Spinal Cord Compression
Spinal cord compression (SCC) is a neurologic emergency requiring rapid recognition and intervention to prevent irreversible paralysis. The four major causes are trauma, metastatic disease, epidura…
Spinal cord compression (SCC) is a neurologic emergency requiring rapid recognition and intervention to prevent irreversible paralysis. The four major causes are trauma, metastatic disease, epidural abscess, and epidural hematoma.[1] Back pain is the earliest and most common symptom, present in 83–95% of patients prior to diagnosis.[2-3] Pretreatment ambulatory status is the strongest predictor of functional outcome.[4-5]
1. History
- Pain characterization: Localized back/neck pain (most common initial symptom), radicular pain, or mechanical pain from vertebral collapse[2]
- Pain that is worse at night, when recumbent, and worsened by Valsalva maneuver is characteristic of epidural compression[2]
- Referred pain patterns: Cervical lesions → midscapular pain; thoracic lesions → hip/lumbosacral pain; lumbosacral lesions → thoracic pain[3]
- Timing: Median time from pain onset to MSCC diagnosis is ~2 months; progressive worsening is typical[2]
- Motor symptoms: "Heaviness" or "clumsiness" of limbs, difficulty walking, gait unsteadiness[2]
- Sensory symptoms: Numbness, paresthesias, ascending pattern
- Autonomic symptoms: Urinary hesitancy → retention → overflow incontinence; constipation; sexual dysfunction[3][6]
- Ask about: Known cancer history, recent infections, IV drug use, anticoagulant/antiplatelet use, recent spinal procedures, immunosuppression[1][7]
2. Alarm Features
- Rapidly progressive motor weakness — can deteriorate during workup[8]
- Bowel or bladder dysfunction (urinary retention with overflow incontinence is pathognomonic for cauda equina syndrome: 90% sensitivity, 95% specificity)[3]
- Saddle anesthesia — perineal/perianal sensory loss[6][9]
- Bilateral lower extremity weakness with upper motor neuron signs
- Fever + back pain + neurologic deficits → epidural abscess until proven otherwise[7]
- Spinal shock: Flaccid areflexic paralysis with systemic hypotension in acute severe compression[1]
- In 20% of patients, cancer first presents as spinal cord compression[3]
3. Medications
- Dexamethasone: Initiate immediately upon diagnosis. Minimum dose: 4 mg IV every 6 hours; dose may range from 10–100 mg. A randomized trial supports high-dose steroids (higher ambulation rates: 81% vs 63% at 3 months)[10-11]
- Alternative dosing: Loading dose of 10 mg IV followed by 4–6 mg maintenance every 4–6 hours[12]
- Standard dose for MSCC: 16 mg/day in divided doses, followed by taper[13]
- GI prophylaxis: H2 blocker or PPI for patients on steroids, especially if on NSAIDs, anticoagulants, or with GI risk factors[10]
- PJP prophylaxis: Consider for patients on dexamethasone ≥3 mg/day (equivalent prednisone 20 mg/day) for ≥4 weeks[11]
- Pain management: Opioids, NSAIDs (with caution), neuropathic agents as needed
- Contraindicated: Avoid steroids before biopsy in suspected CNS lymphoma (can obscure diagnosis)[10]
- Anticoagulants: If epidural hematoma is the cause, reverse anticoagulation immediately[1]
4. Diet
- NPO if surgical intervention is anticipated
- Adequate hydration to prevent steroid-related hyperglycemia complications
- High-fiber diet and stool softeners for patients with constipation from autonomic dysfunction or opioid use
- Long-term: Calcium and vitamin D supplementation if prolonged steroid use anticipated
5. Review of Systems
- Neurologic: Weakness (present in 35–75% at diagnosis), numbness, gait difficulty, hand clumsiness[2]
- GU: Urinary retention, hesitancy, incontinence, sexual dysfunction
- GI: Constipation, fecal incontinence, decreased anal tone
- Constitutional: Fever (suggests infection), weight loss, night sweats (suggests malignancy)
- MSK: Back/neck pain, spinal tenderness
- Vascular: Symptoms of DVT/PE (high VTE risk in SCI)[14]
6. Collateral History and Family History
- Cancer history: Type, stage, prior treatments, known metastatic sites — breast, lung, and prostate are the most common primaries causing MSCC[8][15]
- Infection history: Recent bacteremia, skin infections, endocarditis, spinal procedures[7]
- Substance use: IV drug use (risk factor for epidural abscess; LR+ 13.7)[16-17]
- Anticoagulation status: Warfarin, DOACs, antiplatelet agents (risk for epidural hematoma)[1]
- Functional baseline: Pre-morbid ambulatory status is critical for treatment planning and prognosis[4-5]
- Family history is generally less relevant unless hereditary cancer syndromes are suspected
7. Risk Factors
- Malignancy: Prostate, breast, lung cancer are the most common causes of MSCC; thoracic spine is most frequently affected (60%), followed by lumbosacral (30%) and cervical (10%)[3][15]
- IV drug use, diabetes, immunosuppression, renal failure → epidural abscess[1][17]
- Anticoagulation, coagulopathy, thrombocytopenia → epidural hematoma[1]
- Indwelling vascular catheters (LR+ 15.7 for epidural abscess)[16]
- Osteoporosis, trauma → pathologic/compression fractures
- Prior spinal surgery or procedures[17]
- Degenerative disc disease → large central disc herniation causing cauda equina syndrome[6]
8. Differential Diagnosis
- Metastatic epidural spinal cord compression — most common nontraumatic cause; progressive pain → weakness → sensory loss → sphincter dysfunction[2]
- Epidural abscess — fever + severe back pain + neurologic deficits; 4-phase progression (pain → radicular pain → neurologic changes → paralysis); S. aureus most common pathogen[7]
- Epidural hematoma — acute onset in setting of anticoagulation or coagulopathy[1]
- Cauda equina syndrome — saddle anesthesia, urinary retention, asymmetric lower extremity weakness[6][9]
- Transverse myelitis — inflammatory; noncompressive on MRI[18]
- Spinal cord infarction — hyperacute onset, anterior cord syndrome pattern[18]
- Degenerative cervical myelopathy — insidious onset, hand clumsiness, gait ataxia, upper motor neuron signs[19]
- Primary spinal cord tumors — ependymoma, astrocytoma; subacute presentation[18]
- Vertebral compression fracture without cord compression — mechanical pain without neurologic deficits
- Leptomeningeal disease — consider as alternative diagnosis per NCCN[10]
9. Past Medical History
- Known malignancy — type, stage, treatment history, prior radiation to spine
- Prior episodes of back pain or radiculopathy
- Previous spinal surgery or instrumentation
- Osteoporosis, prior fractures
- Diabetes, immunosuppression, chronic kidney disease (risk for abscess)
- Bleeding disorders, anticoagulant use
- History of DVT/PE (relevant for VTE prophylaxis planning)
10. Physical Exam
- Vital signs: Hypotension and bradycardia suggest neurogenic shock (lesions at T6 or above)[20-21]
- Spinal percussion: Tenderness over affected vertebra — can reveal metastatic disease or fracture; commonly omitted but highly informative[1]
- Motor exam: Symmetric weakness (UMN pattern above conus; LMN pattern in cauda equina); assess strength in all myotomes[1-2]
- Sensory exam: Identify a sensory level — circumferential boundary below which sensation is lost; check above the clavicles to avoid missing cervical cord compression[1]
- Reflexes: Hyperreflexia and Babinski sign (UMN lesion above conus); hyporeflexia/areflexia (cauda equina or spinal shock)[1][19]
- Hoffmann sign, clonus, inverted brachioradialis reflex — cervical myelopathy[19]
- Rectal exam: Anal sphincter tone (decreased in 20–80% of cauda equina syndrome)[3]
- Post-void residual: Absence of PVR virtually excludes cauda equina syndrome (99.99% NPV)[3]
- Gait assessment: Wide-based ataxic gait in myelopathy[19]
11. Lab Studies
- CBC: Leukocytosis (infection); anemia (malignancy)
- CMP: Renal function, calcium (hypercalcemia of malignancy), glucose (steroid monitoring)
- ESR/CRP: Elevated in epidural abscess; useful screening tool[7]
- Blood cultures: If infection suspected — positive in many cases of epidural abscess[7]
- Coagulation studies: PT/INR, PTT — if epidural hematoma suspected or anticoagulant use[1]
- PSA, tumor markers: If unknown primary malignancy
- Urinalysis: Post-void residual measurement for suspected cauda equina syndrome
- Glucose monitoring: Steroid-induced hyperglycemia
12. Imaging
- MRI of the entire spine with and without gadolinium — gold standard; sensitivity 0.44–0.93, specificity 0.90–0.98[4][22]
- Urgent MRI in the event of neurologic symptoms[10]
- 15–20% of patients have additional lesions at other levels — complete spine imaging is strongly recommended[10]
- T2-hyperintense intramedullary signal suggests acute cord edema — critical finding for surgical planning[23]
- CT myelogram — if MRI is contraindicated or unavailable[10]
- Survey spine MRI protocol (sagittal T2 + STIR): 79% faster than routine MRI; 14% positivity rate for cord compression in ED setting[24]
- CT spine: Can identify bony destruction, fractures, instability; not sufficient to evaluate cord compression alone
- Imaging is unnecessary when clinical presentation clearly excludes cord compression (e.g., isolated mechanical low back pain without red flags)
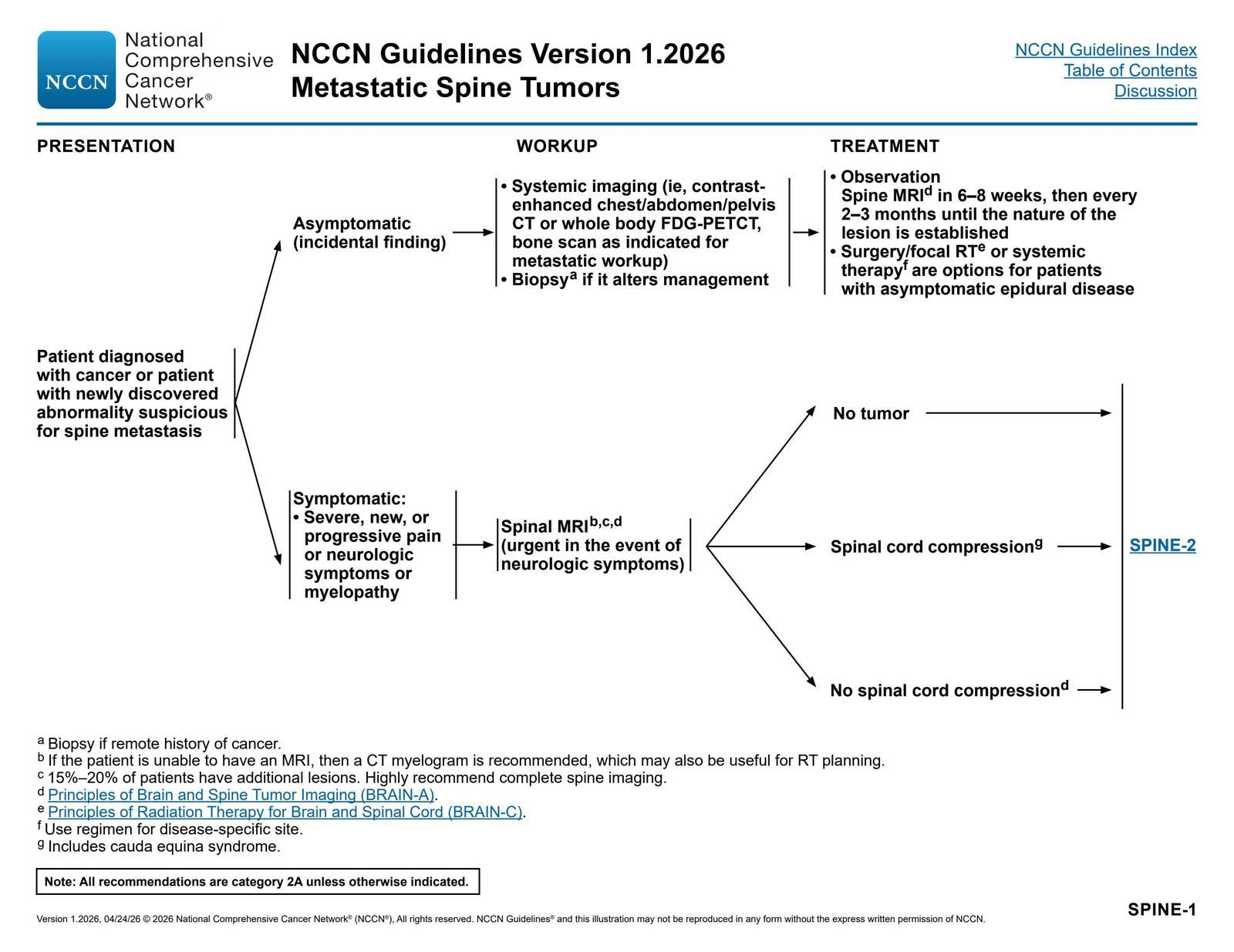
- The NCCN CNS Cancers Guidelines algorithm for metastatic spine tumor workup and treatment is shown below:
- SPINE-1. Metastatic Spine Tumors: Presentation, Workup, and Treatment — NCCN Guidelines® — Central Nervous System Cancers p. 84 (v1.2026) Central Nervous System Cancers. April 23, 2026.
- OpenEvidence has a License from NCCN to use the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Central Nervous System Cancers Version 1.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved.
13. Special Tests
- Spinal Instability Neoplastic Score (SINS): Evaluates spinal instability in metastatic disease — guides surgical vs. nonsurgical management[10]
- Frankel Grading System: Functional assessment scale (A = complete paraplegia through E = normal)[3]
- Bilsky Epidural Spinal Cord Compression Scale: Grades degree of epidural compression on MRI — guides need for separation surgery vs. SBRT[25]
- Post-void residual (PVR): Bedside bladder scan — critical for cauda equina evaluation[3][9]
- Digital rectal exam: Assess anal sphincter tone
- CT-guided biopsy: If no known primary malignancy or if histology would alter management[10]
14. ECG
- Sinus bradycardia is the most common dysrhythmia in acute SCI at T6 or above — universal in severe cervical cord injury[20-21]
- Other findings: ST-segment changes, T-wave inversions, QT prolongation, QRS prolongation, supraventricular arrhythmias[14][26]
- Primary cardiac arrest occurred in 16% of patients with severe cervical cord injury in one series[21]
- ECG abnormalities peak at day 4 post-injury and typically resolve within 2–6 weeks[21]
- Continuous cardiac monitoring is warranted for cervical and high thoracic (≥T6) cord compression[20][27]
- Must differentiate neurogenic ECG changes from primary cardiac pathology[14]
15. Assessment
- SCC is a time-sensitive neurologic emergency — neurologic function at the time of treatment is the strongest predictor of outcome[4-5]
- 50–68% of patients are unable to walk at the time of MSCC diagnosis[2]
- Thoracic spine is the most commonly affected region in metastatic disease[3][15]
- Severity stratification should consider: rate of neurologic decline, ambulatory status, number of compression levels, tumor histology (radiosensitive vs. radioresistant), spinal stability, and overall prognosis[8][10]
- Atypical presentations: Abdominal pain with constipation (thoracic cord lesion), isolated urinary retention, isolated gait difficulty[28-29]
- Complications: Permanent paralysis, chronic pain, DVT/PE, pressure ulcers, autonomic dysreflexia, respiratory failure (cervical lesions)
16. Treatment Plan
Initial Stabilization
- Spinal precautions/immobilization if instability suspected
- Dexamethasone: Start immediately upon diagnosis — minimum 4 mg IV q6h (range 10–100 mg); followed by oral taper[10-11]
- Hemodynamic support if neurogenic shock (IV fluids, vasopressors for MAP goals)
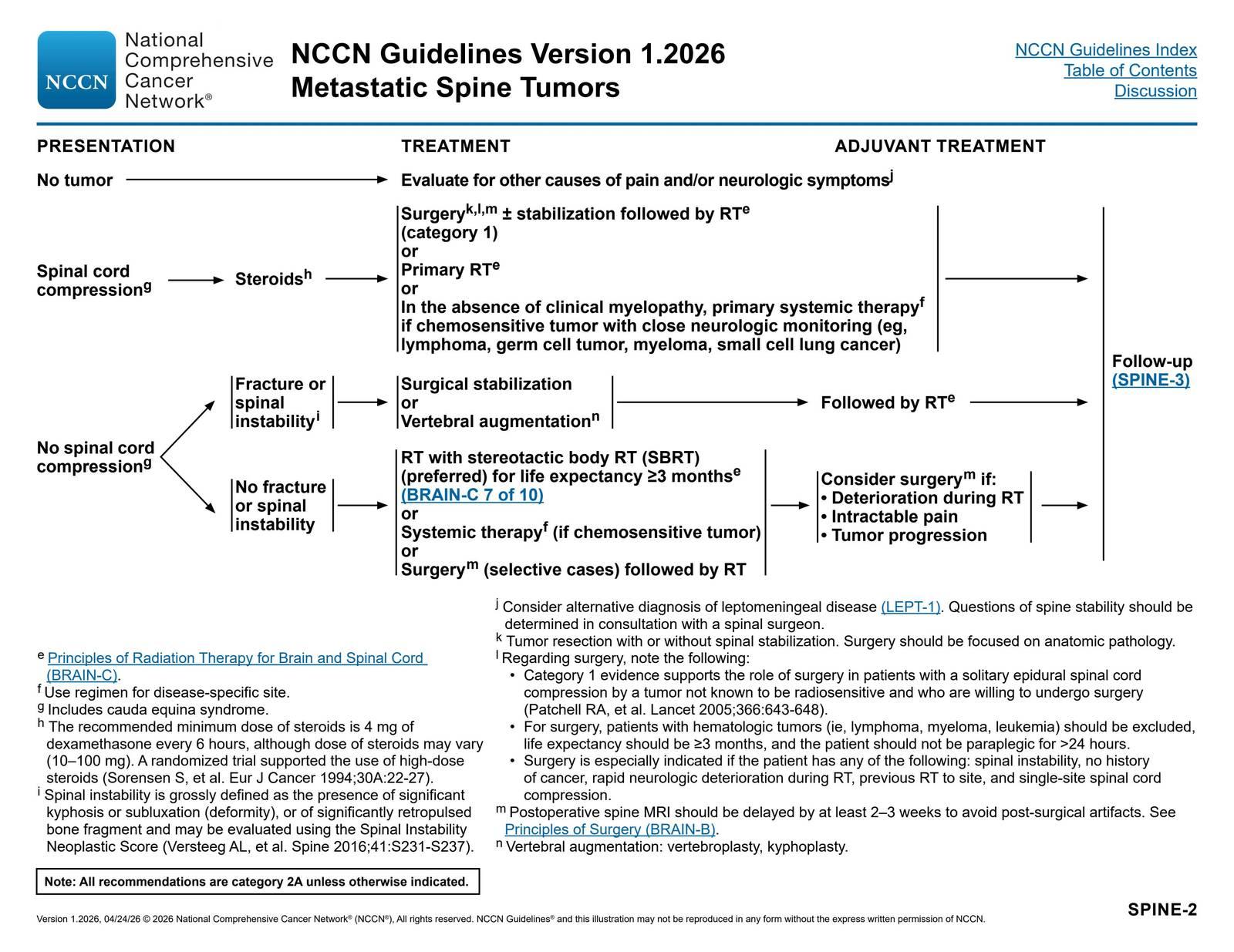
Definitive Treatment (Metastatic SCC) per NCCN Guidelines
- Surgery ± stabilization followed by RT — Category 1 evidence for solitary epidural compression by non-radiosensitive tumor (Patchell trial)[10]
- Primary RT — for patients who are not surgical candidates or with radiosensitive tumors
- Primary systemic therapy — for chemosensitive tumors (lymphoma, myeloma, germ cell, SCLC) in the absence of clinical myelopathy, with close neurologic monitoring[10]
- RT dosing options: 8 Gy/1 fraction, 20 Gy/5 fractions, or 30 Gy/10 fractions; SBRT (16–24 Gy/1 fraction) preferred for life expectancy ≥3 months[10]
- SPINE-2. Metastatic Spine Tumors: Treatment and Adjuvant Treatment — NCCN Guidelines® — Central Nervous System Cancers p. 85 (v1.2026) Central Nervous System Cancers. April 23, 2026.
- OpenEvidence has a License from NCCN to use the NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) for Central Nervous System Cancers Version 1.2026. © National Comprehensive Cancer Network, Inc. 2026. All rights reserved.
Surgery indications
- Spinal instability
- No prior cancer history (need tissue diagnosis)
- Rapid neurologic deterioration during RT
- Previous RT to the site
- Single-site cord compression
- Life expectancy ≥3 months; not paraplegic >24 hours
- Epidural Abscess: Urgent surgical decompression + IV antibiotics (S. aureus coverage); selected patients may be managed with antibiotics alone[7]
- Epidural Hematoma: Emergent surgical evacuation + reversal of anticoagulation[1]
17. Disposition
Admit (essentially all patients with confirmed SCC)
- Any new neurologic deficit (motor, sensory, or sphincter dysfunction)
- Hemodynamic instability / neurogenic shock
- Need for urgent surgery or RT
- Epidural abscess or hematoma
- Rapidly progressive symptoms
- Need for IV steroids and close neurologic monitoring
- ICU admission: Cervical/high thoracic cord compression with bradycardia, hemodynamic instability, or respiratory compromise[20-21]
- Observation (24 hours): Some MSCC patients may be observed to adjust medical/surgical treatment plans[8]
- Outpatient management: Rare; only for select MSCC patients with stable neurologic exam, mild symptoms, and reliable follow-up who can receive outpatient RT[8]
- Consults: Neurosurgery/spine surgery, radiation oncology, medical oncology, infectious disease (if abscess), rehabilitation medicine[4][8][30]
18. Follow Up / Return Precautions
- Post-treatment imaging: Spine MRI/CT 1–3 months after treatment, then every 3–4 months for 1 year, then as clinically indicated[10]
- Steroid taper: Carefully monitored; watch for adrenal insufficiency on weaning, steroid myopathy, hyperglycemia, skin changes[10]
- Rehabilitation: Early involvement of physiatry; specialized rehabilitation improves functional independence[4-5]
- VTE prophylaxis: High risk for DVT/PE — prophylaxis recommended[14]
Return precautions (patient counseling)
- New or worsening weakness in arms or legs
- Loss of bladder or bowel control
- New numbness, especially in the saddle area
- Worsening or new back/neck pain
- Difficulty walking or falls
- Fever (if history of abscess or immunosuppression)
- Expected course: Neurologic outcome is primarily determined by pretreatment function — patients who are ambulatory at treatment initiation have the best prognosis for maintaining ambulation.[2][4-5]
References
1. Acute Spinal Cord Compression. — Ropper AE, Ropper AH. The New England Journal of Medicine. 2017.
2. Metastatic Epidural Spinal Cord Compression. — Cole JS, Patchell RA. The Lancet. Neurology. 2008.
3. Spinal Cord Compression in Patients With Advanced Metastatic Cancer: “All I Care About Is Walking and Living My Life”. — Abrahm JL, Banffy MB, Harris MB. The Journal of the American Medical Association. 2008.
4. Assessment and Management of Patients With Metastatic Spinal Cord Compression: A Multidisciplinary Review. — Lawton AJ, Lee KA, Cheville AL, et al. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2019.
5. Metastatic Spinal Cord Compression: Unraveling the Diagnostic and Therapeutic Challenges. — Boussios S, Cooke D, Hayward C, et al. Anticancer Research. 2018.
6. Clinical Reasoning: A 62-Year-Old Man With Symmetric Saddle Hypoesthesia and Sphincter Dysfunction. — Crausaz L, Baumgartner T, Loser V. Neurology. 2025.
7. Spinal Epidural Abscess. — Tande AJ, Currier BL, Osmon DR. The New England Journal of Medicine. 2026.
8. Initial Management and Disposition of Metastatic Spinal Cord Compression in the Emergency Department: A Review of the Literature. — Singer E, Elsayem A, Nassif T, et al. Annals of Medicine. 2025.
9. Assessment and Early Investigation of Cauda Equina Syndrome- A Systematic Review of Existing International Guidelines and Summary of the Current Evidence. — Hennessy O, Devitt AT, Synnott K, Timlin M. European Spine Journal : Official Publication of the European Spine Society, the European Spinal Deformity Society, and the European Section of the Cervical Spine Research Society. 2025.
10. Central Nervous System Cancers. — Updated 2026-04-24. National Comprehensive Cancer Network.
11. External Beam Radiation Therapy for Palliation of Symptomatic Bone Metastases: An ASTRO Clinical Practice Guideline. — Alcorn S, Cortés ÁA, Bradfield L, et al. Practical Radiation Oncology. 2024.
12. Small Cell Lung Cancer. — Updated 2025-09-16. National Comprehensive Cancer Network.
13. Positioning and Spinal Bracing for Pain Relief in Metastatic Spinal Cord Compression in Adults. — Lee SH, Grant R, Kennedy C, Kilbride L. The Cochrane Database of Systematic Reviews. 2015.
14. The Heart-Brain-Metabolism Axis in Cardiovascular and Neurologic Disease. — Tardo DT, Cortes-Canteli M, Fuster V, Sachdev PS, Kovacic JC. Journal of the American College of Cardiology. 2025.
15. Comprehensive Guide to the Diagnosis, Management, and Treatment of Metastatic Spinal Cord Compression Syndrome. — Vega Moreno DA, Reyes Soto G, Lopez-Valdes JC, et al. Surgical Oncology. 2025.
16. Diagnosis and Treatment of Low Back Pain (LBP) (2022). — Maj Danielle Anderson DPT DSc OCS FAAOMPT, Thiru M. Annaswamy MD MA, LTC Adam J. Bevevino MD, et al Department of Veterans Affairs. 2022.
17. Epidural Abscesses of the CNS. — Pradilla G, Ardila GP, Hsu W, Rigamonti D. The Lancet. Neurology. 2009.
18. Mystery Case: A 61-Year-Old Woman With Lower Extremity Paralysis and Sensory Loss. — Manners J, Jadhav AP, Xia Z. Neurology. 2017.
19. Degenerative Cervical Myelopathy: Recognition and Management. — Kane SF, Abadie KV, Willson A. American Family Physician. 2020.
20. Best Practices Guidelines Spine Injury. — Gregory D. Schroeder MD, Alexander R. Vaccaro MD PhD MBA, William C. Welch MD FACS FAANS FICS FAANOS, et al American College of Surgeons (2022). 2022.
21. Cardiovascular Abnormalities Accompanying Acute Spinal Cord Injury in Humans: Incidence, Time Course and Severity. — Lehmann KG, Lane JG, Piepmeier JM, Batsford WP. Journal of the American College of Cardiology. 1987.
22. Systematic Review of the Diagnosis and Management of Malignant Extradural Spinal Cord Compression: The Cancer Care Ontario Practice Guidelines Initiative's Neuro-Oncology Disease Site Group. — Loblaw DA, Perry J, Chambers A, Laperriere NJ. Journal of Clinical Oncology : Official Journal of the American Society of Clinical Oncology. 2005.
23. Nontraumatic Spinal Cord Compression: MRI Primer for Emergency Department Radiologists. — Laur O, Nandu H, Titelbaum DS, Nunez DB, Khurana B. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2019.
24. Implementation of a Survey Spine MR Imaging Protocol for Cord Compression in the Emergency Department: Experience at a Level 1 Trauma Center. — Mazurek MH, Abruzzo AR, King AH, et al. AJNR. American Journal of Neuroradiology. 2024.
25. An Integrated Multidisciplinary Algorithm for the Management of Spinal Metastases: An International Spine Oncology Consortium Report. — Spratt DE, Beeler WH, de Moraes FY, et al. The Lancet. Oncology. 2017.
26. Electrocardiographic Abnormalities in the Early Stage Following Traumatic Spinal Cord Injury. — Furlan JC, Verocai F, Palmares X, Fehlings MG. Spinal Cord. 2016.
27. Cardiac Electrophysiology of Patients With Spinal Cord Injury. — Manogue M, Hirsh DS, Lloyd M. Heart Rhythm. 2017.
28. Clinical Reasoning: A 67-Year-Old Woman With Abdominal Pain, Constipation, and Urinary Retention. — Hanna SS, Jewell R, Anker CJ, et al. Neurology. 2022.
29. Epidemiological Study of Cervical Cord Compression and Its Clinical Symptoms in Community-Dwelling Residents. — Hirai T, Otani K, Sekiguchi M, Kikuchi SI, Konno SI. PloS One. 2020.
30. Multidisciplinary Approach to Patients With Metastatic Spinal Cord Compression: A Diagnostic Therapeutic Algorithm to Improve the Neurological Outcome. — Rispoli R, Reverberi C, Targato G, et al. Frontiers in Oncology. 2022.