Spinal Epidural Abscess
Spinal epidural abscess (SEA) is a suppurative infection of the epidural space — a high-risk, low-prevalence infectious disease emergency with up to 90% of patients misdiagnosed on their first ED v…
Spinal epidural abscess (SEA) is a suppurative infection of the epidural space — a high-risk, low-prevalence infectious disease emergency with up to 90% of patients misdiagnosed on their first ED visit.[1] The classic triad of back pain, fever, and neurologic deficit is present in fewer than 10–20% of cases at diagnosis.[2-3] Overall mortality is approximately 6–13% within 90 days.[2]
The classic triad of spinal epidural abscess symptoms — focal pain, fever, and neurologic deficit — is relatively uncommon at the time of diagnosis (present in 20% of patients).
— Aaron J. Tande, M.D., et al., Mayo Clinic
Spinal Epidural Abscess. N Engl J Med. April 22, 2026.
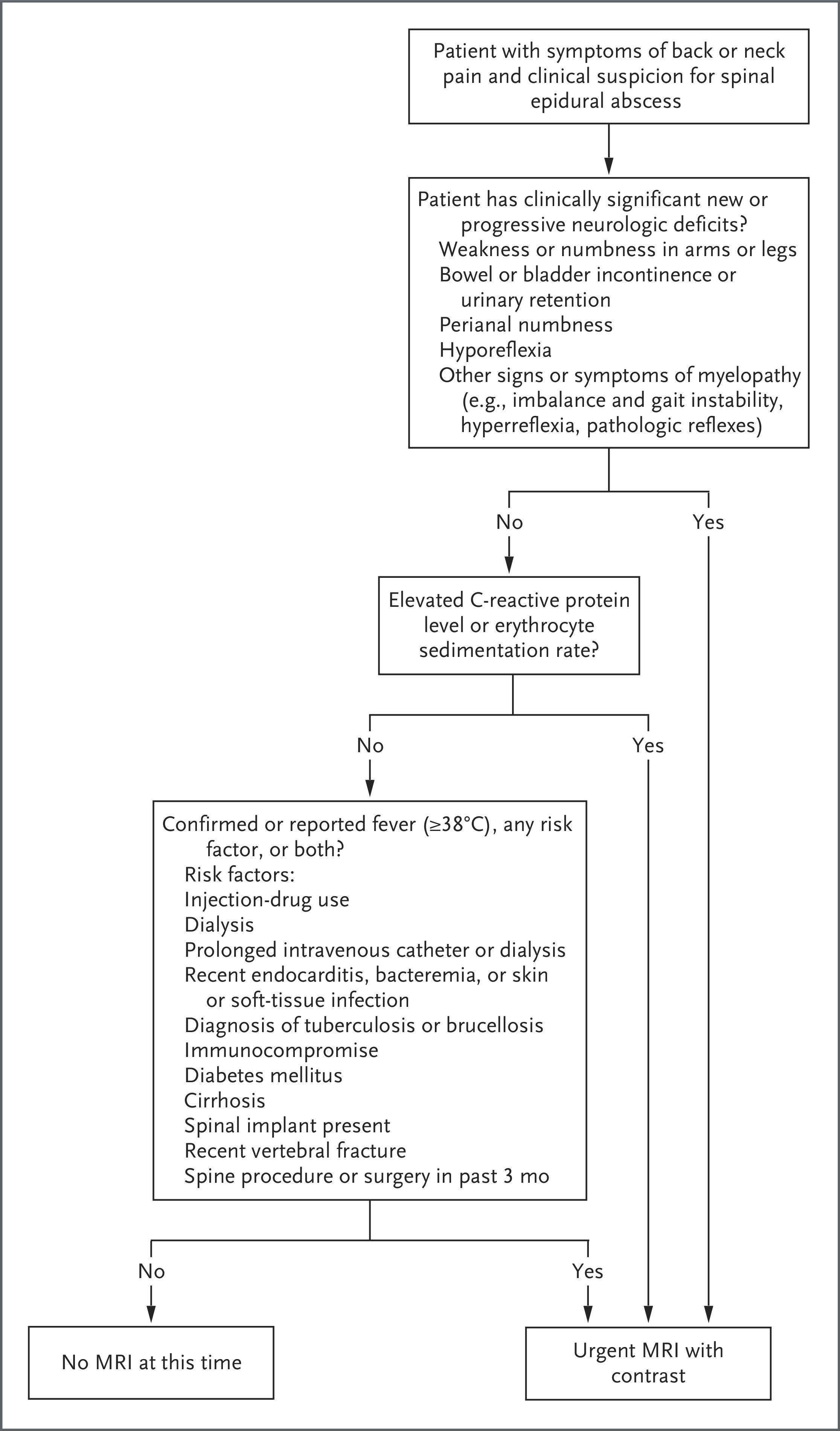
The following algorithm from the 2026 NEJM review outlines when to pursue urgent MRI in patients with suspected SEA:
View full figure Figure 2. Algorithm for Use of Urgent MRI to Evaluate for Spinal Epidural Abscess.<sup><xref ref-type="bibr" rid="r27">27</xref>,<xref ref-type="bibr" rid="r33">33</xref>,<xref ref-type="bibr" rid="r42">42</xref>,<xref ref-type="bibr" rid="r43">43</xref></sup> Spinal Epidural Abscess. N Engl J Med. April 22, 2026.
1. History
- Key HPI questions: Characterize pain location (back vs. neck), onset, severity, and progression. Ask about radicular symptoms (shooting pain, numbness, paresthesias) and any new weakness, gait difficulty, or bowel/bladder changes[2][4]
Symptom progression follows a classic 4-phase pattern
- Phase 1: Localized back/neck pain (>80% of patients)
- Phase 2: Radicular pain
- Phase 3: Motor weakness, sensory deficit, sphincter impairment (present at diagnosis in 20–47%)
- Phase 4: Paralysis (3–9% at diagnosis)
- Timing: One-third of patients have symptoms >2 weeks before diagnosis; neurologic symptoms typically present <1 week before diagnosis[2]
- Important negatives: Absence of acute back pain has a negative likelihood ratio of 0.19 for SEA in S. aureus bacteremia patients. However, the absence of risk factors cannot be used to exclude SEA[1][4]
2. Alarm Features
- New or progressive neurologic deficits — extremity weakness/numbness, bowel/bladder dysfunction, saddle anesthesia, gait instability[2]
- Rapidly progressive symptoms — neurologic deterioration can accelerate once it begins[2][5]
- Sepsis or hemodynamic instability (present in 25–35%)[2]
- Fever with severe, localized spinal tenderness in a patient with risk factors[6]
- Saddle anesthesia has the highest positive likelihood ratio (22.6) for ruling in SEA among S. aureus bacteremia patients[4]
3. Medications
- Empiric therapy: Vancomycin + ceftriaxone is an appropriate first-line regimen[2]
- Upgrade to cefepime (replacing ceftriaxone) in patients with IVDU, surgical-site infection, sepsis, or substantial neurologic deficits[2]
- Withhold antibiotics until cultures are obtained in neurologically intact, non-septic patients without cord compression — to maximize culture yield[2]
- Do not delay antibiotics in patients with sepsis, neurologic deficits, or hemodynamic instability — obtain blood cultures and start empiric therapy immediately[2][7]
- Duration: Typically 6–8 weeks of parenteral therapy, individualized to clinical response; oral step-down with highly bioavailable agents may be considered in selected patients with adequate response[2]
- Antifungals (voriconazole, amphotericin B) should be added if fungal etiology is suspected[7]
4. Diet
- No specific dietary triggers or recommendations unique to SEA
- Adequate nutrition and glycemic control are important, particularly in diabetic patients, to optimize infection management and wound healing
- Ensure adequate hydration, especially during prolonged IV antibiotic therapy
5. Review of Systems
- Neurologic: Weakness, numbness, paresthesias, gait changes, bowel/bladder dysfunction, saddle numbness[2][4]
- Constitutional: Fever, chills, night sweats, malaise, weight loss[2]
- Musculoskeletal: Localized spinal tenderness, radicular pain[2]
- Infectious sources: Skin/soft tissue infections, urinary symptoms, dental infections, recent procedures, endocarditis symptoms (new murmur, embolic phenomena)[8-9]
- Meningeal symptoms: Headache, neck stiffness — meningitis may accompany SEA if dural tear is present[2]
6. Collateral History and Family History
- Injection drug use history — often underreported; collateral from family/friends is critical (LR+ 13.7 for SEA)[6]
- Recent spinal procedures — epidural injections, surgery, lumbar puncture[2][10]
- Indwelling vascular catheters (LR+ 15.7)[6]
- Recent hospitalizations, infections, or bacteremia[9]
- Family history is generally not a major contributor, though immunodeficiency syndromes may be relevant
- Social context: housing instability, alcohol use disorder, HIV status[2][8]
7. Risk Factors
- Injection drug use — strongest independent risk factor in case-control data[2]
- Diabetes mellitus — most commonly reported comorbidity; also predicts failure of medical management[2][11]
- Immunocompromise — HIV, chronic steroid use, transplant, active cancer[2][8]
- Bacteremia / concurrent infection — skin infections, UTI, endocarditis, psoas abscess[1][9]
- Spinal instrumentation or recent spinal procedures[2][10]
- Alcohol abuse and obesity — independent risk factors[2]
- Renal failure / dialysis[2][8]
- Demographics: Predominantly male, age 50–65 years; median age ~55–63 years[2-3][12]
- Absence of risk factors does not exclude SEA — 22.7% of patients in one series had no identifiable risk factors[1][13]
8. Differential Diagnosis
- Vertebral osteomyelitis / discitis — often coexists with SEA; may be the primary process[8-9]
- Spinal subdural abscess — distinguished from SEA on MRI by preservation of the epidural space[2]
- Intramedullary spinal cord abscess — ring-enhancing cord lesion on contrast MRI[2]
- Spinal epidural hematoma — especially in anticoagulated patients; acute onset
- Spinal cord tumor / metastatic epidural compression — progressive neurologic deficits without infectious signs[8]
- Cauda equina syndrome (disc herniation) — bowel/bladder dysfunction, saddle anesthesia without fever
- Transverse myelitis — inflammatory, typically without fever or elevated inflammatory markers
- Psoas abscess — may be contiguous with SEA; hip flexion pain
- Meningitis — may coexist with SEA[2]
- Musculoskeletal back pain — the most common mimic; SEA is frequently misdiagnosed as benign back pain[1][3]
9. Past Medical History
- Prior episodes of SEA or vertebral osteomyelitis
- History of spinal surgery or instrumentation
- Diabetes mellitus, chronic kidney disease, liver disease
- HIV/AIDS, organ transplant, malignancy
- History of endocarditis or recurrent bacteremia
- Chronic indwelling catheters (PICC, dialysis catheter)
- Prior IVDU or alcohol use disorder
10. Physical Exam
- Vital signs: Fever present in only 24–62% of patients; tachycardia and hypotension suggest sepsis[2][12]
- Spine: Focal midline tenderness is a key finding — spine tenderness has a positive LR of 7.5 for SEA; its absence has a negative LR of 0.62. Percussion tenderness over the affected area[4]
Neurologic exam (critical)
- Motor strength testing in all extremities
- Sensory exam including perianal/saddle sensation (saddle anesthesia PLR 22.6)[4]
- Deep tendon reflexes — hyporeflexia (cauda equina) vs. hyperreflexia (cord compression)
- Rectal tone assessment
- Gait evaluation
- Skin: Examine for injection sites, skin/soft tissue infections, surgical wounds
- 40% of patients present without neurological deficit[12]
11. Lab Studies
- ESR and CRP — most sensitive screening labs; typically markedly elevated (CRP >100 mg/L, ESR >60 mm/h). ESR >75 mm/h is associated with medical treatment failure[2][11]
- WBC — elevated in 60–80% but less sensitive and specific than ESR/CRP[2][7]
- Blood cultures — obtain before antibiotics; positive in 26–71% of cases. Concordance with surgical cultures ~60%[2][7]
- Procalcitonin — may be useful adjunct but not well studied specifically for SEA
- Basic metabolic panel, hepatic function, coagulation studies — for surgical planning and antibiotic dosing
- HIV testing if not previously known
- Lactate if sepsis is suspected
- Hemoglobin A1c in diabetic patients
12. Imaging
- First-line: MRI with gadolinium contrast — sensitivity 96%, specificity 93–94%. This is the diagnostic test of choice[2][14-15]
- Once SEA is diagnosed, image the entire spine — noncontiguous skip lesions found in up to 9% of patients[2]
- CT with IV contrast — inferior alternative when MRI is unavailable; sensitivity as low as 18%[2]
- PET-CT — alternative in patients who cannot undergo MRI, though inferior[2]
- CT myelography — invasive, rarely performed; risk of subarachnoid contamination[7]
- Repeat MRI in 2–3 weeks if initial MRI is unremarkable but clinical suspicion persists[7]
- DWI sequences can further aid in abscess characterization and distinguish from Modic type 1 changes[14]
13. Special Tests
- Image-guided needle aspiration/biopsy — for microbiologic diagnosis when blood cultures are negative and surgery is not imminent; target accessible contiguous sites (psoas abscess, paraspinal collection) over epidural fluid to avoid thecal puncture[2]
- Intraoperative cultures — 3–5 tissue/fluid samples for aerobic and anaerobic culture with Gram stain[2]
- Lumbar puncture should be avoided — risk of contaminating the subarachnoid space[8]
- Echocardiography — consider to evaluate for concurrent endocarditis, especially with S. aureus bacteremia[8]
- Predictive models for medical treatment failure: Age >65, diabetes, MRSA, neurologic deficit at presentation, CRP >115, WBC >12.5, positive blood cultures[2][13]
14. ECG
- ECG is not directly diagnostic for SEA
- Obtain ECG if sepsis is present (evaluate for tachyarrhythmias, ischemia)
- Relevant if concurrent endocarditis is suspected (conduction abnormalities, new heart block)
- Baseline ECG before initiating vancomycin (QTc monitoring if combined with other QT-prolonging agents)
15. Assessment
- SEA is a time-sensitive infectious disease emergency with a high rate of diagnostic delay — 71% of patients had potentially related visits in the 30 days prior to diagnosis[3]
- Staphylococcus aureus is the causative pathogen in >50% of cases, evenly split between MSSA and MRSA[2][8]
- Other pathogens: streptococci, aerobic gram-negative bacilli, anaerobes; rarely mycobacteria, fungi, Nocardia[9]
- Thoracic spine is most commonly affected in hematogenous cases; lumbar spine is most common overall (51% in one large series)[3][8]
- Severity stratification should incorporate neurologic status (ASIA scale), sepsis criteria, and predictors of medical treatment failure[2][13]
- Mortality: ~3–6% in-hospital, 6–13% at 90 days; overall mortality ~11%[2][12]
16. Treatment Plan
Initial stabilization
- ABCs, IV access, hemodynamic resuscitation if septic
- Obtain blood cultures immediately
Antibiotics
- Empiric: Vancomycin + ceftriaxone (or cefepime in IVDU, surgical-site infection, sepsis, or significant neurologic deficits)[2]
- In neurologically intact, non-septic patients without cord compression: consider withholding antibiotics until image-guided biopsy to optimize culture yield[2]
- Narrow therapy based on culture and susceptibility data; ID consultation essential[2]
- Duration: 6–8 weeks parenteral, with individualization based on response; oral step-down may be appropriate in selected patients[2]
Surgical management
- Urgent surgery indicated for new or progressive neurologic deficits — neurologic recovery is most likely when surgery occurs within 48–72 hours of symptom onset[2]
- Laminectomy with decompression is the standard surgical approach; multilevel laminectomy or catheter-based irrigation for extensive abscesses[2]
- Paralysis >48 hours is a poor prognostic sign but does not preclude some recovery[8]
Nonoperative management
- May be appropriate in carefully selected patients: neurologically intact, no cord compression, no sepsis[2]
- Failure rate ~28–42%, and delayed surgery has worse outcomes than early surgery[2][11][13]
- Predictors of failure: DM, MRSA, age >65, elevated CRP/ESR, bacteremia, anterior epidural involvement, leukocytosis[2][11][13]
17. Disposition
- All patients with confirmed SEA require hospital admission — there is no role for outpatient management at diagnosis[2]
- ICU admission for sepsis, hemodynamic instability, or rapidly progressive neurologic deficits
- Spine surgery and infectious disease consultation are mandatory for all patients[2]
- Transfer to a facility with spine surgery capability if not available locally; telemedicine ID consultation can bridge the gap[2]
- Patients managed nonoperatively require close neurologic monitoring — serial exams at minimum every few hours initially[2]
- Observation in a monitored setting is appropriate for patients being considered for nonoperative management
18. Follow Up / Return Precautions
- During hospitalization: Serial neurologic exams; monitor ESR/CRP trends; repeat MRI if clinical worsening or inflammatory markers not improving[2]
- Post-discharge: Follow-up with ID and spine surgery; complete antibiotic course (typically via OPAT); monitor for PICC-line complications
- End-of-therapy evaluation: Neurologic exam, ESR/CRP compared to baseline; end-of-therapy MRI recommended for nonoperatively treated patients, those with MRSA, or those without abscess drainage[2]
Return precautions (counsel patients explicitly)
- Any new or worsening weakness, numbness, or tingling
- New bowel or bladder dysfunction
- Worsening or new back/neck pain
- Fever or rigors
- Symptoms of line infection (redness, swelling, drainage at PICC site)
- Expected recovery: Most survivors are cured; recurrence is uncommon. Neurologic outcomes are best predicted by neurologic status at the time of treatment initiation. Meta-analysis shows good neurologic outcome in 86% with early surgery vs. 69% with nonoperative treatment[2]
References
1. High Risk and Low Prevalence Diseases: Spinal Epidural Abscess. — Long B, Carlson J, Montrief T, Koyfman A. The American Journal of Emergency Medicine. 2022.
2. Spinal Epidural Abscess. — Tande AJ, Currier BL, Osmon DR. The New England Journal of Medicine. 2026.
3. Diagnostic Delays Are Common, and Classic Presentations Are Rare in Spinal Epidural Abscess. — Durant EJ, Copos S, Folck BF, et al. The Western Journal of Emergency Medicine. 2025.
4. Clinical Evaluation for Spinal Epidural Abscess in Patients With Staphylococcus Aureus Bacteraemia: A Diagnostic Accuracy Study. — Obeda MJ, Dalai AS, Monti EB, et al. Infectious Diseases. 2026.
5. Epidural Abscesses of the CNS. — Pradilla G, Ardila GP, Hsu W, Rigamonti D. The Lancet. Neurology. 2009.
6. Diagnosis and Treatment of Low Back Pain (LBP) (2022). — Maj Danielle Anderson DPT DSc OCS FAAOMPT, Thiru M. Annaswamy MD MA, LTC Adam J. Bevevino MD, et al Department of Veterans Affairs. 2022.
7. Spinal Epidural Abscess: A Review with Special Emphasis on Earlier Diagnosis. — Bond A, Manian FA. BioMed Research International. 2016.
8. Acute Spinal Cord Compression. — Ropper AE, Ropper AH. The New England Journal of Medicine. 2017.
9. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
10. ASRA Pain Medicine Consensus Practice Infection Control Guidelines for Regional Anesthesia and Pain Medicine. — Provenzano DA, Hanes M, Hunt C, et al. Regional Anesthesia and Pain Medicine. 2025.
11. Outcomes and Factors Associated With Medical Treatment Failure in Patients With Spinal Epidural Abscess: A 14-Year Experience. — García de Santos M, Calderón-Parra J, Gutiérrez-Villanueva A, et al. PloS One. 2025.
12. Clinical Characteristics of Patients With Spinal Epidural Abscess: A Systematic Review and Meta-Analysis. — Budiman L, Abetz JW, Mitra B. Emergency Medicine Australasia : EMA. 2026.
13. Spinal Epidural Abscesses: Risk Factors, Medical Versus Surgical Management, a Retrospective Review of 128 Cases. — Patel AR, Alton TB, Bransford RJ, et al. The Spine Journal : Official Journal of the North American Spine Society. 2014.
14. ACR Appropriateness Criteria® Cervical Pain or Cervical Radiculopathy: 2024 Update. — Eldaya RW, Parsons MS, Hutchins TA, et al. Journal of the American College of Radiology : JACR. 2025.
15. ACR Appropriateness Criteria® Suspected Spine Infection. — Expert Panel on Neurological Imaging, Ortiz AO, Levitt A, et al. Journal of the American College of Radiology : JACR. 2021.