Smoke Inhalation Injury
Smoke inhalation injury is a three-component insult — supraglottic thermal injury, tracheobronchial chemical injury, and systemic toxicity (carbon monoxide and cyanide) — and is an independent pred…
Smoke inhalation injury is a three-component insult — supraglottic thermal injury, tracheobronchial chemical injury, and systemic toxicity (carbon monoxide and cyanide) — and is an independent predictor of mortality in fire victims, capable of doubling mortality when combined with cutaneous burns.[1] Approximately 15% of burn patients have concomitant inhalation injury, and 20–30% of severe burns are associated with it.[2-3]
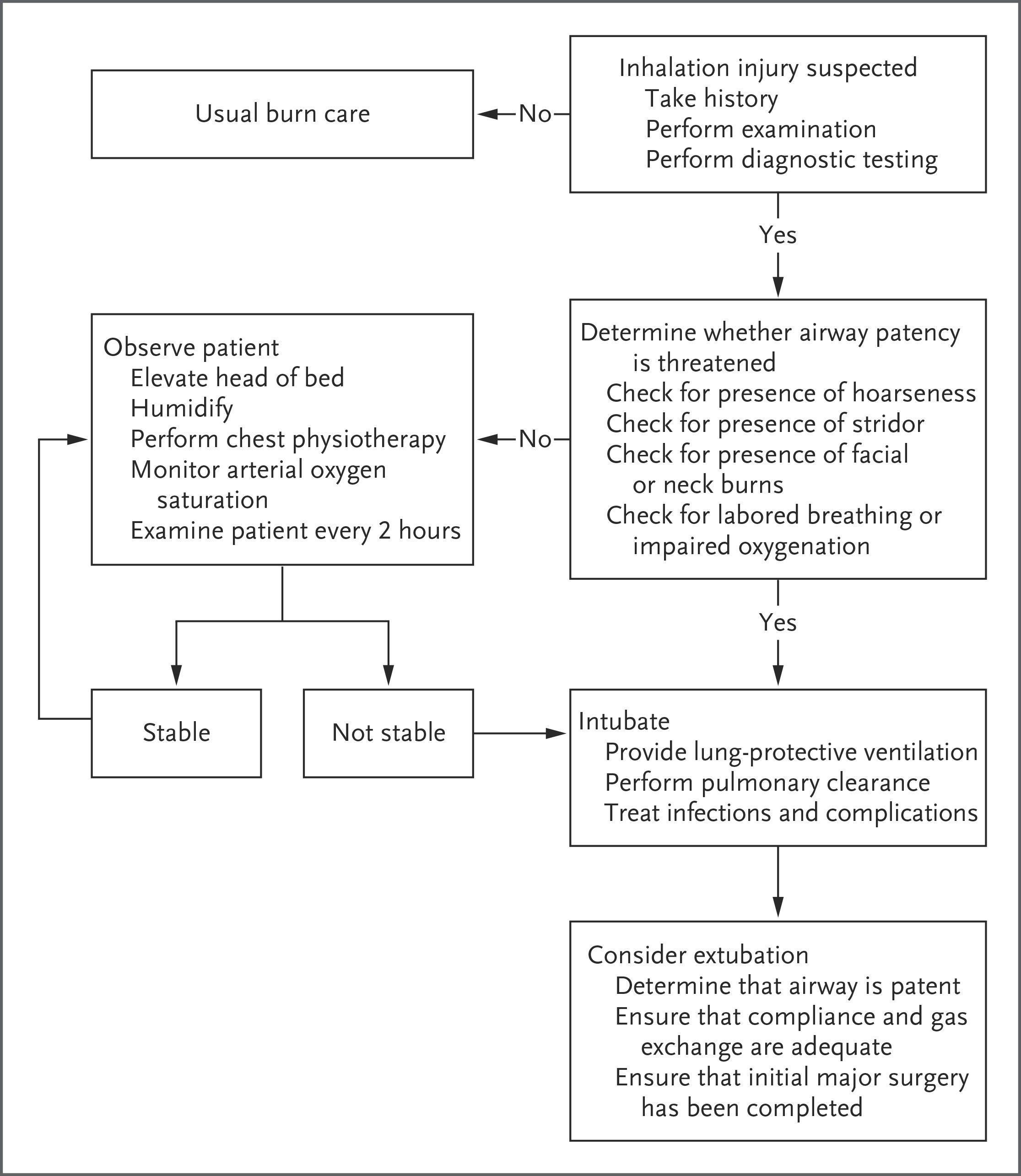
The following algorithm from Sheridan's NEJM review outlines the early management decision framework:
View full figure Figure 2. An Algorithm for Early Management of Fire-Related Inhalation Injury. Fire-Related Inhalation Injury. N Engl J Med. August 3, 2016.
1. History
- Exposure context: Enclosed vs. open space, duration of exposure, type of materials burning (plastics, synthetics, wood — nitrogen-containing products release cyanide)[5-6]
- Symptom characterization: Cough, hoarseness, dyspnea, throat tightness, chest tightness, wheezing
- Timing: Symptoms may be delayed up to 24–48 hours for lower airway and parenchymal injury; upper airway edema typically worsens over the first 12–24 hours, especially with concurrent fluid resuscitation[3][7]
- Associated symptoms: Headache, confusion, nausea, syncope (suggest CO/cyanide toxicity); facial/oral burns, singed hair[4-5]
- Important negatives: Loss of consciousness at scene (suggests significant CO/cyanide exposure), seizures, chest pain, hemoptysis
2. Alarm Features
- Stridor, progressive hoarseness, drooling — impending airway obstruction; intubate early as upper-airway edema makes reintubation extremely difficult[3-4]
- Altered mental status, syncope, or GCS <10 — suspect significant CO and/or cyanide poisoning[8-9]
- Persistent lactic acidosis (lactate >10 mmol/L) despite hemodynamic normalization — strongly associated with cyanide toxicity[4][8]
- COHb >30–40% — severe CO exposure[1]
- Extensive facial/neck burns or >20% TBSA cutaneous burns — anticipate progressive airway edema with resuscitation; low threshold for intubation[3-4]
- Cardiac arrest at scene — high suspicion for cyanide co-poisoning[9]
- Cyanosis, severe hypoxemia, respiratory failure
3. Medications
Treatments
- 100% high-flow O₂ via NRB mask — first-line for all smoke inhalation; reduces COHb half-life from 3–4 hours to <1 hour[1][4]
- Nebulized beta-agonists (albuterol) — for bronchospasm[2][4]
- Nebulized racemic epinephrine — for severe mucosal edema[2]
- Nebulized heparin (5,000–10,000 IU q2–4h) alternating with nebulized N-acetylcysteine (20%, 3 mL q2–4h) — for fibrin cast prevention and mucus clearance; supported by limited evidence[10-11]
- Hydroxocobalamin (5 g IV in adults) — first-line antidote for suspected cyanide poisoning; preferred over sodium nitrite in smoke inhalation because it does not reduce oxygen-carrying capacity[6][12]
Contraindicated/Not recommended
- Prophylactic antibiotics — not recommended[2][4][13]
- Empirical corticosteroids — associated with increased mortality and pneumonia in burn patients; contraindicated[2][4][13]
- Sodium nitrite — avoid in concurrent CO poisoning (induces methemoglobin, further reducing O₂ carrying capacity)[6]
4. Diet
- NPO initially if airway intervention is anticipated
- Early enteral nutrition is a priority in admitted burn/inhalation injury patients to support the hypermetabolic response
- Adequate hydration is critical, but fluid resuscitation must be carefully titrated (over-resuscitation worsens pulmonary edema)
5. Review of Systems
- Respiratory: Cough, dyspnea, wheezing, stridor, sputum production (carbonaceous?), hemoptysis
- Neurologic: Headache, confusion, dizziness, syncope, seizures (CO/cyanide)
- Cardiovascular: Chest pain, palpitations (CO-induced cardiac ischemia at COHb 30–50%)[4]
- GI: Nausea, vomiting (CO toxicity)
- Ophthalmologic: Eye irritation, corneal injury from chemical irritants
- Dermatologic: Facial burns, singed nasal/facial hair, soot deposits
6. Collateral History and Family History
- Bystander/EMS information is critical: Was the patient in an enclosed space? Duration of exposure? Loss of consciousness? Materials burning?
- Prehospital O₂ administration — COHb levels drop rapidly with O₂; a "normal" level on arrival may mask severe exposure[1][4]
- Pre-existing pulmonary disease (COPD, asthma) — increases vulnerability to bronchospasm and respiratory failure
- Pregnancy — fetal hemoglobin binds CO 2.5–3× more avidly than maternal hemoglobin; stronger indication for aggressive treatment and consideration of hyperbaric O₂[14]
- Family history is generally less relevant acutely
7. Risk Factors
- Enclosed-space exposure — the single most important risk factor[1][5]
- Prolonged exposure duration
- Combustion of synthetic materials (plastics, vinyl, wool, silk) — higher cyanide and toxic gas yield[6]
- Concurrent cutaneous burns — lung damage is much more severe when combined with major body-surface burns[1]
- Extremes of age — children and elderly have worse outcomes
- Pre-existing cardiopulmonary disease
- Altered consciousness at time of exposure (intoxication, disability) — prolongs exposure
8. Differential Diagnosis
- Thermal upper airway injury without chemical inhalation (flash burns from propane/butane — typically no smoke inhalation injury)[1]
- Acute asthma/COPD exacerbation triggered by irritant exposure
- Anaphylaxis — if acute airway edema and bronchospasm without clear exposure history
- Foreign body aspiration
- Toxic gas exposure without fire (CO from furnace, industrial cyanide)
- Acute epiglottitis — if isolated supraglottic edema
- Pulmonary contusion — if concurrent blast/trauma
- ARDS from other causes (aspiration, sepsis)
9. Past Medical History
- Asthma/COPD — lower threshold for bronchospasm, higher risk of respiratory failure
- Coronary artery disease — CO-induced cardiac ischemia occurs at COHb 30–50%[4]
- Prior intubation/tracheostomy — may complicate airway management (subglottic stenosis)
- Smoking history — baseline elevated COHb (3–10%)
- Pregnancy — see above
10. Physical Exam
Vital signs
- Tachypnea, tachycardia, hypotension (late/ominous), hypoxemia (SpO₂ unreliable — falsely normal with CO poisoning)[1]
Focused exam
- Airway: Facial/oral burns, singed nasal vibrissae, soot in nares/oropharynx, oropharyngeal edema/erythema, hoarseness, stridor[4-5]
- Lungs: Wheezing, rales, rhonchi; may be initially clear despite significant injury[15]
- Skin: Extent and depth of cutaneous burns, circumferential chest/neck burns (risk of compartment syndrome)
- Neuro: GCS, confusion, agitation, obtundation (CO/cyanide)
- Eyes: Conjunctival injection, corneal injury
- Pearl: A normal initial lung exam does not exclude significant inhalation injury — deterioration over 24–48 hours is common.[3][15]
11. Lab Studies
- Co-oximetry (COHb level) — the only accurate test for CO; standard pulse oximetry and ABG PaO₂ are unreliable[1]
- COHb 10–20%: headache, nausea
- COHb 20–30%: weakness, impaired cognition
- COHb >30–40%: severe exposure, cardiac ischemia, unconsciousness[4]
- Arterial blood gas — assess PaO₂/FiO₂ ratio (reliable indicator of injury severity and predictor of respiratory failure)[5][16]
- Lactate — elevated levels suggest tissue hypoxia; >10 mmol/L strongly associated with cyanide toxicity[8-9]
- CBC — baseline; leukocytosis expected
- BMP/CMP — renal function, electrolytes, anion gap metabolic acidosis
- Troponin — if cardiac ischemia suspected (CO-mediated)
- Cyanide levels — not available in real-time in most EDs; treatment is empirical[6][17]
12. Imaging
- Chest X-ray — often normal initially; may show diffuse infiltrates, atelectasis, or pulmonary edema as injury evolves[4]
- Chest CT — more sensitive for distal airway disease and pulmonary opacification; when combined with bronchoscopy, significantly improves prognostication[5]
- Imaging is not required for diagnosis — clinical evaluation and bronchoscopy are the principal diagnostic tools[4]
- Serial CXR useful for monitoring progression to ARDS/pneumonia
13. Special Tests
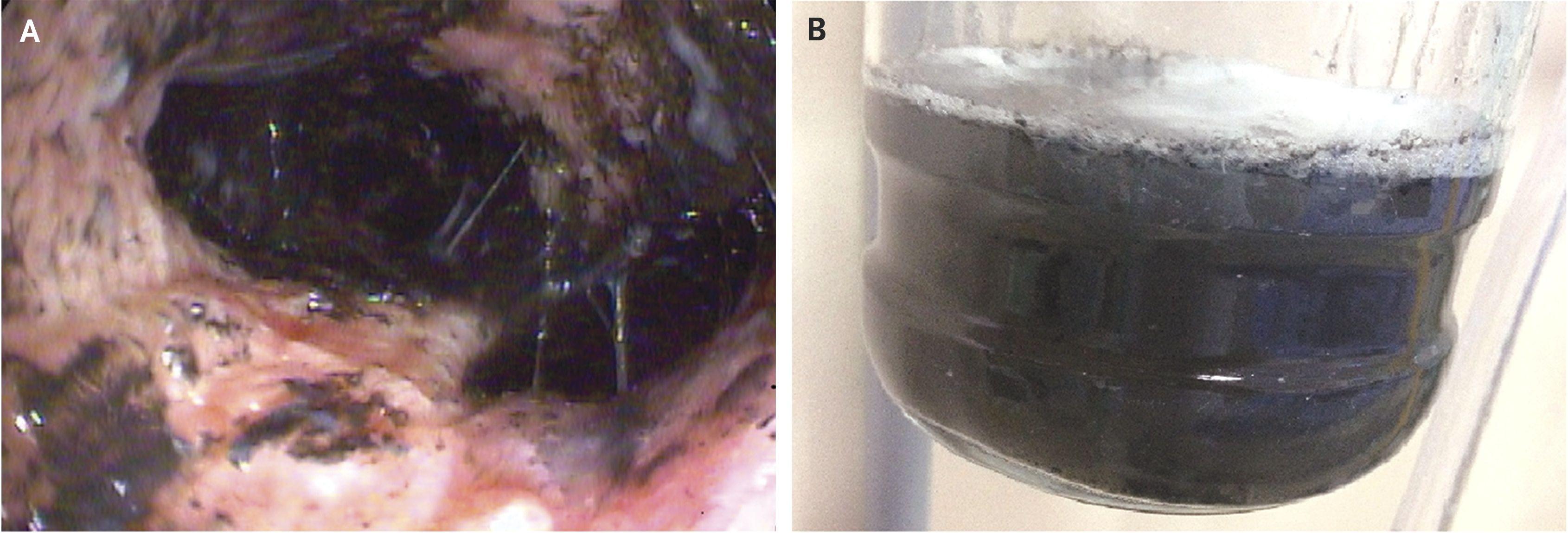
- Fiberoptic bronchoscopy — gold standard for diagnosis and grading of inhalation injury below the vocal cords; 86% accuracy with no false positives[5][18]
- Findings: mucosal edema, erythema, soot deposition, carbonaceous material, ulceration, necrosis, cast formation[15][19]
- Abbreviated Injury Score (AIS) is the most widely used grading system; grades 3–4 associated with higher pneumonia and ARDS risk[18]
- Also therapeutic: suctioning of debris and casts[11]
- Nasolaryngoscopy — for supraglottic assessment; can guide intubation decisions[3][12]
- PaO₂/FiO₂ ratio — correlates with injury severity and predicts mortality[5][16]
14. ECG
- Obtain ECG in all patients with significant CO exposure
- CO-induced myocardial ischemia: ST changes, arrhythmias (at COHb >30%)[4]
- Cyanide toxicity: bradycardia progressing to asystole, wide-complex arrhythmias
- Continuous cardiac monitoring for all moderate-to-severe exposures
15. Assessment
Three zones of injury
- Supraglottic (thermal) — direct heat injury causing edema of oropharynx, larynx; peaks at 12–24 hours; risk of complete obstruction[5][11]
- Tracheobronchial (chemical) — toxic particles (5–10 µm) penetrate lower airways causing epithelial necrosis, sloughing, fibrin cast formation, bronchospasm, and small-airway obstruction[1][15]
- Systemic (toxicologic) — CO and cyanide impair oxygen delivery and cellular respiration[4][8]
- Severity stratification: Combination of TBSA, age, and PaO₂/FiO₂ ratio is highly predictive of mortality.[16] Inhalation injury adds approximately 20% mortality at the LA₅₀ for burn area; pneumonia (develops in two-thirds by day 7–8) adds up to 60% additional mortality.[5]
Complications to anticipate
- Progressive airway obstruction (first 24–72 hours)
- Pneumonia (most common complication; two-thirds of intubated patients)[5]
- ARDS[1][5]
- Subglottic stenosis (long-term)[3]
- Delayed neurologic sequelae from CO (small percentage)[4]
16. Treatment Plan
Initial stabilization (0–72 hours)
- 100% O₂ via NRB for all patients; continue for minimum 6 hours if CO suspected[1][4]
- Airway management: Intubate for facial edema, hoarseness, stridor, GCS depression, or large cutaneous burns (>20% TBSA); secure ETT meticulously — reintubation is extremely difficult with upper-airway edema[3-4]
- Head of bed elevation, humidified air for non-intubated patients[4]
Bronchospasm
- Nebulized albuterol; racemic epinephrine for severe mucosal edema[2]
Airway clearance
- Nebulized heparin (5,000–10,000 IU) alternating with nebulized NAC (20%, 3 mL) q2–4h — reduces fibrin cast formation[10-11]
- Serial bronchoscopy for cast removal and airway toilet[11][19]
Systemic toxicity
- CO poisoning: 100% normobaric O₂ (standard); hyperbaric O₂ may be considered if no wheezing/airway debris and no cutaneous burns, though evidence is controversial[1][4]
- Cyanide poisoning: Hydroxocobalamin 5 g IV empirically if cardiac arrest at scene, GCS <10, lactate >10, or COHb >10% with enclosed-space exposure[6][9]
Mechanical ventilation (if needed)
- Lung-protective strategy: Vt ~6 mL/kg IBW, plateau pressure limits, adequate PEEP[1][20]
- High-frequency percussive ventilation is an option under investigation[12]
- The presence of inhalation injury does not mandate intubation. If airway patency is not threatened, particularly if cutaneous burns involve less than 20% of the body-surface area, elevation of the head of the bed, humidification of the air, and close observation are appropriate.
- — Robert L. Sheridan, M.D., Shriners Hospital for Children and other institutions
- Fire-Related Inhalation Injury. N Engl J Med. August 3, 2016.
17. Disposition
Admit/ICU criteria
- Any confirmed or suspected inhalation injury with respiratory symptoms
- Intubated patients
- COHb >25% or any neurologic symptoms
- Suspected cyanide toxicity
- Concurrent significant cutaneous burns (>20% TBSA)
- Patients requiring observation for progressive airway edema
Burn center transfer criteria
- Inhalation injury is an ABA burn center referral criterion regardless of burn size
- Combined inhalation injury + cutaneous burns
Observation (minimum 4–6 hours)
- Asymptomatic patients with minor exposure and normal COHb may be observed with serial reassessments every 2 hours and discharged if stable[4]
Discharge criteria
- Asymptomatic after observation period, normal COHb, no airway concerns, reliable follow-up
18. Follow Up / Return Precautions
- Follow-up within 24–48 hours for all discharged patients — delayed pulmonary edema can develop up to 48–72 hours post-exposure[7]
- Return immediately for: worsening cough, dyspnea, stridor, voice changes, chest pain, confusion, or any new neurologic symptoms
- Delayed neurologic sequelae from CO exposure (cognitive deficits, personality changes) may develop days to weeks later in a small percentage of patients[4]
- Long-term laryngologic follow-up — patients with inhalation injury are at risk for granulation tissue, vocal cord immobility, subglottic stenosis, and laryngeal scarring[3]
- Counsel on smoke detector installation and fire safety
References
1. Management of Burns. — Greenhalgh DG. The New England Journal of Medicine. 2019.
2. Burns in Children: Standard and New Treatments. — Jeschke MG, Herndon DN. Lancet. 2014.
3. Acute Upper Airway Obstruction. — Eskander A, de Almeida JR, Irish JC. The New England Journal of Medicine. 2019.
4. Fire-Related Inhalation Injury. — Sheridan RL. The New England Journal of Medicine. 2016.
5. Pathophysiology, Research Challenges, and Clinical Management of Smoke Inhalation Injury. — Enkhbaatar P, Pruitt BA, Suman O, et al. Lancet. 2016.
6. 2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Lavonas EJ, Akpunonu PD, Arens AM, et al. Circulation. 2023.
7. Hospital Treatment of Victims Exposed to Combustion Products. — Kulling P. Toxicology Letters. 1992.
8. Hazardous Chemical Emergencies and Poisonings. — Henretig FM, Kirk MA, McKay CA. The New England Journal of Medicine. 2019.
9. Impact of Protocol Development on Hydroxocobalamin Use for Smoke Inhalation Injury With Suspected Cyanide Toxicity: A Pre-Post Analysis. — Snodgrass K, Coffey R, Mandell SP, Faris J. Journal of Burn Care & Research : Official Publication of the American Burn Association. 2026.
10. Nebulized Heparin and N-Acetylcysteine for Smoke Inhalational Injury: A Case Report. — Ashraf U, Bajantri B, Roa-Gomez G, et al. Medicine. 2018.
11. Inhalation Injury in the Burned Patient. — Foncerrada G, Culnan DM, Capek KD, et al. Annals of Plastic Surgery. 2018.
12. Advances in Airway Management and Mechanical Ventilation in Inhalation Injury. — Gigengack RK, Cleffken BI, Loer SA. Current Opinion in Anaesthesiology. 2020.
13. The Diagnosis and Management of Inhalation Injury: An Evidence Based Approach. — Deutsch CJ, Tan A, Smailes S, Dziewulski P. Burns : Journal of the International Society for Burn Injuries. 2018.
14. Carbon Monoxide and Cyanide Poisoning in the Burned Pregnant Patient: An Indication for Hyperbaric Oxygen Therapy. — Culnan DM, Craft-Coffman B, Bitz GH, et al. Annals of Plastic Surgery. 2018.
15. Flexible Bronchoscopy for Assessing and Managing Smoke Inhalational Injury in a Teenager. — Wang G, Jing X, Gu H. Pediatric Pulmonology. 2025.
16. Assessing the Severity of Inhalation Injuries in Adults. — Hassan Z, Wong JK, Bush J, Bayat A, Dunn KW. Burns : Journal of the International Society for Burn Injuries. 2010.
17. Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Cao D, Arens AM, Chow SL, et al. Circulation. 2025.
18. Evaluating the Association Between Bronchoscopic Severity of Burns-Related Smoke Inhalation Injury and Clinical Outcomes: A Systematic Review and Meta-Analysis. — Amarasekera NN, Jha A, Charles WN, et al. Burns : Journal of the International Society for Burn Injuries. 2025.
19. Fire-Related Inhalation Injury. — Sheridan RL. The New England Journal of Medicine. 2016.
20. A Rationale for Safe Ventilation With Inhalation Injury: An Editorial Review. — Dries DJ, Perry JF, Tawfik PN. Journal of Burn Care & Research : Official Publication of the American Burn Association. 2022.