, etc.
- Barbiturates: phenobarbital, pentobarbital, secobarbital, butalbital
- Z-drugs: zolpidem, zaleplon, zopiclone/eszopiclone
- Others: GHB/GBL, chloral hydrate, meprobamate, glutethimide, ethchlorvynol
- Novel benzodiazepines: clonazolam, flualprazolam, etizolam (increasingly found in counterfeit pills)[11]
Antidote — Flumazenil (benzodiazepine-specific)
- Dose: 0.2 mg IV over 30 seconds, may repeat 0.3 mg then 0.5 mg increments q1 min, max 3 mg in overdose[12]
- Contraindications: chronic benzodiazepine dependence, co-ingestion of seizure-provoking drugs (TCAs), epilepsy on benzodiazepines, undifferentiated coma[1-2][12]
- Safe in low-risk settings: iatrogenic procedural sedation reversal, pediatric exploratory ingestions[1-2]
- Does not reverse barbiturate, GHB, or other non-benzodiazepine sedative toxicity
Medications to avoid
- Flumazenil in undifferentiated coma or suspected TCA co-ingestion (risk of refractory seizures and dysrhythmias)[1][12]
- Long-acting paralytics for RSI (may mask seizures) — prefer succinylcholine or rocuronium[6]
4. Diet
- NPO in obtunded patients due to aspiration risk
- Hydration: IV crystalloid for volume support; avoid oral intake until airway protective reflexes return
- No specific dietary triggers; however, alcohol co-ingestion synergistically potentiates CNS depression[1-2]
- Long-term: counsel on avoidance of alcohol with prescribed sedative-hypnotics
5. Review of Systems
- Neurologic: Level of consciousness, confusion, amnesia, ataxia, slurred speech, seizures
- Respiratory: Dyspnea, apnea, snoring/stridor (airway obstruction)
- Cardiovascular: Palpitations, syncope, chest pain
- GI: Nausea, vomiting (aspiration risk)
- Psychiatric: Suicidal ideation, depression, substance use history
- Musculoskeletal: Prolonged immobilization → rhabdomyolysis, compartment syndrome
- Skin: Pressure blisters ("barb burns") from prolonged immobility — classically associated with barbiturate coma
6. Collateral History and Family History
- Collateral is critical when the patient cannot provide history: EMS, family, friends, pill bottles, medication lists, pharmacy records[6]
- Photographs of medications at the scene are invaluable
- Psychiatric history: Prior suicide attempts, depression, access to medications
- Substance use history: Chronic benzodiazepine or opioid use (determines flumazenil safety and withdrawal risk)[1][13]
- Family history: Substance use disorders, psychiatric illness, seizure disorders
7. Risk Factors
- Polysubstance use — the single greatest risk factor for mortality[1-2]
- Chronic benzodiazepine or opioid prescriptions
- Psychiatric comorbidities (depression, anxiety, personality disorders)[13]
- Elderly patients — increased sensitivity, fall risk, prolonged sedation[5]
- Hepatic or renal impairment — impaired drug metabolism/excretion
- History of prior overdose or suicide attempt
- Access to large quantities of sedative-hypnotics
- Use of illicit benzodiazepines (counterfeit pills containing novel benzodiazepines or fentanyl)[2][11]
8. Differential Diagnosis
- Opioid overdose — miosis, more profound respiratory depression; responds to naloxone[2]
- Alcohol intoxication — similar presentation; check ethanol level
- Hypoglycemia — check point-of-care glucose immediately[6]
- Carbon monoxide poisoning — altered mental status, headache; check carboxyhemoglobin[8]
- Anticholinergic toxidrome — dry, flushed, mydriasis, tachycardia (opposite of sedative-hypnotic)
- Hepatic encephalopathy — asterixis, elevated ammonia
- Postictal state — history of seizure disorder
- Structural CNS pathology — stroke, subdural hematoma (especially after fall while intoxicated)[5]
- Hypothyroidism/myxedema coma — hypothermia, bradycardia
- Sepsis/meningitis — fever, altered mental status
- Key distinguishing features: The sedative-hypnotic toxidrome classically presents with normal or small pupils (unlike opioid miosis), hypothermia, hypotension, respiratory depression, and hyporeflexia without the anticholinergic signs (dry skin, mydriasis, tachycardia).[5]
9. Past Medical History
- Chronic benzodiazepine or sedative use — determines tolerance, withdrawal risk, and flumazenil safety[1][12]
- Seizure disorder — flumazenil contraindicated if benzodiazepines are used for seizure control[12]
- Psychiatric history — depression, prior suicide attempts, personality disorders
- Substance use disorders — alcohol, opioids, polysubstance
- Hepatic disease — impaired metabolism of most sedative-hypnotics
- Chronic pain on opioids — high risk for synergistic respiratory depression
- Prior overdose history
10. Physical Exam
Vital signs
- Bradypnea/apnea — most critical finding
- Hypotension (especially barbiturates)
- Bradycardia (mild)
- Hypothermia[3][5]
Neurologic
- Decreased level of consciousness (GCS documentation essential)[6]
- Slurred speech, ataxia, nystagmus[5]
- Hyporeflexia, hypotonia
- Normal or small pupils (not pinpoint like opioids)
- Absent gag reflex in severe cases
Skin
- Pressure blisters ("barb burns") — bullous lesions over pressure points from prolonged immobility (classically barbiturates but not pathognomonic)
- Check for transdermal patches (fentanyl), track marks[6]
Focused maneuvers
- Assess airway patency and protective reflexes
- Check for signs of trauma (subdural hematoma from fall)
- Compartment checks if prolonged immobilization suspected
11. Lab Studies
- Point-of-care glucose — immediate, to rule out hypoglycemia[6]
- Serum acetaminophen and salicylate levels — mandatory in all intentional overdoses and undifferentiated altered mental status[6]
- BMP (electrolytes, creatinine, bicarbonate, anion gap)[6]
- ABG/VBG — assess for hypercapnia and respiratory acidosis; characterize acid-base status[6][14]
- Hepatic function panel — baseline and to evaluate for co-ingestant hepatotoxicity
- Serum ethanol level
- CK — if prolonged immobilization suspected (rhabdomyolysis)
- Pregnancy test — women of childbearing age[6]
- Barbiturate level — quantitative phenobarbital level useful for guiding enhanced elimination[7][15]
- Urine drug screen — limited acute utility; high false-positive/negative rates; does not detect novel benzodiazepines. Useful for confirming exposure but should not guide acute management.[6][11]
- Lactate — if hemodynamic instability
12. Imaging
- Chest X-ray: Indicated if hypoxic, tachypneic, or obtunded — evaluate for aspiration pneumonitis, ARDS, or pulmonary edema[6]
- CT head without contrast: If altered mental status is disproportionate to expected toxicity, concern for trauma/fall, or focal neurologic findings[5]
- Abdominal imaging: Generally not indicated; plain films have low sensitivity for most sedative-hypnotics. Consider CT abdomen if body packing suspected[6]
- Imaging is unnecessary in straightforward, witnessed benzodiazepine ingestions with expected clinical course
13. Special Tests
- Glasgow Coma Scale — serial assessments to track clinical trajectory[6]
- Poison Control consultation (800-222-1222) — recommended for all significant ingestions[6]
- Quantitative drug levels: Phenobarbital level is clinically useful (correlates with severity and guides enhanced elimination). Benzodiazepine levels are generally not clinically useful.[7][15]
- Bedside ultrasound: Assess cardiac function and IVC if hemodynamically unstable
- End-tidal CO₂ monitoring: Useful for detecting hypoventilation, especially during observation
14. ECG
- Obtain ECG in all significant sedative-hypnotic overdoses, especially with unknown co-ingestants[6]
- Isolated benzodiazepine/barbiturate overdose: Typically shows sinus bradycardia or normal sinus rhythm; no characteristic morphologic changes
Critical role is to rule out co-ingestants
- Prolonged QRS → sodium channel blocker (TCA) co-ingestion[6][16]
- Prolonged QTc → multiple psychotropic co-ingestants; QTc >500 ms is highest risk for adverse cardiovascular events[17-18]
- AV block → beta-blocker or calcium channel blocker co-ingestion
- Continuous cardiac monitoring recommended until the patient is free of drug influence[17]
- A QTc >500 ms on admission ECG in drug overdose carries an OR of 11.2 for adverse cardiovascular events[18]
15. Assessment
Severity stratification
- Mild: Drowsiness, slurred speech, ataxia — maintains airway and protective reflexes
- Moderate: Stupor, significant hypotension, diminished reflexes — requires close monitoring
- Severe: Coma, respiratory depression/apnea, hemodynamic collapse — requires airway intervention and ICU care
Key clinical pearls
- Isolated benzodiazepine overdose is rarely fatal in adults; always suspect co-ingestants when life-threatening features are present[1-2]
- Barbiturate overdose has a much narrower therapeutic index and higher mortality[4-5][7]
- Older lipophilic agents (glutethimide, ethchlorvynol) cause fluctuating consciousness due to enterohepatic recirculation — observe for several days[4]
- Long-acting benzodiazepines (diazepam, chlordiazepoxide) may cause intoxication lasting several days due to active metabolites[4]
- Novel/designer benzodiazepines (clonazolam) may cause prolonged sedation (up to 30 hours) and are not detected on standard immunoassay screens[11]
Complications
- Aspiration pneumonitis/pneumonia
- Rhabdomyolysis and compartment syndrome from prolonged immobilization
- Pressure injuries/blisters
- Hypothermia
- Anoxic brain injury (from prolonged hypoxia)
16. Treatment Plan
Initial stabilization (ABCs)
- Airway: Head-tilt/chin-lift, nasopharyngeal airway; intubate if unable to protect airway[1][6]
- Breathing: Bag-mask ventilation → endotracheal intubation if needed; supplemental O₂
- Circulation: IV access, crystalloid bolus for hypotension; vasopressors if refractory
Decontamination
- Activated charcoal (1 g/kg, max 50 g): Consider if within 1 hour of ingestion and airway is intact/protected[4][6]
- Multiple-dose activated charcoal (MDAC): Indicated for phenobarbital poisoning (reduces half-life from ~80 to ~40 hours)[6][15]
Antidote
- Flumazenil — reserved for low-risk, known benzodiazepine-only ingestions (e.g., iatrogenic procedural sedation, pediatric exploratory ingestion)[1-2][12]
- Dose: 0.2 mg IV over 30 sec → 0.3 mg → 0.5 mg increments q1 min, max 3 mg[12]
- Do not use in undifferentiated coma, chronic benzodiazepine users, suspected TCA co-ingestion, or seizure disorder patients on benzodiazepines[1][12]
- No antidote exists for barbiturates, GHB, or other non-benzodiazepine sedative-hypnotics
Enhanced elimination (barbiturates)
- Urinary alkalinization with IV sodium bicarbonate (target urine pH ~7.5) — enhances excretion of phenobarbital[4][15]
- Hemodialysis/CRRT: Consider for life-threatening barbiturate toxicity with refractory hypotension[14-15]
Supportive care
- Continuous pulse oximetry, capnography, cardiac monitoring
- Rewarming for hypothermia
- DVT prophylaxis if prolonged immobilization
- Frequent repositioning to prevent pressure injuries and rhabdomyolysis
- Psychiatric evaluation once medically cleared (if intentional ingestion)
17. Disposition
Admission criteria (ICU)
- Intubation or need for mechanical ventilation
- Hemodynamic instability requiring vasopressors
- Severe barbiturate poisoning requiring enhanced elimination
- GCS ≤8 or declining mental status
- Significant co-ingestants requiring monitoring (e.g., acetaminophen, TCAs)
Observation
- Moderate sedation with stable vitals — observe until clinically improving and able to protect airway
- Minimum 4–6 hours observation for short-acting agents; longer for long-acting benzodiazepines or barbiturates[4]
- Older lipophilic agents (glutethimide, ethchlorvynol) require several days of observation due to fluctuating levels[4]
Discharge criteria
- Alert, ambulatory, tolerating PO, stable vitals for appropriate observation period
- No respiratory depression
- Psychiatric clearance if intentional ingestion
- Safe disposition plan (not returning to environment with access to lethal means)
Specialist consultation triggers
- Toxicology/Poison Control: All significant ingestions[6]
- Psychiatry: All intentional overdoses
- Nephrology: If hemodialysis considered for barbiturate poisoning[14-15]
18. Follow Up / Return Precautions
Follow-up timing
- PCP or psychiatry follow-up within 48–72 hours for intentional ingestions
- Substance use disorder referral if applicable
- Medication reconciliation — reassess need for sedative-hypnotic prescriptions
- Return precautions — instruct patient/family to return immediately for:
- Recurrent drowsiness or difficulty arousing (especially with long-acting agents or if flumazenil was used, as re-sedation can occur)[12]
- Difficulty breathing or noisy breathing
- Confusion, agitation, or seizures (may indicate withdrawal in chronic users)[5][19]
- Fever, cough, or chest pain (aspiration pneumonitis)
- Dark urine or muscle pain (rhabdomyolysis)
Patient counseling
- Avoid alcohol and other CNS depressants
- Secure medications to prevent accidental pediatric ingestion
- Lethal means counseling and safe storage/disposal of unused medications
- Expected recovery: mild cases resolve within hours; long-acting agents may cause residual sedation for days[4]
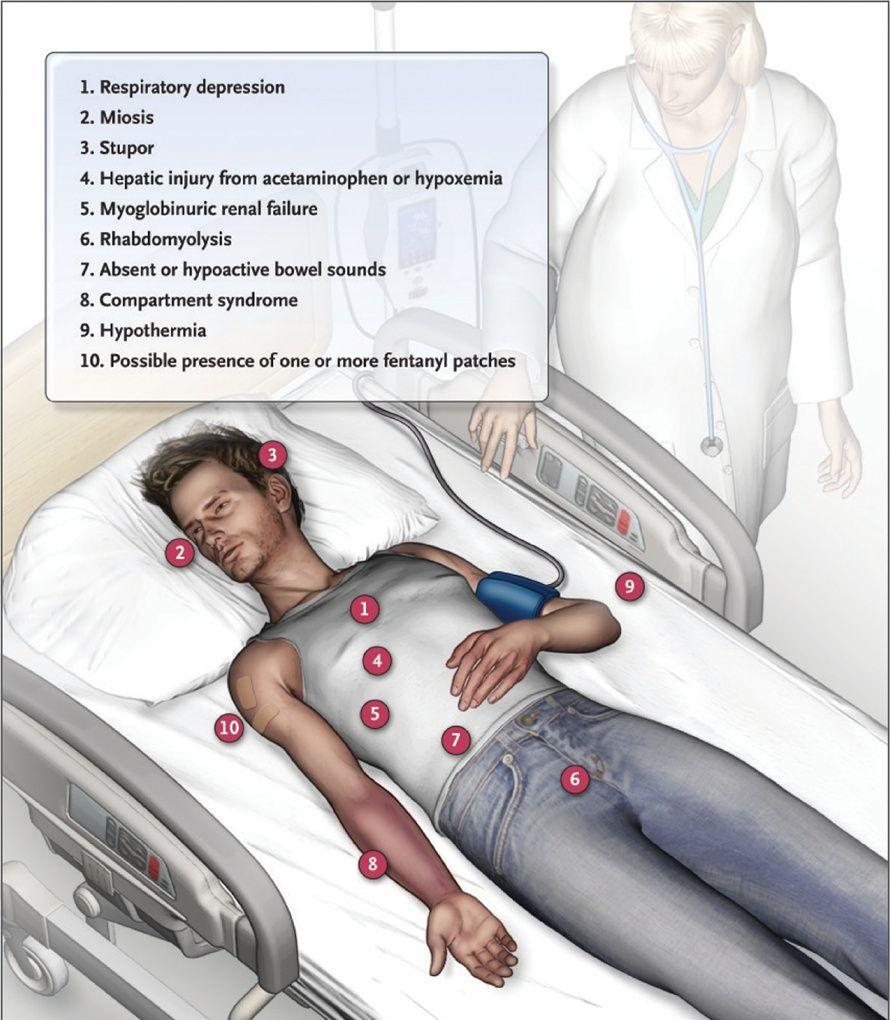
- Relevant images 2 items
- Clinical Findings in Opioid Analgesic Intoxication.
- NEJM July 11, 2012
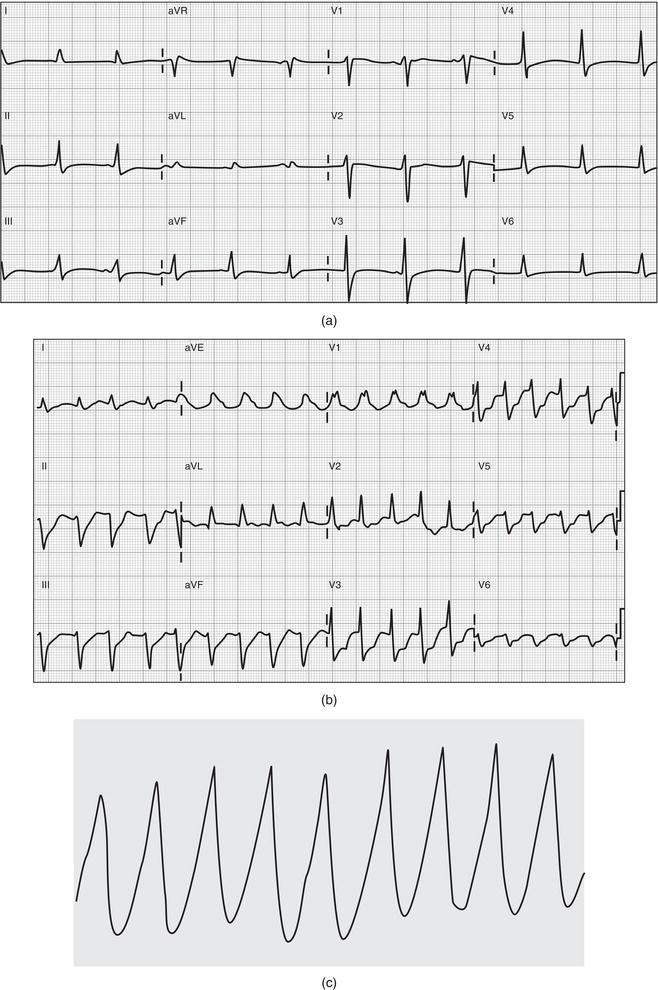
- (a) Minimally widened QRS complex in the setting of a cardiotoxic ingestion with sodium channel blocking ability. (b) Tricyclic antidepressant overdose with characteristic changes on ECG, including sinus tachycardia, deep S wave in lead I, R wave in lead aVr, and widened QRS complex. (c) Ventricular tachycardia related to sodium channel blockade.
- Electrocardiagram in Emergency and Acute Care December 31, 2022
References
1. 2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Lavonas EJ, Akpunonu PD, Arens AM, et al. Circulation. 2023.
2. Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Cao D, Arens AM, Chow SL, et al. Circulation. 2025.
3. FDA Drug Label. — Updated date: 2025-04-29. Food and Drug Administration.
4. Role of the Primary Care Physician in Problems of Substance Abuse. — Weaver MF, Jarvis MA, Schnoll SH. Archives of Internal Medicine. 1999.
5. Diagnostic and Statistical Manual of Mental Disorders. — Dilip V. Jeste, Jeffrey A. Lieberman, David Fassler, et al American Psychiatric Association (2022). 2022.
6. Acute Medication Poisoning. — Vega IL, Griswold MK, Laskey D. American Family Physician. 2024.
7. FDA Drug Label. — Updated date: 2017-06-30. Food and Drug Administration.
8. Toxin-Induced Coma and Central Nervous System Depression. — Krause M, Hocker S. Neurologic Clinics. 2020.
9. FDA Drug Label. — Updated date: 2026-05-05. Food and Drug Administration.
10. FDA Drug Label. — Updated date: 2026-01-28. Food and Drug Administration.
11. Non-Fatal Intoxications Involving the Novel Benzodiazepine Clonazolam: Case Series From the Emerging Drugs Network of Australia - Victoria Project. — Syrjanen R, Greene SL, Castle JW, et al. Clinical Toxicology. 2023.
12. FDA Drug Label. — Updated date: 2020-01-03. Food and Drug Administration.
13. The Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations when Benzodiazepine Risks Outweigh Benefits. — Emily Brunner, Chwen-Yuen A. Chen, Tracy Klein, et al American College of Medical Toxicology (2024). 2024.
14. Poisoning by Abnormally High Blood Phenobarbital Concentration Treated With Extracorporeal Therapy. — Kohara S, Kamijo Y, Seki S, Hasegawa E. The American Journal of Emergency Medicine. 2023.
15. Enhanced Elimination in Acute Barbiturate Poisoning - A Systematic Review. — Roberts DM, Buckley NA. Clinical Toxicology. 2011.
16. Electrocardiographic Abnormalities Associated With Poisoning. — Delk C, Holstege CP, Brady WJ. The American Journal of Emergency Medicine. 2007.
17. Update to Practice Standards for Electrocardiographic Monitoring in Hospital Settings: A Scientific Statement From the American Heart Association. — Sandau KE, Funk M, Auerbach A, et al. Circulation. 2017.
18. Validation of the Prognostic Utility of the Electrocardiogram for Acute Drug Overdose. — Manini AF, Nair AP, Vedanthan R, Vlahov D, Hoffman RS. Journal of the American Heart Association. 2017.
19. Guidelines for Managing Substance Withdrawal in Jails. — Jeffrey Alvarez MD CCHP, Andrew F. Angelino MD, Oscar Aviles CPM CJM CCE CCHP, et al American Society of Addiction Medicine (2023). 2023.