Septic Shock
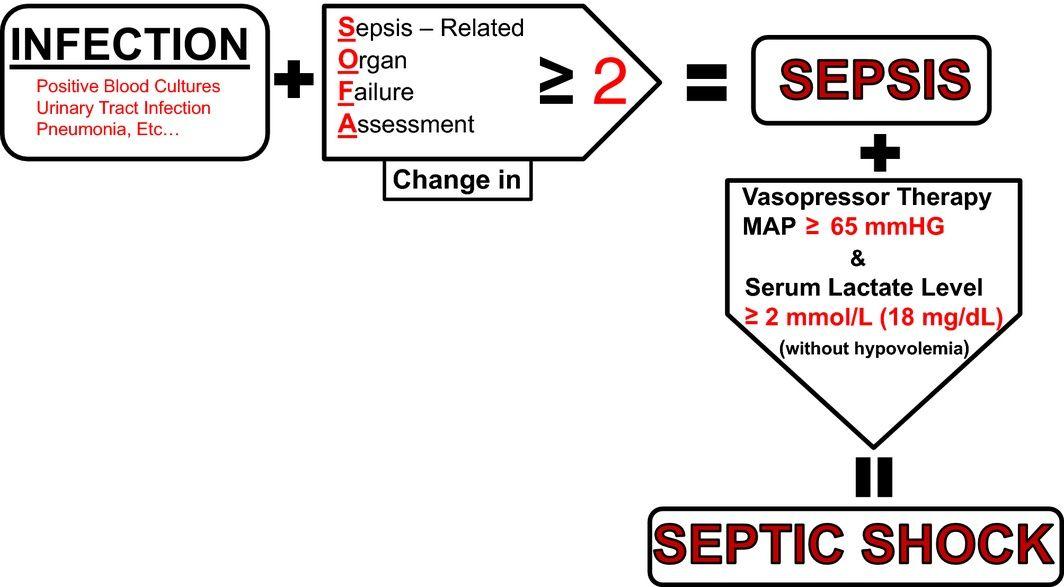
Septic shock is defined as a subset of sepsis with persistent hypotension requiring vasopressor therapy to maintain MAP ≥65 mmHg and serum lactate >2 mmol/L despite adequate fluid resuscitation (Se…
Septic shock is defined as a subset of sepsis with persistent hypotension requiring vasopressor therapy to maintain MAP ≥65 mmHg and serum lactate >2 mmol/L despite adequate fluid resuscitation (Sepsis-3 criteria).[1-2] It carries a mortality rate of approximately 40–50% and affects approximately 49 million sepsis cases worldwide annually, with 11 million sepsis-related deaths.[1][3]
1. History
- Source-directed HPI: Cough/dyspnea (pneumonia — most common source), dysuria/flank pain (UTI), abdominal pain (intra-abdominal), wound erythema/drainage (skin/soft tissue)[4]
- Timing and progression: Onset of symptoms, rapidity of decline, duration of fever, recent antibiotic use, prior hospitalizations
- Associated symptoms: Fever/chills, rigors, confusion, decreased urine output, malaise, myalgias
- Important negatives: Chest pain (ACS mimic), drug ingestion/overdose, recent procedures/surgeries, indwelling devices (lines, catheters, prosthetics), travel history, animal/insect exposures
- Medication history: Immunosuppressants, chemotherapy, beta-blockers (may mask tachycardia), antipyretics (may mask fever), recent antibiotics[5]
2. Alarm Features
- Hypotension refractory to fluid resuscitation (SBP <90, MAP <65)
- Altered mental status / acute encephalopathy
- Lactate ≥4 mmol/L (severe tissue hypoperfusion)
- Skin mottling, cyanosis, prolonged capillary refill time
- Oliguria/anuria (<0.5 mL/kg/hr)
- Rapidly escalating vasopressor requirements
- New-onset organ dysfunction: respiratory failure, coagulopathy (DIC), acute kidney injury[5-6]
- Sepsis can be difficult to recognize in the elderly, immunocompromised, and those presenting very early in the illness course[6]
3. Medications
Empiric Antimicrobials
- Septic shock: Administer immediately, ideally within 1 hour of recognition (strong recommendation)[7]
- Broad-spectrum coverage targeting gram-negative and gram-positive organisms based on local susceptibility patterns[6]
- Add MRSA coverage (e.g., vancomycin) if high-risk (recent healthcare exposure, known colonization, skin/soft tissue source)[8]
- Consider antifungal coverage if high-risk for invasive fungal infection (prolonged ICU stay, TPN, immunosuppression)[9]
- Prolonged beta-lactam infusions (after initial bolus) improve outcomes over intermittent boluses[9]
Vasopressors
- Norepinephrine — first-line vasopressor (strong recommendation)[8]
- Vasopressin (0.03 U/min) — add if norepinephrine dose reaches 0.25–0.5 mcg/kg/min[5][9]
- Epinephrine — third-line if MAP goals not met with norepinephrine + vasopressin[8]
- Can be initiated via peripheral IV (≥20-gauge) safely; do not delay for central access[6][10]
Corticosteroids
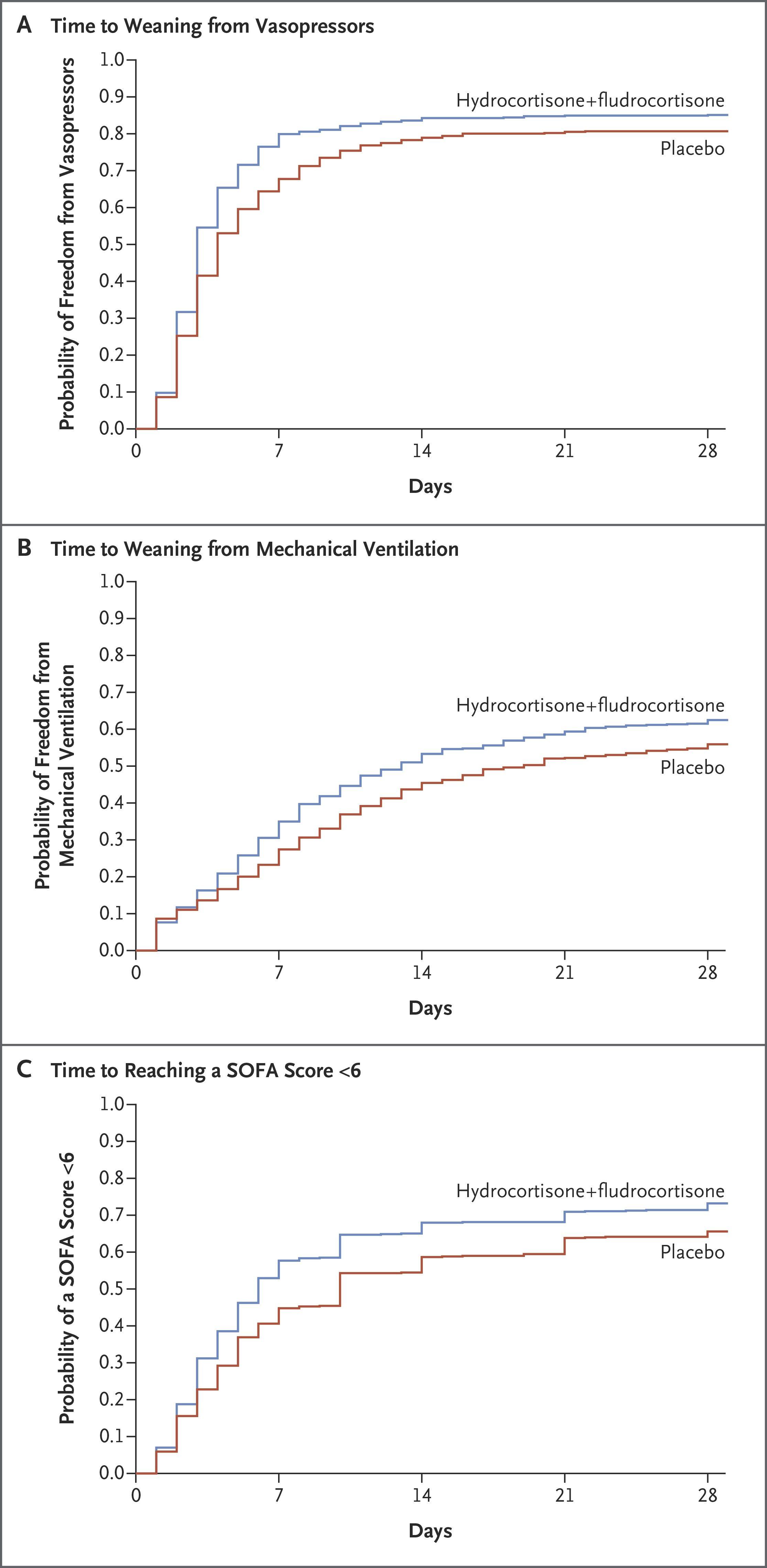
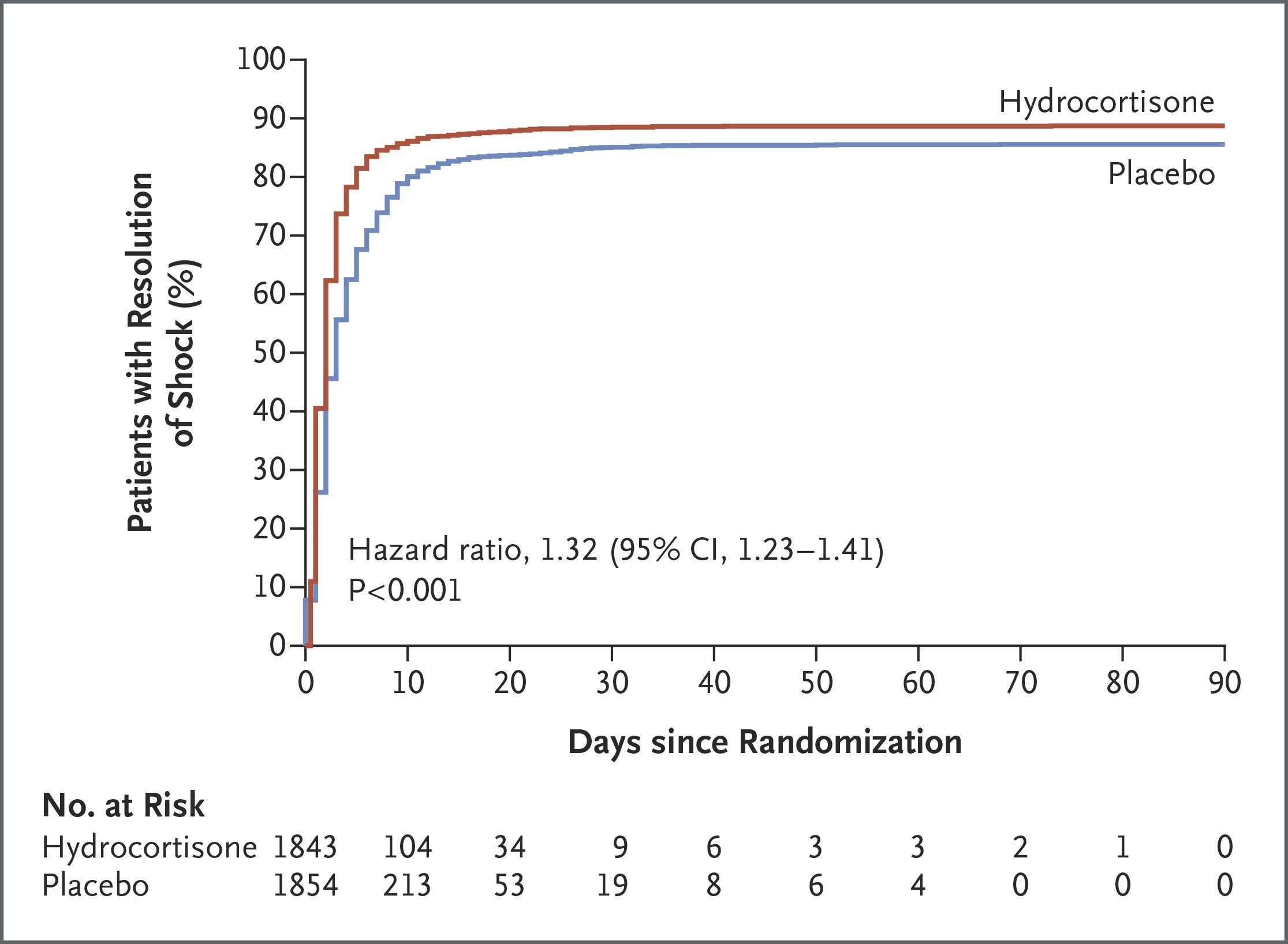
- Hydrocortisone 200 mg/day IV (50 mg q6h or continuous infusion) ± fludrocortisone 50 mcg daily for patients with ongoing vasopressor requirements (conditional recommendation)[7-8]
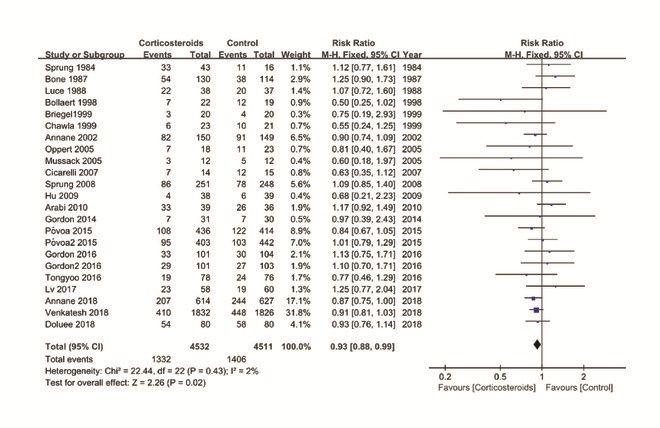
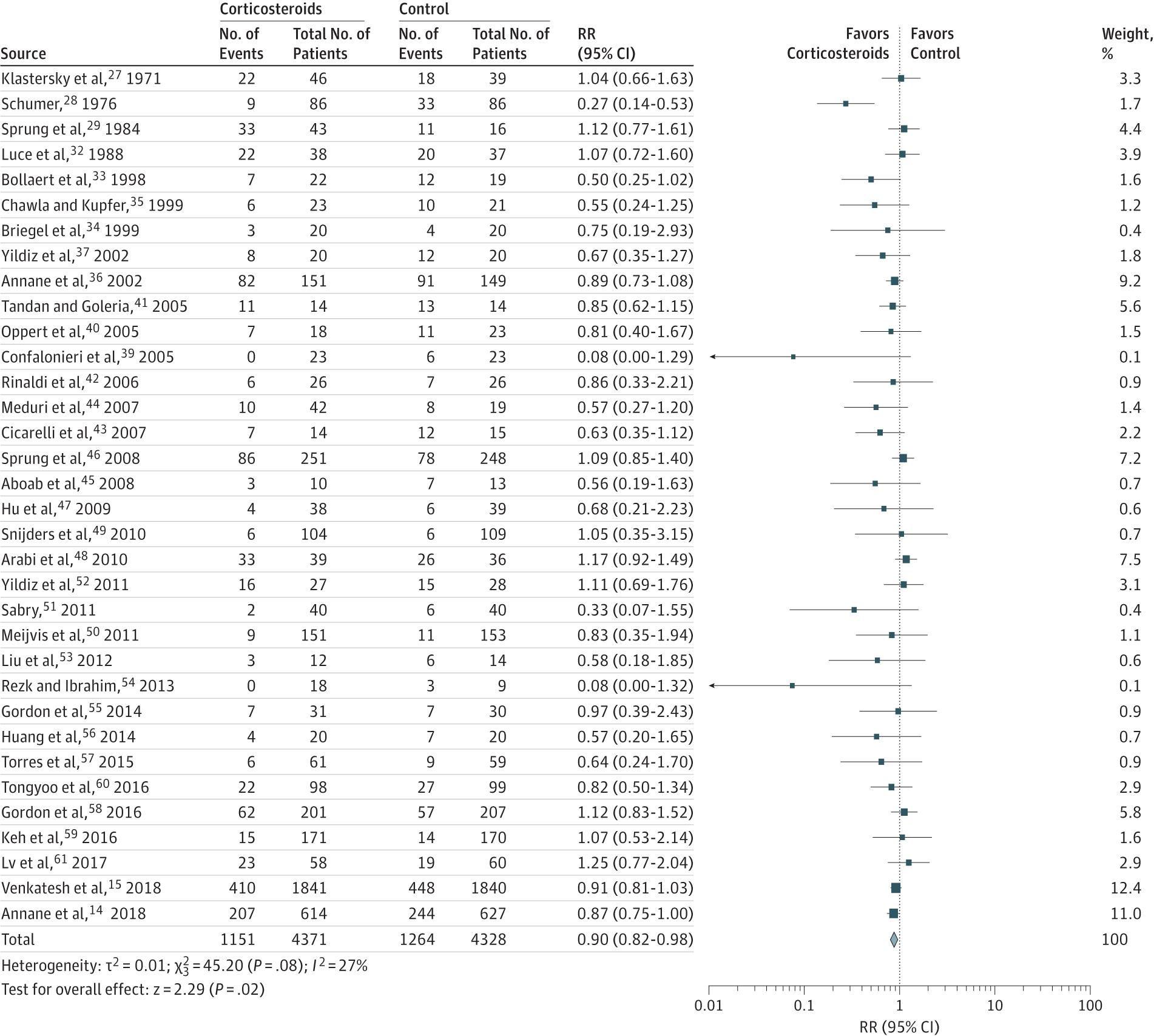
- Accelerates shock reversal; uncertain mortality benefit[7-8]
- Monitor for hyperglycemia and hypernatremia[7]
Medications to Avoid
- Hydroxyethyl starch — increased mortality[9]
- Synthetic colloid gelatin — insufficient evidence[9]
- Terlipressin — suggested against[8]
4. Diet
- NPO initially in critically ill/intubated patients
- Early enteral nutrition (within 24–48 hours of ICU admission) is preferred over parenteral nutrition once hemodynamically stable
- Avoid overfeeding; target caloric goals per ICU nutrition guidelines
- Adequate hydration is addressed through IV fluid resuscitation
5. Review of Systems
- Neurologic: Confusion, lethargy, agitation (septic encephalopathy)
- Respiratory: Dyspnea, tachypnea, cough, hypoxia (pneumonia, ARDS)
- Cardiovascular: Palpitations, chest pain (septic cardiomyopathy, new-onset atrial fibrillation)
- GI: Nausea, vomiting, diarrhea, abdominal pain (intra-abdominal source)
- GU: Dysuria, frequency, flank pain (urinary source)
- Skin: Rash, wound changes, erythema, warmth (cellulitis, necrotizing fasciitis)
- Musculoskeletal: Joint pain/swelling (septic arthritis), back pain (epidural abscess, osteomyelitis)[4][11]
6. Collateral History and Family History
- Collateral: Baseline mental status, functional status, recent hospitalizations, recent procedures, indwelling devices, known colonization with resistant organisms, advance directives/goals of care
- Family history: Immunodeficiency syndromes; genetic polymorphisms in innate immunity genes may influence sepsis susceptibility, though clinical utility is limited[12]
- Social context: Injection drug use (endocarditis), alcohol use disorder (aspiration pneumonia, SBP), homelessness, nursing home residence
7. Risk Factors
- Age: Extremes of age (infants, elderly ≥65)[12-13]
- Immunosuppression: HIV/AIDS, chemotherapy, transplant recipients, chronic corticosteroid use[13-14]
- Chronic organ failure: CKD (especially dialysis-dependent), cirrhosis, COPD, heart failure[15-16]
- Malignancy[15-16]
- Diabetes mellitus[13][17]
- Recent surgery or invasive procedures
- Indwelling devices: Central lines, urinary catheters, prosthetic joints/valves[11]
- Male sex, Black race (associated with higher incidence and mortality)[12][16]
- Cirrhosis is a particularly strong independent predictor of mortality in septic shock (adjusted OR 1.85)[16]
8. Differential Diagnosis
- Approximately 20–40% of patients with suspected sepsis in the ED are ultimately diagnosed with a noninfectious sepsis mimic.[6] Critical differentials include:
- Cardiogenic shock — elevated JVP, pulmonary edema, cold extremities, echo with reduced EF[18]
- Hypovolemic shock — hemorrhage, dehydration, third-spacing
- Anaphylaxis — urticaria, angioedema, exposure history
- Pulmonary embolism — pleuritic chest pain, RV strain on echo/CT
- Adrenal crisis — hypotension refractory to fluids, hyperkalemia, hyponatremia
- Toxic ingestion/overdose — medication history, toxidrome features[19]
- Neuroleptic malignant syndrome / serotonin syndrome — medication history, rigidity, hyperthermia[11]
- Thyroid storm — tachycardia, hyperthermia, agitation, thyroid history
- Hemophagocytic lymphohistiocytosis (HLH) — pancytopenia, hyperferritinemia, hepatosplenomegaly[20]
- Pancreatitis — epigastric pain, lipase elevation
- Neurogenic shock — spinal cord injury, bradycardia with hypotension[19]
9. Past Medical History
- Prior episodes of sepsis (increased risk of recurrence)
- Chronic diseases: diabetes, CKD, cirrhosis, COPD, heart failure, malignancy
- Surgical history: splenectomy (encapsulated organisms), recent abdominal/urologic surgery
- Immunosuppressive medications or conditions
- Known colonization with MDR organisms (MRSA, VRE, ESBL-producing organisms)
- Baseline cardiac function (history of heart failure increases risk of septic cardiomyopathy)[21]
10. Physical Exam
Vital Signs
- Hypotension (SBP <90, MAP <65), tachycardia (HR >90), tachypnea (RR >22), fever (>38.3°C) or hypothermia (<36°C), hypoxia
Focused Exam
- General: Toxic appearance, diaphoresis, altered mentation
- Skin: Mottling (especially over knees), delayed capillary refill (>3 sec), petechiae/purpura (DIC, meningococcemia), wound erythema/crepitus (necrotizing fasciitis)
- HEENT: Nuchal rigidity (meningitis), dental abscess, sinus tenderness
- Lungs: Crackles, decreased breath sounds, dullness to percussion
- Cardiovascular: New murmur (endocarditis), JVD, peripheral edema
- Abdomen: Peritoneal signs, distension, tenderness (intra-abdominal source)
- GU: CVA tenderness, suprapubic tenderness
- Extremities: Joint effusion/erythema (septic arthritis), IV site infection
- Spine: Midline tenderness (epidural abscess)[6][22]
11. Lab Studies
Initial Labs
- Serum lactate — cornerstone biomarker; >2 mmol/L defines septic shock; serial trending guides resuscitation[1][8]
- CBC with differential — leukocytosis (>12,000), leukopenia (<4,000), bandemia (>10% bands)
- BMP/CMP — creatinine (AKI), glucose (hyperglycemia common), electrolytes
- Hepatic function panel — bilirubin, transaminases (hepatic dysfunction)
- Coagulation studies — PT/INR, fibrinogen, D-dimer (DIC screening)
- Blood cultures (≥2 sets from different sites) — obtain before antibiotics if possible without delaying treatment
- Urinalysis and urine culture
- Procalcitonin — may support diagnosis but should not be used in isolation to exclude sepsis[4][23]
- ABG/VBG — acid-base status, PaO2
- Type and screen if hemorrhage or surgical intervention anticipated
Monitoring Parameters
- Serial lactate (target decreasing trend toward normal)[8]
- Urine output (target ≥0.5 mL/kg/hr)
- Capillary refill time (adjunct to guide resuscitation)[8]
12. Imaging
- Chest X-ray — first-line for suspected pulmonary source (pneumonia, empyema, ARDS)
- CT abdomen/pelvis with IV contrast — suspected intra-abdominal source (abscess, perforation, cholangitis)
- CT head — altered mental status without clear cause, concern for CNS infection
- Point-of-care ultrasound (POCUS) — assess cardiac function (EF, RV dilation), IVC collapsibility (volume status), lung (B-lines, effusion), free fluid (FAST)[18]
- CT chest — if CXR nondiagnostic and pulmonary source suspected
- MRI spine — suspected epidural abscess
- Imaging should be source-directed based on clinical suspicion[4]
13. Special Tests
Scoring Systems
- SOFA score — defines organ dysfunction (increase ≥2 points = sepsis); superior prognostic accuracy in ICU[2][24]
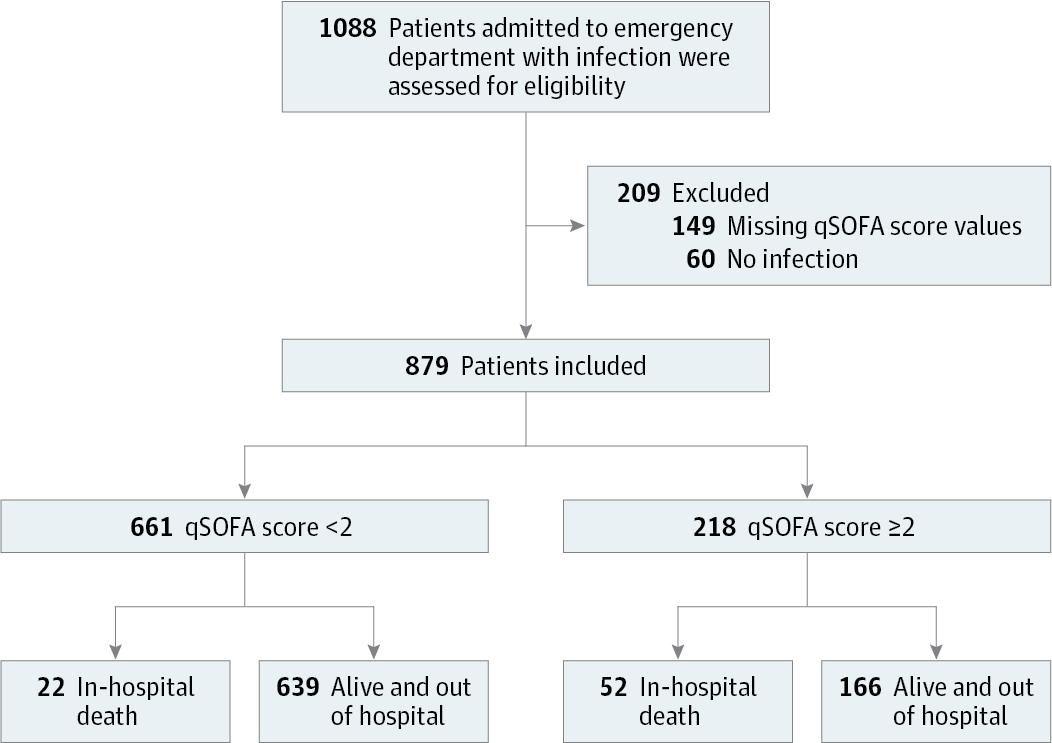
- qSOFA (RR ≥22, altered mentation, SBP ≤100) — bedside screening tool for non-ICU settings; limited sensitivity[9][25]
- APACHE II / SAPS II — ICU severity scoring; higher scores independently predict mortality[16]
Point-of-Care Tests
- Bedside echocardiography — assess for septic cardiomyopathy (biventricular dysfunction), cardiac tamponade, PE[18][26]
- Passive leg raise test — dynamic assessment of fluid responsiveness (>10% increase in stroke volume suggests fluid responsiveness)[5][8]
- Multiplex PCR pathogen panels — rapid pathogen identification from blood cultures[5]
14. ECG
- Sinus tachycardia — most common finding (39% of sepsis patients)[27]
- New-onset atrial fibrillation/flutter — occurs in ~9% of sepsis patients; associated with worse outcomes (OR 2.19 for poor outcomes)[27]
- QT prolongation — common (54.4%); associated with adverse outcomes[27]
- ST-T wave changes — may represent demand ischemia or septic cardiomyopathy; must differentiate from ACS[28-29]
- ECG should be obtained in all patients with septic shock to evaluate for arrhythmia, ischemia, and cardiac dysfunction[28]
- Troponin elevation is common in sepsis and does not necessarily indicate ACS; correlate with clinical picture and echocardiography[28]
15. Assessment
- Definition (Sepsis-3): Sepsis with vasopressor requirement to maintain MAP ≥65 mmHg AND lactate >2 mmol/L after adequate fluid resuscitation.[1-2]
Severity Stratification
- Mortality increases with higher SOFA scores (1.21 per point increase), higher APACHE II scores (1.10 per point increase), and elevated lactate (1.13 per 1 mmol/L increase)[16]
- Respiratory source of sepsis carries higher mortality than urinary source[16]
- AKI at presentation is an independent predictor of mortality (adjusted OR 1.88)[16]
Atypical Presentations
- Elderly patients may present with hypothermia, confusion, or functional decline without fever[5]
- Immunocompromised patients may lack typical inflammatory signs[6]
- Beta-blockers may mask tachycardia; antipyretics may mask fever[5]
Complications
- ARDS, DIC, AKI, hepatic dysfunction, septic cardiomyopathy, ICU-acquired weakness, long-term cognitive impairment[3]
16. Treatment Plan
Immediate Stabilization (Hour-1 Bundle)
- Measure lactate (remeasure if initial >2 mmol/L)
- Obtain blood cultures before antibiotics (do not delay antibiotics)
- Administer broad-spectrum IV antibiotics within 1 hour[7]
- Begin IV crystalloid resuscitation: at least 30 mL/kg within 3 hours for hypoperfusion/shock[7]
- Balanced crystalloids (e.g., lactated Ringer's) preferred over normal saline[9]
- Use adjusted body weight for BMI >30[7]
- Start vasopressors if hypotension persists despite fluids — target MAP ≥65 mmHg[8]
Vasopressor Escalation
- Norepinephrine → add vasopressin (0.03 U/min) → add epinephrine[8]
- For cardiac dysfunction with persistent hypoperfusion: add dobutamine to norepinephrine or use epinephrine alone[8]
Adjunctive Therapies
- Hydrocortisone 200 mg/day IV ± fludrocortisone 50 mcg daily for refractory shock[7-8]
- Source control — drain abscesses, remove infected devices, debride necrotic tissue as soon as feasible[3]
- Lung-protective ventilation if intubated (tidal volume 6 mL/kg ideal body weight, plateau pressure <30 cmH2O)
- Glucose management — target glucose ≤180 mg/dL
- VTE prophylaxis and stress ulcer prophylaxis per ICU protocols
Ongoing Resuscitation
- Guide further fluids using dynamic measures (passive leg raise, stroke volume variation, pulse pressure variation) rather than static measures (CVP)[8-9]
- Target decreasing lactate trend and capillary refill time normalization[5][8]
17. Disposition
Admission Criteria
- All patients with septic shock require ICU admission[8]
- ICU admission should occur within 6 hours of recognition; delays increase mortality[8]
Observation Indications
- Patients with sepsis without shock who respond to initial resuscitation may be appropriate for step-down/intermediate care with close monitoring
Specialist Consultation Triggers
- Critical care/intensivist — all septic shock patients
- Surgery — source control needs (abscess drainage, bowel perforation, necrotizing fasciitis)
- Infectious disease — MDR organisms, unclear source, immunocompromised host, failure to improve
- Cardiology — new cardiac dysfunction, concern for endocarditis or ACS
18. Follow Up / Return Precautions
Inpatient Monitoring
- Serial lactate q2–4h until trending down
- Continuous hemodynamic monitoring (arterial line recommended for vasopressor use)
- Daily reassessment of antibiotic spectrum; narrow based on culture/sensitivity data
- Reassess for source control if failing to improve
Post-Discharge
- Survivors are at high risk for rehospitalization within 12 months, cognitive impairment, physical disability, and psychological sequelae (PTSD, depression)[3]
- Follow-up within 1–2 weeks of discharge with PCP
- Medication reconciliation (antibiotics completion, chronic medication adjustments)
- Screening for post-sepsis syndrome: fatigue, cognitive changes, functional decline
- Return precautions: fever, recurrent hypotension, confusion, decreased urine output, worsening symptoms at infection site
- Sepsis should be considered in all patients presenting with severe infection or acute organ dysfunction that is not clearly attributable to a noninfectious cause.
- — Nuala J. Meyer, M.D., et al., University of Pennsylvania Perelman School of Medicine and other institutions
- Sepsis and Septic Shock. N Engl J Med. December 4, 2024.
- Relevant images 12 items
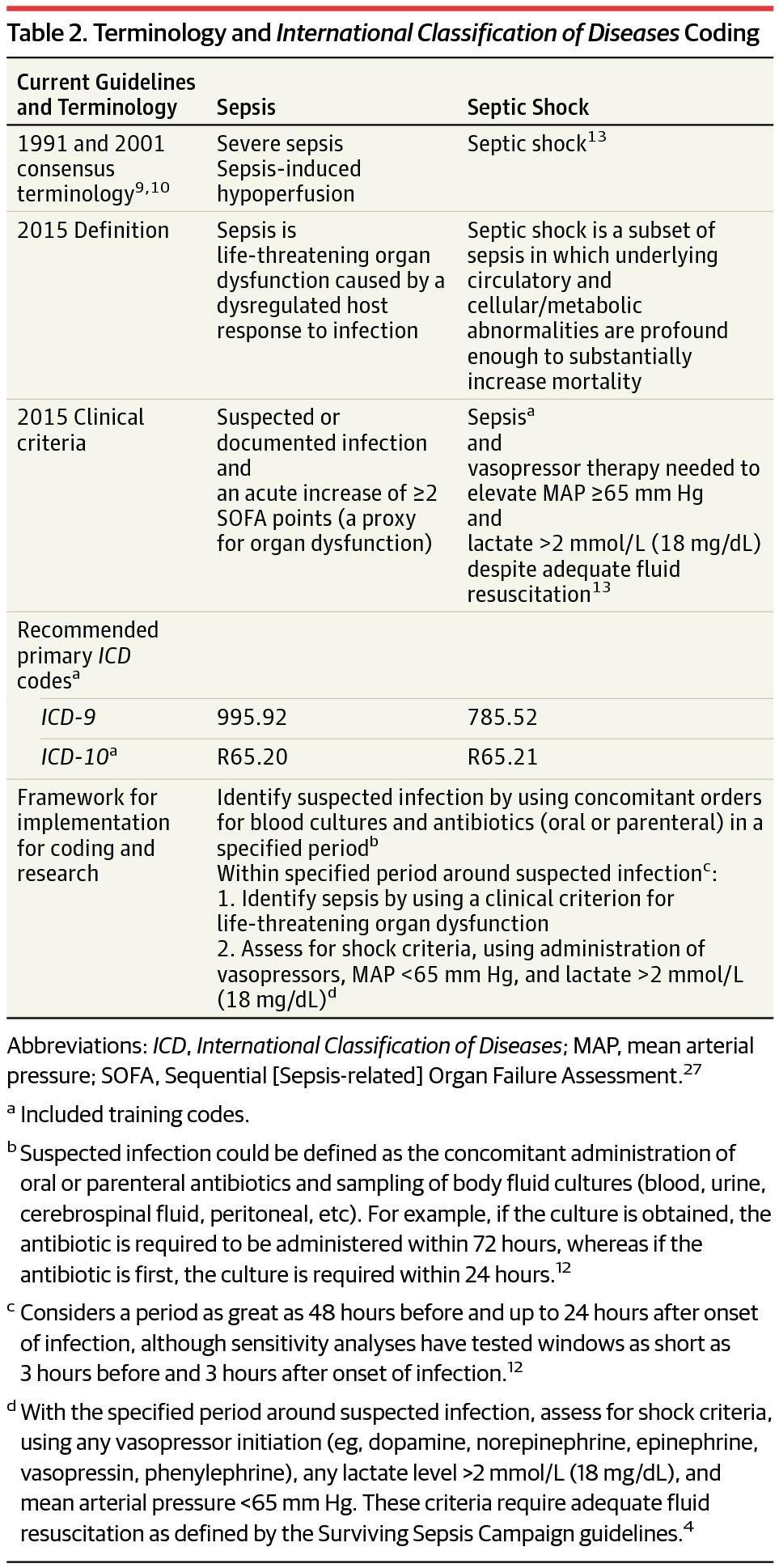
- Terminology and International Classification of Diseases Coding
- JAMA February 22, 2016
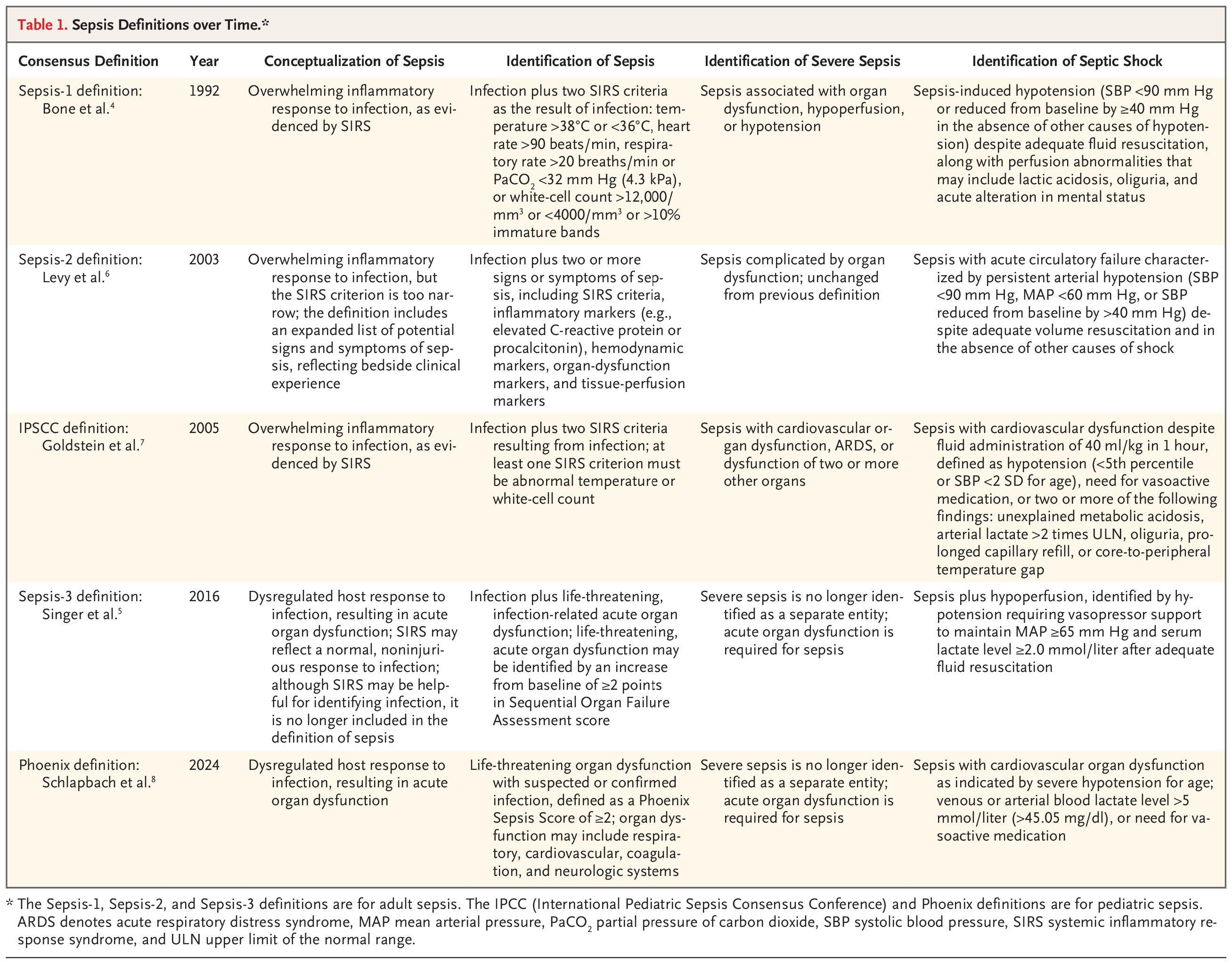
- Sepsis Definitions over Time.*
- NEJM December 4, 2024
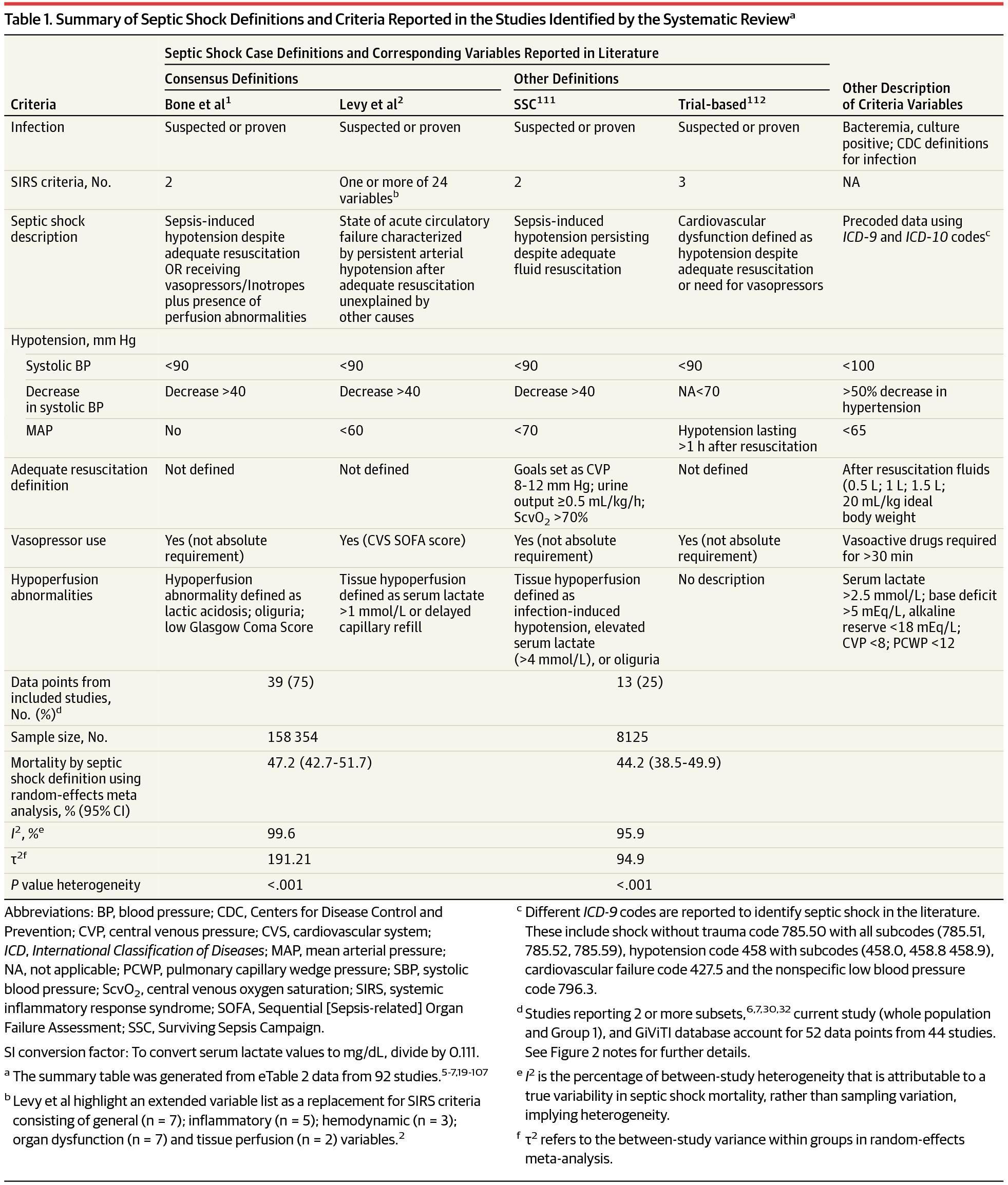
- Summary of Septic Shock Definitions and Criteria Reported in the Studies Identified by the Systematic Reviewa
- JAMA February 22, 2016
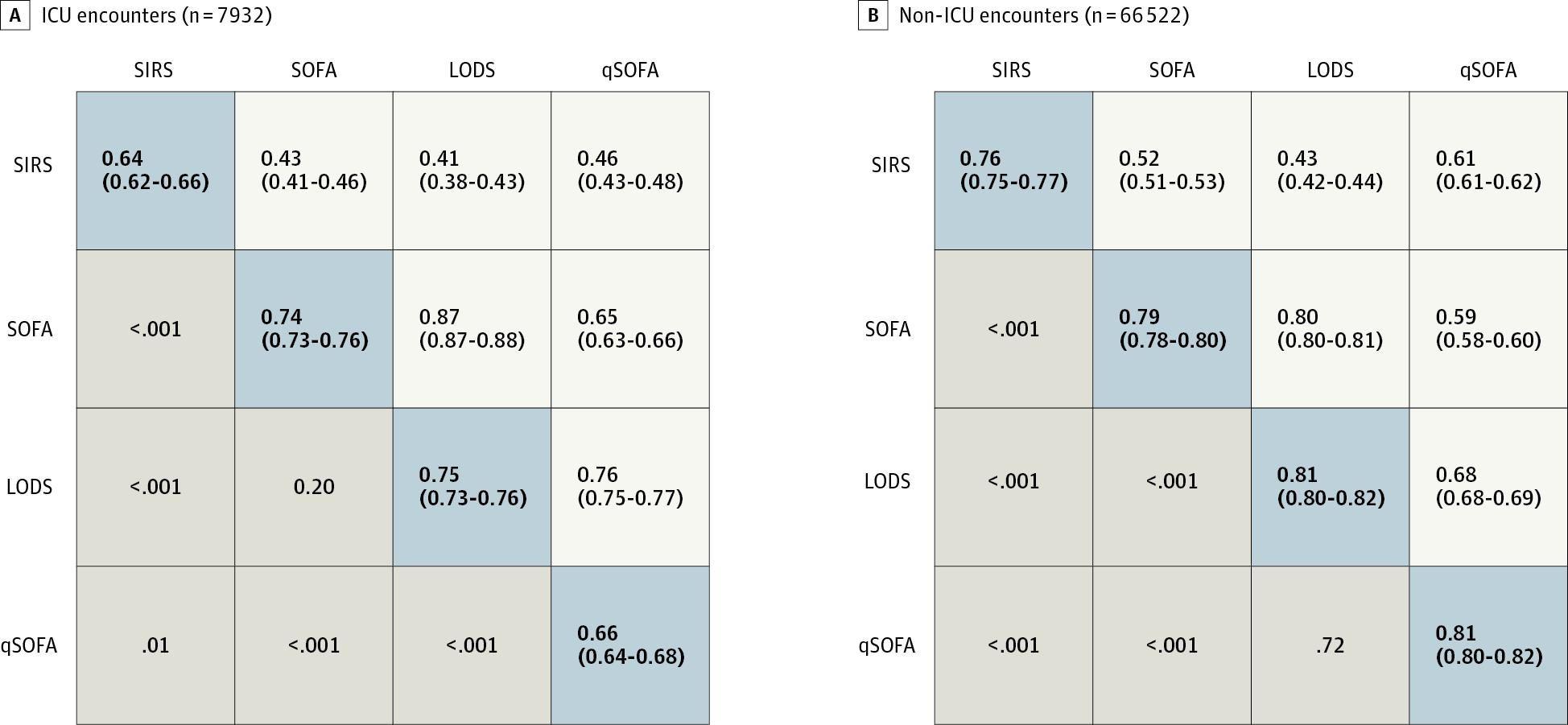
- Area Under the Receiver Operating Characteristic Curve and 95% Confidence Intervals for In-Hospital Mortality of Candidate Criteria (SIRS, SOFA, LODS, and qSOFA) Among Suspected Infection Encounters in the UPMC Validation Cohort (N = 74 454)
- JAMA February 22, 2016
- Definition of septic shock and associated mortality.
- Immunological Reviews October 31, 2016
- Flow Diagram of Study to Validate qSOFA Scoring
- JAMA January 16, 2017
- Time to Weaning from Vasopressors, to Weaning from Mechanical Ventilation, and to Reaching a SOFA Score below 6.
- NEJM February 28, 2018
- Forest plots of comparison corticosteroids versus control for 28‐day all‐cause mortality.
- BioMed Research International January 21, 2019
- Cumulative Incidence Function of Time from Randomization to Resolution of Shock.
- NEJM February 28, 2018
- Mortality at 28 Days in All Trials Evaluating Corticosteroids Among Patients With Sepsis
- JAMA Intern Med January 31, 2019
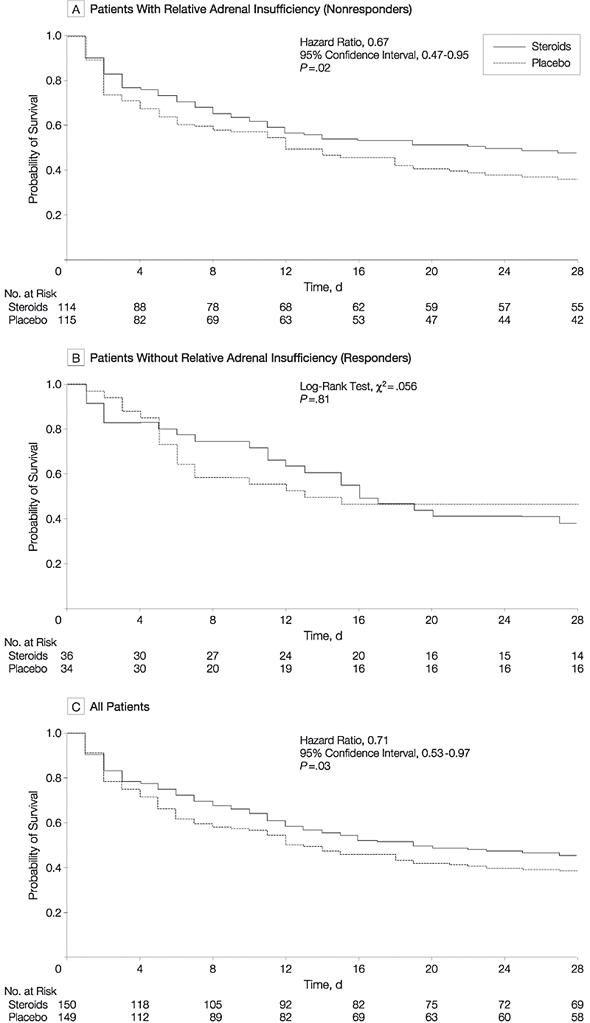
- Figure 2
- JAMA August 20, 2002
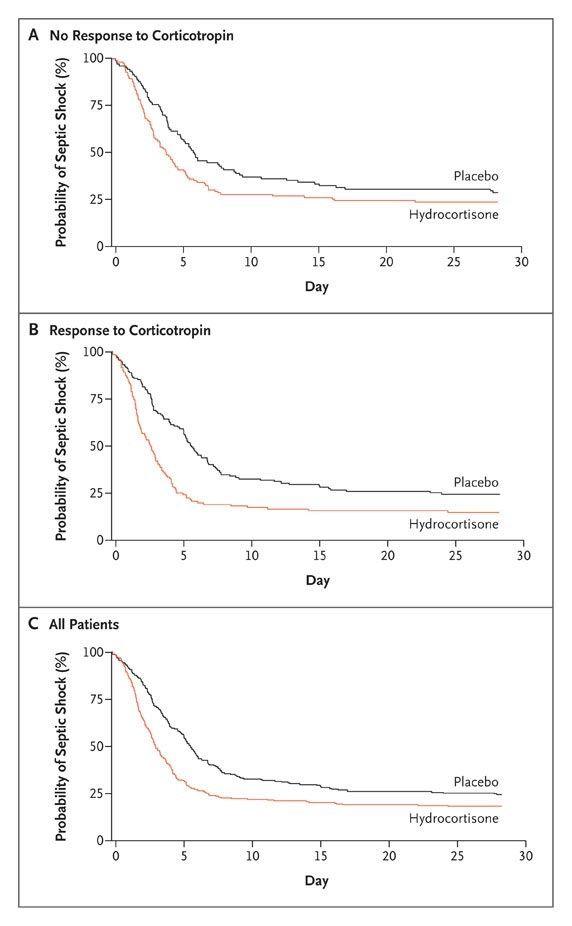
- Kaplan–Meier Curves for the Time to Reversal of Shock.
- NEJM January 9, 2008
References
1. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). — Shankar-Hari M, Phillips GS, Levy ML, et al. The Journal of the American Medical Association. 2016.
2. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). — Singer M, Deutschman CS, Seymour CW, et al. The Journal of the American Medical Association. 2016.
3. Current Standard of Care for Septic Shock. — Delaney A, Borges-Sa M, Chew MS, et al. Intensive Care Medicine. 2025.
4. Emergency Medicine Updates: Evaluation and Diagnosis of Sepsis and Septic Shock. — Long B, Gottlieb M. The American Journal of Emergency Medicine. 2025.
5. Sepsis and Septic Shock. — Meyer NJ, Prescott HC. The New England Journal of Medicine. 2024.
6. Early Care of Adults With Suspected Sepsis in The Emergency Department and Out-of-Hospital Environment: A Consensus-Based Task Force Report. — Yealy DM, Mohr NM, Shapiro NI, et al. Annals of Emergency Medicine. 2021.
7. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026. — Prescott HC, Antonelli M, Alhazzani W, et al. Critical Care Medicine. 2026.
8. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. — Evans L, Rhodes A, Alhazzani W, et al. Critical Care Medicine. 2021.
9. Surviving Sepsis: Updated Guidelines From the Society of Critical Care Medicine. — Arnold MJ. American Family Physician. 2022.
10. Emergency Medicine Updates: Management of Sepsis and Septic Shock. — Long B, Gottlieb M. The American Journal of Emergency Medicine. 2025.
11. Consideration of Occult Infection and Sepsis Mimics in the Sick Patient Without an Apparent Infectious Source. — Boushra MN, Miller SN, Koyfman A, Long B. The Journal of Emergency Medicine. 2019.
12. Severe Sepsis and Septic Shock. — Angus DC, van der Poll T. The New England Journal of Medicine. 2013.
13. Risk Factors for Hospitalization Due to Community-Acquired Sepsis - A Population-Based Case-Control Study. — Henriksen DP, Pottegård A, Laursen CB, et al. PloS One. 2015.
14. Septic Shock. — Annane D, Bellissant E, Cavaillon JM. Lancet. 2005.
15. The Impact of Comorbidities and COVID-19 on the Evolution of Community Onset Sepsis. — de Araújo GC, Pardini A, Lima C. Scientific Reports. 2023.
16. Prognostic Factors Associated With Mortality in Septic Shock: A Systematic Review and Meta-Analysis. — Jung RG, Gupta A, Stotts C, et al. The Lancet. Respiratory Medicine. 2026.
17. Impact of Cardiovascular and Metabolic Comorbidities on Severity and Outcomes of Hospital-Acquired Sepsis in Intensive Care Patients: A Case-Control Study. — Roy A, Krishnasamy V, Mitra S, et al. BMC Infectious Diseases. 2026.
18. Circulatory Shock. — Vincent JL, De Backer D. The New England Journal of Medicine. 2013.
19. Clinical Mimics: An Emergency Medicine-Focused Review of Sepsis Mimics. — Long B, Koyfman A. The Journal of Emergency Medicine. 2017.
20. Sepsis in Patients Who Are Immunocompromised: Diagnostic Challenges and Future Therapies. — Deinhardt-Emmer S, Chousterman BG, Schefold JC, et al. The Lancet. Respiratory Medicine. 2025.
21. Identifying Predictors and Determining Mortality Rates of Septic Cardiomyopathy and Sepsis-Related Cardiogenic Shock: A Retrospective, Observational Study. — Hendrickson KW, Cirulis MM, Burk RE, et al. PloS One. 2023.
22. A Plea for Personalization of the Hemodynamic Management of Septic Shock. — De Backer D, Cecconi M, Chew MS, et al. Critical Care. 2022.
23. Sepsis: Diagnosis and Management. — Gauer R, Forbes D, Boyer N. American Family Physician. 2020.
24. Prognostic Accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for In-Hospital Mortality Among Adults With Suspected Infection Admitted to the Intensive Care Unit. — Raith EP, Udy AA, Bailey M, et al. The Journal of the American Medical Association. 2017.
25. Plasma Interleukin-6 Concentration for the Diagnosis of Sepsis in Critically Ill Adults. — Molano Franco D, Arevalo-Rodriguez I, Roqué I Figuls M, et al. The Cochrane Database of Systematic Reviews. 2019.
26. The Septic Heart: Current Understanding of Molecular Mechanisms and Clinical Implications. — Martin L, Derwall M, Al Zoubi S, et al. Chest. 2019.
27. Association of Electrocardiogram Abnormalities With Clinical Outcomes in Emergency Department Sepsis Patients. — Kotruchin P, Chuehongthong M, Tangpaisarn T, et al. The Western Journal of Emergency Medicine. 2026.
28. Current Challenges in Understanding, Diagnosing and Managing Sepsis-Induced Cardiac Dysfunction. — Paraschiv C, Popescu Moraru MR, Paduraru LF, et al. Journal of Critical Care. 2025.
29. Septic Cardiomyopathy or Myocardial Infarction?: A Case Report of Septic Shock With ST-segment Elevation on ECG. — Gao H, Wang X, Yang Q. Medicine. 2025.