Smallpox (Variola)
Smallpox is a CDC Category A bioterrorism agent caused by variola virus (an orthopoxvirus), eradicated globally since 1980 but remaining a critical biothreat. Any single suspected case constitutes…
Smallpox is a CDC Category A bioterrorism agent caused by variola virus (an orthopoxvirus), eradicated globally since 1980 but remaining a critical biothreat. Any single suspected case constitutes an international public health emergency requiring immediate notification of local/state health departments and the CDC.[1-3] The fatality rate of variola major is approximately 25–30% in unvaccinated individuals.[1][3]
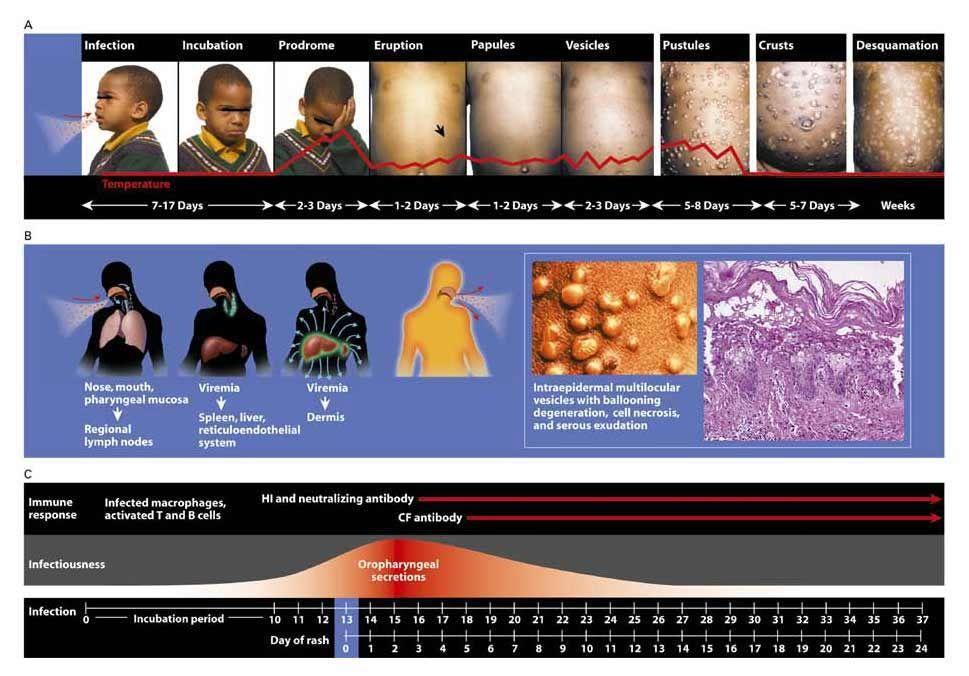
The following figure from Breman & Henderson (NEJM, 2002) illustrates the clinical progression, pathogenesis, and immune response timeline of smallpox:
1. History
- Exposure context: Any case in the modern era implies deliberate release (bioterrorism) or laboratory accident — ask about travel, occupational exposure to research labs, contact with known cases, or suspicious events[1][4]
- Incubation period: 7–17 days (mean 10–14 days); ask about timeline from potential exposure[2][5]
- Prodrome (1–4 days before rash): Abrupt onset of high fever (38.9–40.6°C), severe prostration, headache, backache (up to 90% of patients), chills, vomiting, severe abdominal pain[2][5-6]
- Rash progression: Enanthem (oral mucosa) → exanthem starting on face → spreading to extremities and trunk within 24–48 hours; macules → papules (day 2) → vesicles (days 4–5) → pustules (day 7) → crusting (2–3 weeks)[5-6]
- Key distinguishing features: Lesions all in the same stage of development on any given body part; centrifugal distribution (face/extremities > trunk); lesions on palms and soles; deep-seated, firm, round, well-circumscribed[5]
- Important negatives: Absence of lymphadenopathy (distinguishes from mpox); no crops of lesions at different stages (distinguishes from varicella)[6-7]
2. Alarm Features
- Hemorrhagic smallpox: Dusky erythema, petechiae, frank hemorrhages into skin/mucous membranes; death by day 5–6 of rash; ~98% fatality; more common in pregnant women[1][8]
- Flat (malignant) smallpox: Soft, flat, confluent lesions that do not project above skin; 94–97% case fatality rate[2][8]
- Confluent ordinary smallpox: Mortality ~50–60% vs. 10% for discrete ordinary type[5][8]
- Encephalitis: Occurs in <1% of cases; decreased consciousness, seizures[2][6]
- Respiratory decompensation: Bronchopneumonia, secondary bacterial infection — more likely with severe/confluent disease[2]
- Delirium/encephalopathy: ~15% of patients during febrile stage; febrile seizures in ~7% of children <5 years[6]
3. Medications
Antiviral Treatment
- Tecovirimat (TPOXX): FDA-approved for treatment of smallpox in adults and pediatric patients ≥3 kg[9-10]
- Oral dosing (14-day course): 13–<25 kg: 200 mg q12h; 25–<40 kg: 400 mg q12h; 40–<120 kg: 600 mg q12h; ≥120 kg: 600 mg q8h[10]
- IV formulation available for patients unable to take oral[10-11]
- Mechanism: Inhibits VP37 envelope wrapping protein, blocking extracellular viral dissemination[12-13]
- Efficacy not proven in human smallpox (approved under FDA Animal Rule); may be reduced in immunocompromised patients[4][10]
- CYP450 interactions — check drug-drug interactions, especially with antiretrovirals[14]
- Cidofovir / Brincidofovir: Alternative antivirals with in vitro activity against variola; potential role if tecovirimat resistance emerges[15-16]
- Vaccinia Immune Globulin Intravenous (VIGIV): Available for passive immunization; indicated for vaccine complications (eczema vaccinatum, progressive vaccinia)[3][15]
Contraindicated/Cautions
- No role for standard antivirals (acyclovir, valacyclovir) — these target herpesvirus thymidine kinase, not orthopoxviruses
- Tecovirimat resistance mutations have been identified, particularly in immunocompromised patients[12]
4. Diet
- No specific dietary triggers or restrictions
- Hydration is critical — patients with extensive oropharyngeal enanthem may have difficulty swallowing, leading to dehydration[2][8]
- Nutritional support and caloric supplementation for severely ill, bedridden patients
- Soft/liquid diet may be necessary during the pustular phase due to oral mucosal involvement
5. Review of Systems
- Constitutional: Fever, rigors, prostration, malaise (universal in prodrome)[2][5]
- Dermatologic: Rash character, distribution, stage of evolution, palms/soles involvement
- HEENT: Oral enanthem, dysphagia, eye involvement (keratitis, conjunctival lesions)[2]
- Respiratory: Cough (not prominent but assess for pneumonia), dyspnea[2]
- Neurologic: Headache, backache, delirium, seizures, altered consciousness[6]
- GI: Abdominal pain, vomiting (prodromal), diarrhea
- MSK: Arthritis/joint pain (especially in children — osteomyelitis variolosa in 2–5%)[2][6]
- Lymphatic: Absence of lymphadenopathy (helps distinguish from mpox)[5-6]
6. Collateral History and Family History
- Contact tracing is paramount: Identify all face-to-face and household contacts for immediate vaccination and surveillance[1-2]
- Vaccination history: Prior smallpox vaccination (pre-1980s) may confer partial protection — modified/milder disease in previously vaccinated individuals[2][5]
- Occupational history: Laboratory workers handling orthopoxviruses, military personnel
- Travel history: Relevant only in context of bioterrorism investigation
- Pregnancy status: Pregnant women are at increased risk for hemorrhagic smallpox and higher mortality[1][8]
- Immunocompromised status: HIV, transplant recipients, chemotherapy — increased risk of severe disease[10]
7. Risk Factors
- Unvaccinated status: Global vaccination ceased in the 1980s; the vast majority of the current population is susceptible[4][15]
- Pregnancy: Disproportionately high risk for hemorrhagic smallpox; CFR 28% vs. 8% in non-pregnant women in historical data[8]
- Immunosuppression: Reduced efficacy of both vaccination and antiviral therapy[10]
- Young children and elderly: Higher morbidity and mortality
- Close/household contact with an infected individual: Primary mode of person-to-person spread via respiratory droplets and direct contact[1]
- Healthcare workers without vaccination: High-risk occupational exposure[1][3]
8. Differential Diagnosis
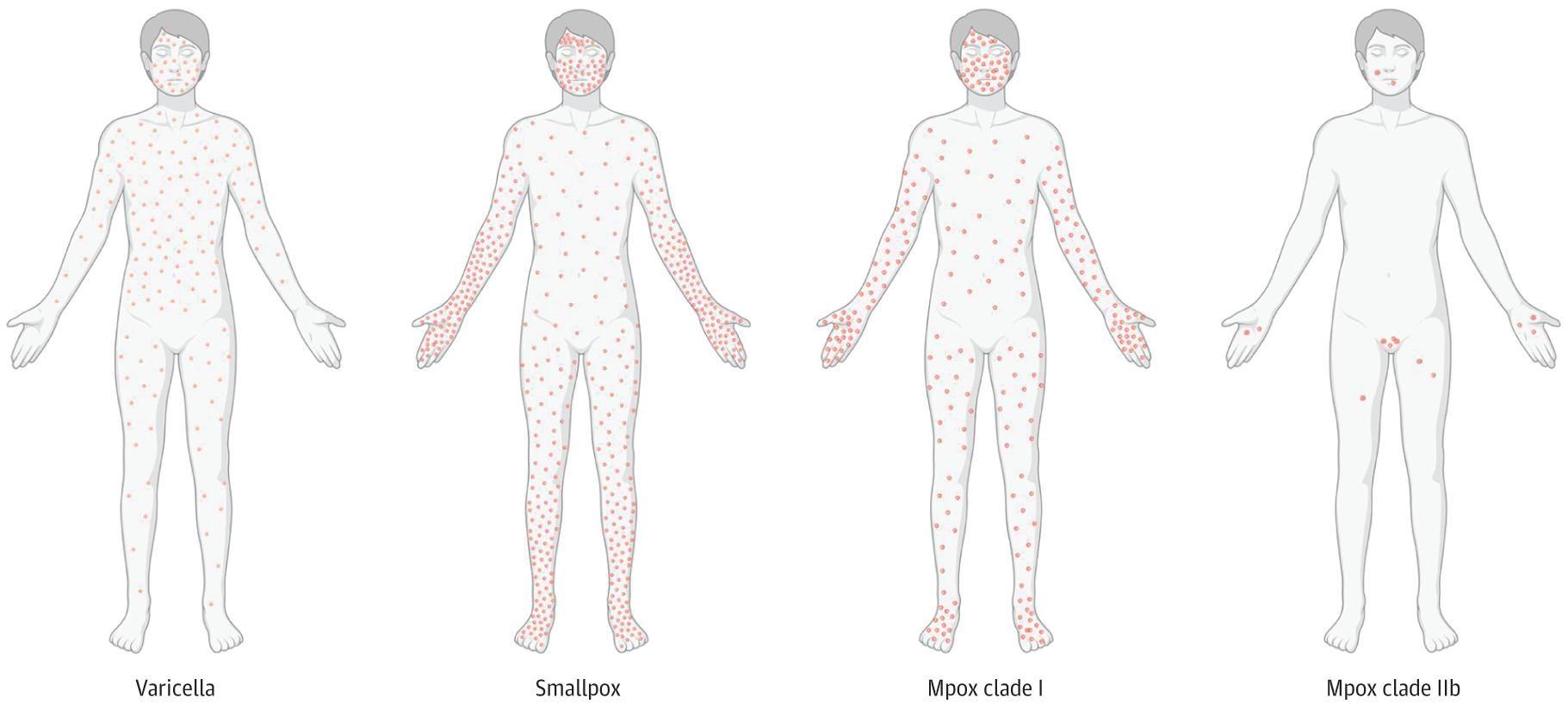
- The following figure compares the distribution of skin lesions in varicella, smallpox, and mpox:
- Export Diagnosis Key Distinguishing Features References Chickenpox (Varicella) Superficial "dewdrop" vesicles; lesions in multiple stages (crops); centripetal distribution (trunk > extremities); rarely on palms/soles; milder prodrome[1-2]
- Mpox (Monkeypox) Similar deep-seated lesions and centrifugal distribution; lymphadenopathy is pathognomonic differentiator from smallpox; PCR confirmation required[1, 3-4]
- Disseminated Herpes Simplex Grouped vesicles on erythematous base; may be widespread in immunocompromised; Tzanck smear/PCR positive for HSV[1]
- Disseminated Herpes Zoster Dermatomal distribution initially; may disseminate in immunocompromised; VZV PCR positive[1]
- Hemorrhagic Smallpox Mimics Meningococcemia, acute leukemia, DIC — hemorrhagic smallpox was historically misdiagnosed as these conditions[2, 5]
- Drug Eruptions / Erythema Multiforme Medication history; target lesions in EM; Stevens-Johnson syndrome may mimic[1]
- Secondary Syphilis Painless rash including palms/soles; RPR/VDRL positive; sexual history[1, 4]
- Generalized Vaccinia History of recent smallpox vaccination; widespread vaccinia lesions[1, 6]
9. Past Medical History
- Prior smallpox vaccination: Determines risk of modified vs. ordinary disease; vaccination scars (typically deltoid) may be present in individuals born before ~1972 (US)[2][5]
- Immunodeficiency: HIV/AIDS, organ transplant, active chemotherapy — impacts disease severity and treatment response[10]
- Eczema/atopic dermatitis: Historically associated with eczema vaccinatum from vaccination; relevant if vaccination is being considered[3]
- Cardiac history: ACAM2000 vaccine carries risk of myopericarditis (~5.7 per 1000 vaccinees)[3]
- Pregnancy: Contraindication to live vaccines (ACAM2000); JYNNEOS (MVA-based, non-replicating) may be considered[3][15]
10. Physical Exam
- Vital signs: High fever (38.9–40.6°C) during prodrome; tachycardia; hypotension in severe/hemorrhagic cases[2][5]
- Skin: Deep-seated, firm, round, well-circumscribed vesicles/pustules; all lesions in same stage on any body region; centrifugal distribution; check palms and soles[5]
- Oral cavity: Enanthem on tongue, buccal mucosa, oropharynx — appears ~24 hours before exanthem[2][5]
- Eyes: Assess for keratitis, conjunctival lesions[2]
- Lymph nodes: Absence of significant lymphadenopathy (present = think mpox)[5-6]
- Respiratory: Auscultate for pneumonia signs
- Neurologic: Mental status, signs of encephalitis or meningismus[6]
- Hemorrhagic variant: Petechiae, purpura, ecchymoses, mucosal bleeding[1][8]
11. Lab Studies
- Definitive diagnosis requires BSL-4 laboratory confirmation — do NOT send to routine hospital labs[1-2][5]
- Specimen collection: Vesicular/pustular fluid (open with blunt scalpel, swab), scab scrapings, blood, tonsillar swabs; collector should ideally be recently vaccinated and wear full PPE[1-2]
- PCR: Real-time PCR for orthopoxvirus DNA and variola-specific sequences — most rapid and specific[2][5]
- Electron microscopy: Identifies characteristic brick-shaped orthopoxvirus virions (cannot distinguish variola from other orthopoxviruses)[1-2]
- Viral culture: Growth on cell lines or chorioallantoic membrane — confirmatory but slower[1-2]
- Serology: Does not differentiate among orthopoxvirus species; paired sera needed; IgM may enhance early diagnosis[2][5]
- Routine labs: CBC, CMP, coagulation studies for supportive care; blood cultures if secondary bacterial infection suspected
- Rule-out testing: VZV PCR, HSV PCR to exclude varicella and herpes in moderate-risk cases before pursuing variola testing[5]
12. Imaging
- Chest X-ray: Indicated if respiratory symptoms develop; assess for bronchopneumonia (more common in severe/confluent disease)[2]
- No pathognomonic imaging findings for smallpox itself
- Imaging is primarily supportive — to evaluate complications (pneumonia, ARDS)
- Routine imaging is unnecessary in uncomplicated cases
13. Special Tests
- CDC Smallpox Evaluation Algorithm (Major and Minor Criteria):[5]
Major criteria (any present raises suspicion)
- Febrile prodrome (≥38.3°C) with prostration, headache, backache, chills, vomiting, or severe abdominal pain, occurring 1–4 days before rash
- Classic smallpox lesions: deep-seated, firm, round, well-circumscribed vesicles/pustules; may become umbilicated or confluent
- Lesions in same stage of development on any one body part
- Minor criteria include: centrifugal distribution, first lesions on face/oral mucosa, patient appears toxic/moribund, slow evolution of lesions (each stage lasting 1–2 days), and lesions on palms/soles.
- Point-of-care: ABICAP immunofiltration assay can produce results in ~45 minutes[16]
- Skin biopsy: Histopathology shows intraepidermal multilocular vesicles with ballooning degeneration and cell necrosis[2]
- Tzanck smear: Useful to rule out herpes (multinucleated giant cells) but does not confirm smallpox
14. ECG
- Not a primary diagnostic tool for smallpox
ECG indicated if
- Hemodynamic instability or shock (hemorrhagic smallpox) — assess for myocarditis or ischemia
- Post-vaccination with ACAM2000 — monitor for myopericarditis (ST changes, PR depression, new arrhythmias)[3]
- Sepsis from secondary bacterial infection
15. Assessment
Clinical Classification (WHO)
- Ordinary smallpox (~90% of cases): Classic pustular rash; CFR ~30% unvaccinated (10% discrete, 50–60% confluent)
- Modified smallpox: Milder, accelerated course in previously vaccinated; rarely fatal
- Variola sine eruptione: Fever without rash; occurs in vaccinated contacts or infants with maternal antibodies; does not transmit
- Flat (malignant) smallpox (~7%): Soft, flat, confluent lesions; CFR 94–97%
- Hemorrhagic smallpox (~2–3%): Petechiae, hemorrhages, DIC-like picture; CFR ~98%; death by day 5–6; not reduced by prior vaccination
- Complications: Pockmark scarring (65–80% of survivors), blindness from keratitis (~1%), arthritis/osteomyelitis (2–5% of children), encephalitis (<1%), bronchopneumonia, secondary bacterial sepsis[2][6]
16. Treatment Plan
Immediate Actions
- Isolate the patient immediately — airborne + contact precautions; negative pressure room if available[1-3]
- Notify public health authorities — state health department → CDC (770-488-7100, 24/7) → WHO[2]
- Supportive care is the mainstay: IV fluids, antipyretics, pain management, nutritional support[1][16]
Antiviral Therapy
- Tecovirimat (TPOXX) — initiate as soon as possible; 14-day course; weight-based dosing as above[10]
- Consider cidofovir or brincidofovir if tecovirimat unavailable or resistance suspected[15]
- VIGIV for vaccine-related complications[3][15]
Vaccination of Contacts
- Ring vaccination strategy: Vaccinate all household and face-to-face contacts within 2–3 days of exposure (up to 4 days may still attenuate disease)[1-3]
- ACAM2000: Live vaccinia vaccine; single percutaneous dose; contraindicated in severe immunosuppression, eczema, pregnancy[3]
- JYNNEOS (MVA-BN): Non-replicating; safer for immunocompromised and pregnant patients; stockpiled for emergency use[14-15]
Secondary Infection Management
- Antibiotics for documented bacterial superinfection of skin lesions or pneumonia[16]
17. Disposition
- A single case of smallpox is a global public health emergency[2][4]
- Isolation is mandatory for all confirmed or suspected cases[1][3]
- Home isolation preferred when feasible to reduce nosocomial spread; hospital admission reserved for severe disease (hemorrhagic, flat, respiratory compromise, encephalitis)[1]
- Admission criteria: Hemodynamic instability, hemorrhagic or flat-type disease, respiratory failure, encephalitis, inability to maintain hydration, pregnancy with severe disease
- All healthcare workers must use airborne + contact precautions regardless of vaccination status[2-3]
- Specialist consultation: Infectious disease, public health/epidemiology, dermatology; critical care for severe cases
- Law enforcement/bioterrorism response should be activated concurrently[1]
18. Follow Up / Return Precautions
- Infectiousness persists from rash onset until all scabs have separated (typically 3–4 weeks)[1][3]
- Contacts under surveillance: Monitor for fever and rash for 17 days after last exposure[1]
- Survivors: Expect pockmark scarring in 65–80%; ophthalmologic follow-up for keratitis/blindness risk; orthopedic follow-up for children with arthritis[2]
- Lifelong immunity is conferred after natural infection[2]
- Return precautions for contacts: Seek immediate medical attention for any fever ≥38.3°C, rash, or constitutional symptoms during the surveillance period
- Psychological support: Significant morbidity from disfigurement; PTSD considerations in bioterrorism context
References
1. Smallpox as a Biological Weapon: Medical and Public Health Management. — Henderson DA, Inglesby TV, Bartlett JG, et al. The Journal of the American Medical Association. 1999.
2. Diagnosis and Management of Smallpox. — Breman JG, Henderson DA. The New England Journal of Medicine. 2002.
3. Clinical Management of Potential Bioterrorism-Related Conditions. — Adalja AA, Toner E, Inglesby TV. The New England Journal of Medicine. 2015.
4. Oral Tecovirimat for the Treatment of Smallpox. — Grosenbach DW, Honeychurch K, Rose EA, et al. The New England Journal of Medicine. 2018.
5. Smallpox. — Moore ZS, Seward JF, Lane JM. Lancet. 2006.
6. Neurologic Complications of Smallpox and Monkeypox: A Review. — Billioux BJ, Mbaya OT, Sejvar J, Nath A. JAMA Neurology. 2022.
7. Monkeypox: An international epidemic. — Focosi D, Novazzi F, Baj A, Maggi F. Reviews in Medical Virology. 2022.
8. Pandemic potential of poxviruses: From an ancient killer causing smallpox to the surge of monkeypox. — Brüssow H. Microbial Biotechnology. 2023.
9. FDA Orange Book. — FDA Orange Book. 2026.
10. FDA Drug Label. — Updated date: 2025-12-31. Food and Drug Administration.
11. Overview of the Regulatory Approval of Tecovirimat Intravenous Formulation for Treatment of Smallpox: Potential Impact on Smallpox Outbreak Response Capabilities, and Future Tecovirimat Development Potential. — Russo AT, Grosenbach DW, Honeychurch KM, Long PG, Hruby DE. Expert Review of Anti-Infective Therapy. 2023.
12. Tecovirimat: A Journey From Discovery to Mechanistic Insights in Poxvirus Inhibition. — Li X, Pan Z, Zhang L. PLoS Pathogens. 2025.
13. An Update on Mpox: Focussing on Current and Emerging Antiviral Strategies. — Hou Y, Su Y, Li J, Ding J. Reviews in Medical Virology. 2026.
14. Guidelines for the Prevention and Treatment of Opportunistic Infections in Children With and Exposed to HIV. — Bill G. Kapogiannis, Franklin Yates, Wei Li, et al Office of AIDS Research Advisory Council (2025). 2025.
15. Treatment and Vaccination for Smallpox and Monkeypox. — Saalbach KP. Advances in Experimental Medicine and Biology. 2024.
16. Confronting the Threat of Bioterrorism: Realities, Challenges, and Defensive Strategies. — Green MS, LeDuc J, Cohen D, Franz DR. The Lancet. Infectious Diseases. 2019.
17. Mpox—A Rapidly Evolving Disease. — Cowen EW, Tkaczyk ER, Norton SA, Leslie KS. JAMA Dermatology. 2023.