Spice Toxicity
Synthetic cannabinoids (SCs) — commonly known as "Spice," "K2," "Cloud 9," "Mojo," or "herbal incense" — are full agonists at CB1/CB2 receptors with binding affinities up to 100 times greater than…
Synthetic cannabinoids (SCs) — commonly known as "Spice," "K2," "Cloud 9," "Mojo," or "herbal incense" — are full agonists at CB1/CB2 receptors with binding affinities up to 100 times greater than THC, producing more severe and unpredictable toxicity than natural cannabis.[1-3] They are undetectable on routine urine drug screens.[4-5]
1. History
- Substance used: Ask specifically about "Spice," "K2," "herbal incense," "fake weed," or "research chemicals" — patients may not consider these "drugs"[3]
- Route: Most commonly smoked; also vaped, ingested as edibles, or absorbed via drug-impregnated paper strips (especially in correctional settings)[6-7]
- Timing of use, amount, and number of exposures
- Coingestants: Polysubstance use is common (~31% exposed to >1 substance); ask about opioids, benzodiazepines, alcohol, stimulants[8]
- Prior episodes of SC use and any previous adverse reactions
- Source of product (street purchase, internet, correctional facility)
- Important negatives: Deny access to anticoagulants, history of bleeding disorders, recent trauma
2. Alarm Features
- Coma/GCS ≤8 — associated with bradycardia and risk of cardiac arrest[6]
- Seizures — generalized tonic-clonic, may be refractory to benzodiazepines[4][9]
- Hyperthermia — rapidly life-threatening; exacerbated by physical restraints[10]
- Unexplained bleeding/coagulopathy — raises concern for brodifacoum (superwarfarin) contamination, which has caused multi-state outbreaks with INR >10, intracranial hemorrhage, and death[11-12]
- Acute respiratory failure — occurred in 60% of ICU-admitted patients in one series[4]
- Chest pain with ECG changes — myocardial infarction, including in patients with normal coronary arteries[1][10]
- Severe rhabdomyolysis with acute kidney injury[1][8]
3. Medications
Acute treatment
- Benzodiazepines (e.g., midazolam, lorazepam) — first-line for agitation, seizures, and sympathomimetic features[6][10]
- IV fluids — for dehydration, rhabdomyolysis, hypotension[1][6]
- Antiemetics (ondansetron) for nausea/vomiting[1]
- Atropine — for symptomatic bradycardia with hypotension; shown to improve hemodynamics and mental status[6]
- Vitamin K1 (phytonadione) — high-dose IV then oral for brodifacoum-contaminated products (e.g., 20 mg IV q8h initially, then 20 mg PO TID)[11-12]
Contraindicated/caution
- Antipsychotics (haloperidol, droperidol) — risk of QTc prolongation additive with SC-induced QTc prolongation[13]
- Physical restraints — may worsen hyperthermia and agitation; use only briefly if necessary[10]
- Withdrawal management: Benzodiazepines (diazepam) and quetiapine have shown symptom relief[14-15]
4. Diet
- NPO if altered mental status or risk of aspiration
- Aggressive IV hydration for rhabdomyolysis
- No specific dietary triggers; however, SC products are occasionally consumed as edibles ("cannabis gums")[7]
5. Review of Systems
- Neuropsychiatric: Agitation, hallucinations, paranoia, psychosis, suicidal ideation, coma, seizures, confusion[1][3][16]
- Cardiovascular: Chest pain, palpitations, syncope[3][17]
- GI: Nausea, vomiting, abdominal pain (hyperemesis syndrome reported)[1][3]
- Renal: Flank pain, decreased urine output, hematuria[3][8]
- Hematologic: Easy bruising, bleeding from any site (if brodifacoum-contaminated)[11]
- Respiratory: Dyspnea, cough[4]
6. Collateral History and Family History
- Collateral from bystanders, EMS, or law enforcement is critical — patients may be unable to provide history
- Ask companions about the specific product used and whether others are symptomatic (cluster presentations suggest contaminated batch)[11][18]
- Correctional facility staff may provide information about drug-impregnated paper strips[6]
- Family history of psychiatric illness, substance use disorders, or bleeding disorders
- Social context: Homelessness (13/30 ICU patients were undomiciled in one series), incarceration, populations subject to drug testing[3-4]
7. Risk Factors
- Demographics: Predominantly young males (20s–30s)[1][3][19]
- Polysubstance use[3][16]
- Homelessness and housing instability[4]
- Incarceration (SC undetectable on standard drug screens, driving use in correctional settings)[6]
- Psychiatric illness and personality disorders[4]
- Military personnel and athletes (evading drug testing)[3]
- Prior cannabis use (high-risk population for SC use)[14]
8. Differential Diagnosis
- Sympathomimetic toxidrome: Amphetamines, cathinones ("bath salts"), cocaine — similar agitation, tachycardia, hyperthermia[10]
- Anticholinergic toxidrome: Diphenhydramine, jimsonweed — mydriasis, dry skin, urinary retention, delirium
- Serotonin syndrome: Clonus, hyperreflexia, hyperthermia — medication history key
- Phencyclidine (PCP) intoxication: Nystagmus, violent behavior, analgesia
- Opioid intoxication: If presenting with CNS depression and bradycardia (newer SC compounds mimic this)[20]
- Primary psychiatric emergency: First-break psychosis, acute mania
- Superwarfarin/LAAR poisoning: If coagulopathy present — consider brodifacoum-contaminated SC[11][21]
- Meningitis/encephalitis: If fever and altered mental status
- Hypoglycemia, DKA, or other metabolic derangement
9. Past Medical History
- Prior SC or other substance use and adverse reactions
- Psychiatric history (schizophrenia, bipolar disorder — SC may precipitate psychosis)[4][22]
- Seizure disorder (SC lowers seizure threshold)[22]
- Cardiac history (arrhythmias, coronary artery disease)
- Renal disease (increased risk of AKI)
- Asthma/COPD (one death from ARDS in a patient with asthma history)[4]
- Bleeding disorders or anticoagulant use
10. Physical Exam
- Vitals: Tachycardia (37–77% of cases), hypertension; newer compounds may cause bradycardia (up to 24%) and hypotension (10%); hyperthermia; hypothermia (rare)[1][6][20]
- Neuro: GCS assessment, pupil size (mydriasis common), nystagmus, tremor, myoclonus, seizure activity, clonus
- Psych: Agitation level, psychosis, hallucinations, bizarre behavior, suicidality
- Cardiovascular: Rate, rhythm, murmurs; signs of heart failure
- Respiratory: Tachypnea, accessory muscle use, crackles (pulmonary infiltrates reported)[4]
- Skin: Diaphoresis, dry vs. moist, pallor, bruising/petechiae (if coagulopathy)
- Abdomen: Tenderness (flank pain with AKI or renal hemorrhage)
- Conjunctival injection[23]
11. Lab Studies
- Routine toxicology screen — will be negative for SC; useful to rule out coingestants[4-5]
- BMP/CMP: Glucose, electrolytes (hypokalemia characteristic), renal function (creatinine for AKI)[24]
- CBC: Anemia if bleeding
- CK/myoglobin: Rhabdomyolysis (26% of ICU patients)[4]
- Lactate: Metabolic acidosis assessment
- Hepatic panel: Liver injury
- Coagulation studies (PT/INR, aPTT): Critical — if INR elevated, suspect brodifacoum contamination[11-12]
- If coagulopathy present: Factor levels (II, VII, IX, X will be low), brodifacoum/superwarfarin panel[25]
- Troponin: If chest pain or ECG changes
- Urinalysis: Hematuria (most common bleeding symptom in brodifacoum contamination)[11]
- VBG/ABG: Respiratory and metabolic acidosis[7]
- Specialized SC testing: Liquid chromatography–tandem mass spectrometry (LC-MS/MS) can confirm specific SC compounds but is not widely available with rapid turnaround[5][9]
12. Imaging
- Chest X-ray: Diffuse pulmonary infiltrates, tree-in-bud pattern, diffuse alveolar hemorrhage reported[4]
- CT Head: If altered mental status, seizures, or suspected intracranial hemorrhage (especially with coagulopathy) — cerebral edema, loss of gray-white differentiation, intracranial bleeding[4][12]
- CT Abdomen/Pelvis: If abdominal/flank pain or hematuria — renal abnormalities, suburothelial hemorrhage (89% sensitivity for brodifacoum-associated coagulopathy), intramural bowel hematomas[11][26]
- Imaging is unnecessary in mild, self-limited presentations with normal vitals and mental status
13. Special Tests
- Superwarfarin/LAAR panel: Brodifacoum, bromadiolone, difenacoum — send if unexplained coagulopathy; results may take days[11][25]
- Point-of-care glucose: Immediate bedside assessment
- Bedside ultrasound: Cardiac function, IVC assessment, free fluid
- SC-specific immunoassay: Available at some centers with short turnaround for common compounds (AB-FUBINACA, 4F-MDMB-BUTINACA)[8]
- LC-HRMS (nontargeted): Gold standard for novel SC identification[9]
14. ECG
- QTc prolongation — documented in SC users; increased QT dispersion and P-wave dispersion indicating pro-arrhythmic risk[13][27]
- Sinus tachycardia (most common) or sinus bradycardia (newer full-agonist compounds)[1][20]
- ST changes: Ischemia, MI (vasospasm-mediated, even with normal coronaries)[5][10]
- Ventricular arrhythmias: VF, VT reported in cardiac arrest[10]
- hERG channel inhibition by SC compounds (e.g., 5F-AKB48) provides mechanistic basis for QT prolongation[28]
- Caution: Avoid QTc-prolonging medications (antipsychotics) in the setting of SC-induced QTc prolongation[13]
15. Assessment
- SC toxicity presents on a spectrum from mild to life-threatening. Most presentations involve young males with tachycardia, agitation, and nausea that resolve within <8 hours with supportive care.[1][19] However, severe complications include:
- Toxic encephalopathy (coma in 33% of ICU patients)[4]
- Acute respiratory failure (60% of ICU patients; 70% required intubation)[4]
- Seizures (20% of ICU patients)[4]
- Rhabdomyolysis and AKI[1][8]
- Myocardial infarction and stroke[1][5]
- Brodifacoum-associated coagulopathy — a distinct and potentially fatal complication requiring high-dose vitamin K for weeks to months[11-12]
- Newer-generation SC compounds (full CB1 agonists like INACA derivatives, XLR-11) may present atypically with CNS depression and bradycardia rather than the classic sympathomimetic picture.[6][20]
16. Treatment Plan
Initial stabilization
- ABCs; intubation for GCS ≤8 or respiratory failure (required in up to 70% of ICU patients)[4]
- Continuous cardiac monitoring, pulse oximetry, temperature monitoring
Agitation/seizures
- Benzodiazepines first-line: Midazolam 5–10 mg IM/IV or lorazepam 2–4 mg IV; repeat as needed[6][10]
- Refractory agitation/seizures → deeper sedation, consider propofol or barbiturates, and intubation[6]
Hemodynamic instability
- IV crystalloid bolus for hypotension
- Bradycardia with hypotension: Atropine 0.5–1 mg IV[6]
- Vasopressors if refractory
Hyperthermia
- Aggressive cooling (evaporative, ice packs)
- Benzodiazepines to reduce psychomotor activity[10]
Rhabdomyolysis
- Aggressive IV normal saline; target UOP 1–3 mL/kg/hr[6]
Brodifacoum-associated coagulopathy
- Vitamin K1 (phytonadione): 10–20 mg IV q8h initially, transition to 20 mg PO TID[11-12]
- FFP, 4-factor PCC, or packed RBCs as clinically indicated for active bleeding[11][18]
- Treatment duration: Weeks to months due to brodifacoum's half-life of 20–130 days[21][23]
Symptomatic care
- Antiemetics for nausea/vomiting
- Monitor and correct hypokalemia[24]
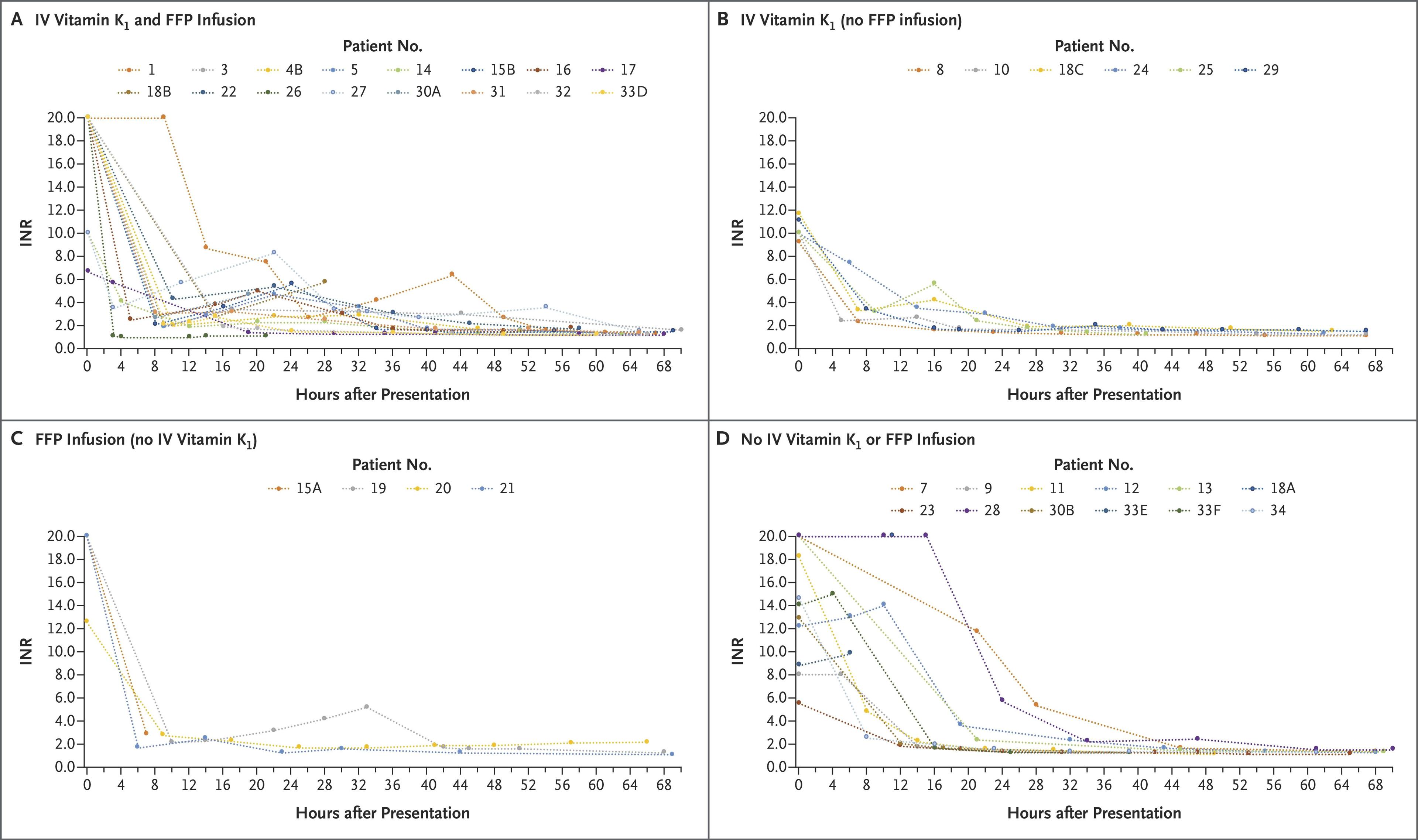
- The following figure from the Illinois outbreak demonstrates INR trajectories over 72 hours with various treatment combinations for brodifacoum-contaminated SC coagulopathy:
17. Disposition
- Discharge criteria: Mild symptoms (nausea, mild agitation) that resolve with observation, normal vitals, normal mental status, normal labs including INR; most mild cases resolve within 6–8 hours[1][19]
- Observation: Persistent mild symptoms, borderline vitals, awaiting lab results
Admission (telemetry/floor)
- Persistent tachycardia or bradycardia
- Abnormal labs (elevated CK, AKI, coagulopathy)
- Ongoing agitation requiring repeated benzodiazepine dosing
- 31% of patients in one series required hospital admission[8]
ICU admission
- Intubation for airway protection or respiratory failure
- Refractory seizures
- Hemodynamic instability requiring vasopressors or pacing
- Severe rhabdomyolysis
- Active hemorrhage with coagulopathy[4][20]
Specialist consultation triggers
- Toxicology/Poison Control — all moderate-severe cases
- Hematology — brodifacoum-associated coagulopathy
- Nephrology — AKI requiring dialysis
- Psychiatry — psychosis, suicidal ideation, first-break psychosis
- Neurosurgery — intracranial hemorrhage
- Note: 53% of ICU patients in one series left AMA; patients leaving AMA were 1.6× more likely to be rehospitalized[4][18]
18. Follow Up / Return Precautions
- Brodifacoum coagulopathy: Requires outpatient INR monitoring 2–3 times weekly initially, with vitamin K dose titration; treatment may be needed for months[11-12][21]
- Withdrawal syndrome: Onset within 1–2 days of cessation; symptoms include insomnia, irritability, low mood, drug craving, diaphoresis, nausea, tremor, hypertension, and tachycardia; more severe than cannabis withdrawal[29-30]
- Managed with benzodiazepines (diazepam) and quetiapine[14-15]
- Return precautions: Return immediately for any bleeding (blood in urine, stool, gums, nosebleeds), recurrent seizures, chest pain, confusion, inability to tolerate fluids, or worsening psychiatric symptoms
- Counseling: Emphasize that SC products are far more dangerous than natural cannabis, unpredictable in composition, and undetectable on standard drug screens[3-4]
- Referral: Substance use disorder treatment, harm reduction services
- Expected course: Most mild intoxications resolve fully within hours; severe cases may have prolonged recovery; chronic use may lead to persistent cognitive and psychiatric symptoms[31]
References
1. A Systematic Review of Adverse Events Arising From the Use of Synthetic Cannabinoids and Their Associated Treatment. — Tait RJ, Caldicott D, Mountain D, Hill SL, Lenton S. Clinical Toxicology. 2015.
2. Adverse Clinical Effects Associated With the Use of Synthetic Cannabinoids: A Systematic Review. — Prete MM, Feitosa GTB, Ribeiro MAT, Fidalgo TM, Sanchez ZM. Drug and Alcohol Dependence. 2025.
3. Synthetic Cannabinoids. — Mills B, Yepes A, Nugent K. The American Journal of the Medical Sciences. 2015.
4. Critical Illness Secondary to Synthetic Cannabinoid Ingestion. — Kourouni I, Mourad B, Khouli H, Shapiro JM, Mathew JP. JAMA Network Open. 2020.
5. Ischemic Stroke After Use of the Synthetic Marijuana "Spice". — Freeman MJ, Rose DZ, Myers MA, et al. Neurology. 2013.
6. Identification and Health Risks of an Emerging Means of Drug Use in Correctional Facilities. — Kuai D, Rivera Blanco LE, Krotulski A, et al. JAMA Network Open. 2024.
7. Clinical Features Associated With ADB-BUTINACA Exposure in Patients Attending Emergency Departments in England. — King A, Hill SL, Pucci M, et al. Clinical Toxicology. 2022.
8. Acute Intoxication Caused by Three Common Synthetic Cannabinoids: The Experience of a Large, Urban, Tertiary Care Hospital. — Shopan N, Scolnik D, Hassoun E, et al. The American Journal of Emergency Medicine. 2023.
9. Intoxication From the Novel Synthetic Cannabinoids AB-PINACA and ADB-PINACA: A Case Series and Review of the Literature. — Armenian P, Darracq M, Gevorkyan J, et al. Neuropharmacology. 2018.
10. 2023 American Heart Association Focused Update on the Management of Patients With Cardiac Arrest or Life-Threatening Toxicity Due to Poisoning: An Update to the American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Lavonas EJ, Akpunonu PD, Arens AM, et al. Circulation. 2023.
11. An Outbreak of Synthetic Cannabinoid–Associated Coagulopathy in Illinois. — Kelkar AH, Smith NA, Martial A, et al. The New England Journal of Medicine. 2018.
12. An Outbreak of Severe Coagulopathy in Northern Israel Among Users of Illicit Synthetic Cannabinoids Adulterated With Brodifacoum. — Lurie Y, Nadir Y, Hoffman R, et al. Clinical Toxicology. 2023.
13. Synthetic Cannabinoids and Their Effects on the Cardiovascular System. — Von Der Haar J, Talebi S, Ghobadi F, et al. The Journal of Emergency Medicine. 2016.
14. Adverse Effects of Synthetic Cannabinoids: Management of Acute Toxicity and Withdrawal. — Cooper ZD. Current Psychiatry Reports. 2016.
15. Synthetic Cannabinoid Withdrawal: A New Demand on Detoxification Services. — Macfarlane V, Christie G. Drug and Alcohol Review. 2015.
16. Acute Poisonings From Synthetic Cannabinoids - 50 U.S. Toxicology Investigators Consortium Registry Sites, 2010-2015. — Riederer AM, Campleman SL, Carlson RG, et al. MMWR. Morbidity and Mortality Weekly Report. 2016.
17. Synthetic Cannabinoids and Cathinones Cardiotoxicity: Facts and Perspectives. — Radaelli D, Manfredi A, Zanon M, et al. Current Neuropharmacology. 2021.
18. An Outbreak of Severe Coagulopathy From Synthetic Cannabinoids Tainted With Long-Acting Anticoagulant Rodenticides. — Devgun JM, Rasin A, Kim T, et al. Clinical Toxicology. 2020.
19. Evolution of Clinical Characteristics and Outcomes of Synthetic Cannabinoid Receptor Agonist Exposure in the United States: Analysis of National Poison Data System Data From 2010 to 2015. — Cordeiro SK, Daro RC, Seung H, Klein-Schwartz W, Kim HK. Addiction. 2018.
20. Retrospective Chart Review of Synthetic Cannabinoid Intoxication With Toxicologic Analysis. — Sud P, Gordon M, Tortora L, et al. The Western Journal of Emergency Medicine. 2018.
21. Bad Weed: Synthetic Cannabinoid-Associated Coagulopathy. — Arepally GM, Ortel TL. Blood. 2019.
22. Toxicity of Synthetic Cannabinoids in K2/Spice: A Systematic Review. — de Oliveira MC, Vides MC, Lassi DLS, et al. Brain Sciences. 2023.
23. Hemorrhagic Soft Tissue Upper Airway Obstruction From Brodifacoum-Contaminated Synthetic Cannabinoid. — Ross CH, Singh P, Simon EL. The Journal of Emergency Medicine. 2019.
24. Acute Toxicity Due to the Confirmed Consumption of Synthetic Cannabinoids: Clinical and Laboratory Findings. — Hermanns-Clausen M, Kneisel S, Szabo B, Auwärter V. Addiction. 2013.
25. Factor-Guided Diagnosis of Coagulopathy Associated With Coumarin-Contaminated Synthetic Cannabinoids. — Torian SC, Hayes L, Negrete A. The American Journal of Emergency Medicine. 2022.
26. Radiological Findings in Poisoning by Synthetic Cannabinoids Adulterated With Brodifacoum. — Bar N, Lopez-Alonso R, Merhav G, et al. European Radiology. 2024.
27. Electrocardiographic Alterations in Patients Consuming Synthetic Cannabinoids. — Ozturk HM, Erdogan M, Alsancak Y, et al. Journal of Psychopharmacology. 2018.
28. Noncanonical Pharmacological Inhibition of the hERG K+ Channel by a Synthetic Cannabinoid. — Cheng H, Upex C, Du C, et al. Biochemical Pharmacology. 2025.
29. Clinical Withdrawal Symptom Profile of Synthetic Cannabinoid Receptor Agonists and Comparison of Effects With High Potency Cannabis. — Craft S, Ferris JA, Barratt MJ, et al. Psychopharmacology. 2022.
30. Withdrawal Phenomena and Dependence Syndrome After the Consumption of "Spice Gold". — Zimmermann US, Winkelmann PR, Pilhatsch M, et al. Deutsches Arzteblatt International. 2009.
31. "": A Thematic Analysis of the Experience of an Addiction to Synthetic Cannabinoids. — Marandure BN, Mhizha S, Wilson A. Journal of Psychoactive Drugs. 2022.