Spinal Hematoma
Spinal hematoma is a rare but potentially catastrophic neurological emergency characterized by blood accumulation within the spinal canal (epidural, subdural, subarachnoid, or intramedullary), most…
Spinal hematoma is a rare but potentially catastrophic neurological emergency characterized by blood accumulation within the spinal canal (epidural, subdural, subarachnoid, or intramedullary), most commonly in the epidural space. Estimated incidence of spontaneous spinal epidural hematoma (SSEH) is 0.1 per 100,000/year.[1-2] Rapid recognition and intervention are critical, as delays lead to permanent neurological deficits.
1. History
- Onset: Sudden, severe neck or back pain is the chief complaint in ~79% of cases, often described as "thunderclap" or "worst ever"[1][3]
- Progression: Pain followed by rapidly evolving motor weakness, sensory changes, and/or sphincter dysfunction — minutes to hours[1][4]
- Timing: Ask about exact time of symptom onset (critical for surgical decision-making); symptoms may progress in <1 hour in severe cases[1]
- Triggers: Recent spinal procedure (epidural, LP, spinal surgery), trauma, Valsalva maneuver, heavy lifting, extreme neck movements[2][4-5]
- Anticoagulant/antiplatelet use: Warfarin, DOACs, heparin, LMWH, aspirin, clopidogrel — present in ~20% of spontaneous cases[1][6]
- Associated symptoms: Radicular pain, bilateral leg weakness, urinary retention/incontinence, saddle anesthesia
- Important negatives: Absence of cranial nerve deficits (helps distinguish from stroke), no fever (distinguishes from epidural abscess)[7]
2. Alarm Features
- Rapidly progressive paraparesis or tetraparesis — surgical emergency[1][8]
- Sphincter dysfunction (urinary retention, fecal incontinence) — associated with poor prognosis[1]
- Complete motor deficit (ASIA Grade A) — strongest predictor of poor outcome[1]
- Rapid neurological deterioration (<1 hour from onset to severe deficit)[1]
- Cervical hematoma with respiratory compromise — risk of diaphragmatic paralysis
- Brown-Séquard syndrome — recognized presentation of cervical epidural hematoma[4][7]
- Hemiparesis without cranial nerve signs — suspect cervical spinal hematoma, NOT stroke; thrombolysis is contraindicated and can be fatal[7]
3. Medications
Relevant contributors
- Warfarin — independently associated with worse surgical outcomes[9]
- DOACs (rivaroxaban, apixaban, dabigatran, edoxaban) — all carry black box warnings regarding neuraxial procedures; associated with SSEH[10-11]
- LMWH/UFH — risk increases with therapeutic dosing, traumatic needle placement, and concomitant aspirin[12]
- Antiplatelets (aspirin, clopidogrel, dual antiplatelet therapy)[6]
- Reversal agents (administer emergently, do not wait for lab confirmation):[13-14]
- Warfarin: 4-factor PCC (25–50 IU/kg) + IV vitamin K 10 mg
- Dabigatran: Idarucizumab 5 g IV
- Factor Xa inhibitors: 4-factor PCC or aPCC (andexanet alfa was withdrawn from the US market)[13][15]
- UFH/LMWH: Protamine sulfate
- Thrombocytopenia: Platelet transfusion to target >100,000/μL for neurosurgical intervention
Contraindicated medications
- tPA/thrombolytics — absolutely contraindicated; can worsen hemorrhage and cause death[7]
- Resumption of anticoagulation should be deferred until hemostasis is confirmed and neurosurgical clearance obtained
4. Diet
- Not directly applicable in the acute setting
- Post-operatively, patients with prolonged immobility should receive adequate hydration and fiber to prevent constipation (which can trigger autonomic dysreflexia in cervical/high thoracic injuries)
- Nutritional optimization for wound healing in surgical patients
5. Review of Systems
- Neurological: Weakness (bilateral vs. unilateral), numbness/tingling, gait difficulty, bowel/bladder changes
- Musculoskeletal: Back/neck pain severity, radiation pattern
- Vascular: History of DVT/PE, recent vascular procedures
- Constitutional: Fever (abscess), weight loss (malignancy), night sweats
- Hematologic: Easy bruising, bleeding gums, menorrhagia (coagulopathy)
- Cardiovascular: Palpitations, syncope (neurogenic shock in cervical injuries)[16-17]
6. Collateral History and Family History
- Medication reconciliation: Confirm exact anticoagulant/antiplatelet agents, doses, and timing of last dose — critical for reversal strategy[13]
- Recent procedures: Epidural anesthesia, lumbar puncture, spinal surgery, interventional pain procedures[5][12]
- Bleeding history: Prior hemorrhagic events, known coagulopathy
- Family history: Hereditary bleeding disorders (hemophilia, von Willebrand disease), vascular malformations
- Functional baseline: Pre-morbid ambulatory status and independence level
7. Risk Factors
- Anticoagulant/antiplatelet therapy — most significant modifiable risk factor (~20–74% of cases depending on series)[1][6]
- Coagulopathy (thrombocytopenia, liver disease, DIC, hemophilia)[12]
- Hypertension[2][18]
- Spinal vascular malformations (arteriovenous fistulas found in ~15% on DSA)[1]
- Age: Bimodal distribution — peaks in 2nd and 6th decades; elderly women at highest risk for procedure-related hematoma (1:3,600 for epidural in knee arthroplasty)[1][12]
- Spinal procedures: Epidural catheter placement/removal, lumbar puncture, spinal surgery[5][12]
- Spinal pathology: Degenerative spondylosis, osteoporotic deformities, prior spinal surgery[12]
- Pregnancy: Relatively protective due to hypercoagulable state (1:200,000 risk)[12]
- Trauma (including minor)[2][8]
8. Differential Diagnosis
- Epidural abscess — fever, elevated WBC/ESR/CRP, IV drug use, immunosuppression; ring enhancement on MRI[8][19]
- Metastatic spinal cord compression — known malignancy, progressive course, bony destruction on imaging[8]
- Acute disc herniation — typically unilateral radiculopathy, less commonly myelopathy
- Spinal cord infarction — apoplectic onset, anterior cord syndrome, no mass on MRI[19]
- Transverse myelitis — subacute onset (days to weeks), intramedullary T2 signal without mass[19]
- Ischemic stroke (cervical hematoma mimic) — presence of cranial nerve deficits favors stroke; absence favors spinal pathology[7]
- Spinal subdural hematoma — crescentic shape on MRI, may require intradural surgical approach[20-21]
- Dural arteriovenous fistula — stepwise progression, flow voids on MRI[19]
- Cauda equina syndrome (other causes) — disc herniation, tumor
9. Past Medical History
- Prior spinal surgeries or procedures (increased risk of postoperative hematoma)[5]
- Previous episodes of spinal hematoma
- Atrial fibrillation or VTE requiring anticoagulation
- Liver disease, renal insufficiency (affects drug clearance and coagulation)
- Known vascular malformations
- Malignancy (risk of metastatic compression and coagulopathy)
- Hypertension
10. Physical Exam
Vital signs
- Hypotension + bradycardia = neurogenic shock (cervical/high thoracic lesions at or above T6)[16-17]
- Hypertension may be present as a risk factor or with autonomic dysreflexia
Focused neurological exam
- Motor: Bilateral lower extremity weakness (paraparesis/paraplegia) or all four extremities (tetraparesis) — grade using ASIA scale[22-23]
- Sensory: Dermatomal sensory level; check pinprick and light touch bilaterally
- Reflexes: Hyperreflexia below the level (upper motor neuron); hyporeflexia/areflexia in acute spinal shock
- Rectal exam: Perianal sensation, anal tone, voluntary anal contraction — critical for ASIA classification (complete vs. incomplete)[22]
- Brown-Séquard pattern: Ipsilateral motor loss + contralateral pain/temperature loss[4][7]
- Horner syndrome: Ipsilateral ptosis, miosis, anhidrosis (cervical lesions)[7]
- Lhermitte's sign: Electric shock sensation with neck flexion[7]
- Spinal tenderness: Focal midline tenderness at the level of the hematoma
11. Lab Studies
- CBC with platelets — assess for thrombocytopenia
- PT/INR, aPTT — detect coagulopathy, guide warfarin reversal
- Fibrinogen — rule out DIC or consumptive coagulopathy
- Type and screen — anticipate surgical blood loss
- BMP, hepatic panel — renal/hepatic function affects drug metabolism and coagulation
- Drug-specific anti-Xa levels (if on factor Xa inhibitors) or thrombin time/ecarin clotting time (if on dabigatran) — helpful but should NOT delay reversal[13-14]
- ESR/CRP, blood cultures — if epidural abscess is in the differential
- Lactate — if neurogenic shock suspected
12. Imaging
- First-line: MRI of the entire spine (with and without contrast)
- Gold standard for diagnosis[20][24]
- Identifies location (epidural vs. subdural vs. intramedullary), extent, and degree of cord compression
Typical MRI findings
- Biconvex, posterior dorsal mass in the epidural space (90.5% dorsal/dorsolateral)[1]
- T1: Isointense to cord acutely; hyperintense in subacute phase
- T2: Heterogeneous hyperintensity with focal hypointensity acutely
- Dura seen as a low-signal curvilinear line separating hematoma from cord[27]
- Average extension over 3.3 vertebral segments[1]
- Most common locations: cervicothoracic (C5–T2) and thoracolumbar (T10–L2)[1-2]
When MRI is unavailable or contraindicated
- CT myelography — alternative for detecting cord compression
- Cervical CT — can be a rapid screening tool when cervical hematoma is suspected in a stroke mimic scenario[7]
When imaging is unnecessary
13. Special Tests
- ASIA Impairment Scale (AIS) — standardized grading of spinal cord injury severity (A = complete, B–D = incomplete, E = normal); the most important prognostic tool[22-23]
- Frankel Scale — older classification, still referenced in some literature[1]
- Modified Rankin Scale (mRS) — used for functional outcome assessment[18]
- Spinal digital subtraction angiography (DSA) — consider if vascular malformation suspected (~15% of SSEH cases have abnormal vascular findings)[1]
- Lumbar puncture — may reveal xanthochromia or bloody CSF in rare cases presenting with sentinel headache; generally NOT recommended when epidural hematoma is suspected due to risk of herniation[3]
14. ECG
- ECG is indicated in all patients with cervical or high thoracic (≥T6) spinal cord compression:[16-17][29]
- Sinus bradycardia — most common dysrhythmia, universal in severe cervical cord injury[16][29]
- Cardiac arrest — reported in 16% of severe cervical injuries[29]
- ST-segment changes, T-wave inversions, QT prolongation — may mimic acute coronary syndrome[30]
- Supraventricular arrhythmias[29]
- Bradyarrhythmias peak at day 4 post-injury and resolve within 2–6 weeks[29]
- Continuous telemetry monitoring is essential in the acute phase
15. Assessment
- Spinal hematoma is a time-critical neurosurgical emergency. Key assessment points:
- Severity stratification: ASIA Grade A (complete) carries the worst prognosis; preoperative neurological status is the strongest independent predictor of outcome[1][9]
- Typical presentation: Acute severe back/neck pain → progressive motor/sensory deficit → sphincter dysfunction, evolving over minutes to hours[1]
- Atypical presentations: Hemiparesis mimicking stroke (cervical hematoma), sentinel headache without initial neurological deficit, isolated radiculopathy[3][7]
- Complications: Permanent paraplegia/tetraplegia, neurogenic shock, autonomic dysreflexia, DVT/PE, respiratory failure (cervical lesions), urinary retention, pressure injuries
16. Treatment Plan
Initial stabilization
- ABCs — secure airway if cervical cord compression with respiratory compromise
- IV access, continuous monitoring (telemetry, pulse oximetry, BP)
- Maintain MAP ≥85 mmHg in neurogenic shock (vasopressors: norepinephrine or phenylephrine)[17]
- Treat bradycardia with atropine; consider dopamine or transcutaneous pacing for refractory cases[16][31]
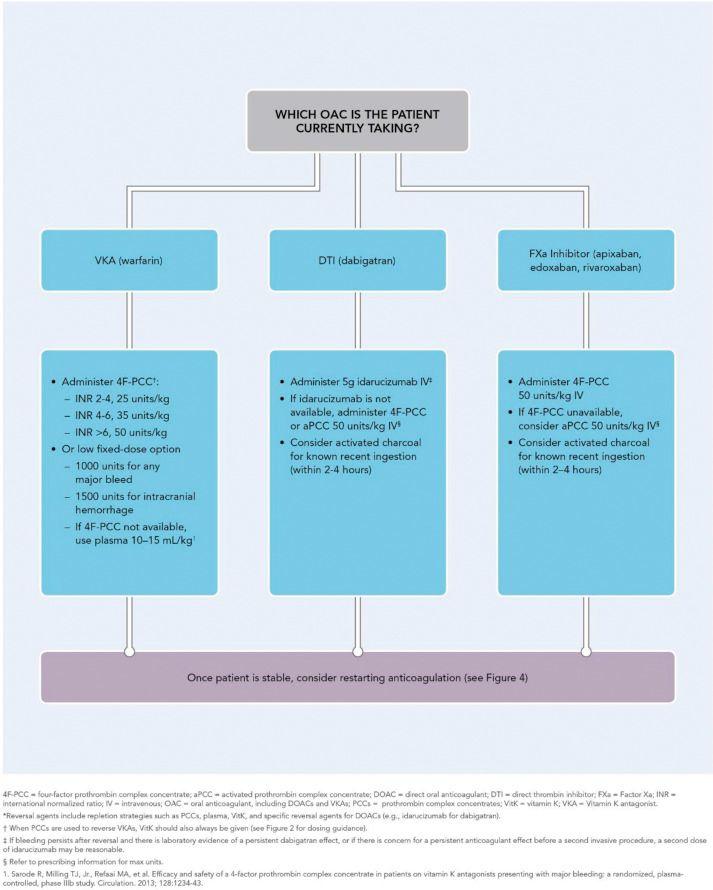
- Anticoagulant reversal (administer immediately, do not wait for labs):[13-14]
- Warfarin → 4-factor PCC + IV vitamin K 10 mg
- Dabigatran → Idarucizumab 5 g IV
- Factor Xa inhibitors → 4-factor PCC 25–50 IU/kg (or aPCC)
- Heparin → Protamine sulfate
- Correct thrombocytopenia (target platelets >100,000 for surgery)
- The ACC/AHA reversal algorithm is summarized in the following figure:
- View full figure Figure 3. Guidance for Administering Reversal Agents* 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. December 18, 2017.
Surgical intervention
- Decompressive laminectomy with hematoma evacuation is the definitive treatment for patients with moderate-to-severe neurological deficits[1][9][18]
- Timing: Surgery within 12 hours of symptom onset is associated with the best functional outcomes; ultraearly surgery (<12 hours) showed 100% favorable outcomes vs. 63.6% for delayed surgery in one series[9][33]
- The critical interval is from onset of neurological deficit to surgery, not from pain onset[1]
Conservative management
- May be appropriate in patients with mild or improving neurological deficits (Frankel D–E)[1]
- Approximately 73–84% of conservatively managed patients achieve complete recovery[1]
- Requires serial neurological exams (every 1–2 hours initially) with immediate surgical backup
- Repeat MRI to confirm hematoma resolution
17. Disposition
- Admission criteria (all patients with confirmed spinal hematoma):
- ICU admission for cervical/high thoracic lesions (hemodynamic instability, respiratory monitoring)[16-17]
- Neurosurgical/spine surgery service for operative candidates
- Monitored bed for conservatively managed patients with serial neuro checks
Specialist consultation triggers
- Neurosurgery/spine surgery — emergent consultation for all cases with neurological deficit[1][8]
- Hematology — for complex coagulopathy management
- Interventional radiology — if vascular malformation suspected on MRI
Observation indications
- Mild deficits with stable or improving exam on serial assessments
- Small hematoma without significant cord compression on MRI
18. Follow Up / Return Precautions
For surgically treated patients
- Inpatient rehabilitation referral for residual deficits
- Follow-up MRI at 4–6 weeks to confirm hematoma resolution
- Neurosurgery follow-up within 2–4 weeks
- DVT prophylaxis during recovery (mechanical + pharmacologic when safe)
- Reassess need for anticoagulation — multidisciplinary discussion weighing thrombotic vs. hemorrhagic risk
For conservatively managed patients
- Close outpatient follow-up within 1 week
- Serial MRI to document hematoma resolution
- Strict return precautions: any new or worsening weakness, numbness, bowel/bladder changes, or increasing pain requires immediate ED evaluation
Expected recovery
- 69–92% of surgically treated patients achieve favorable outcomes (mRS ≤2 or significant ASIA improvement)[18][34]
- Recovery depends primarily on preoperative neurological status and time to decompression[1][9]
- Patients with ASIA Grade A at presentation have the poorest prognosis regardless of surgical timing[1]
- Neurological recovery may continue for months after surgery
Patient counseling
- Emphasize that any new neurological symptom is an emergency
- Discuss anticoagulation risks and alternatives with prescribing physician before resuming therapy
- Rehabilitation expectations and timeline
References
1. Prognostic Factors and Treatments Efficacy in Spontaneous Spinal Epidural Hematoma: A Multicenter Retrospective Study. — Peng D, Yan M, Liu T, et al. Neurology. 2022.
2. Prognosis After Spinal Cord and Cauda Compression in Spontaneous Spinal Epidural Hematomas. — Bakker NA, Veeger NJ, Vergeer RA, Groen RJ. Neurology. 2015.
3. Spontaneous Spinal Epidural Hemorrhage and Sentinel Headache-a Case Report. — Hanna JP, Absher JR, Enyart DS. Headache. 2021.
4. Pearls & Oy-Sters: Localization in Acute Stroke Management: Thinking Straight When It Comes Down to Crunch Time. — Vijayan J, Hock Luen T, Ting E, Ning C. Neurology. 2016.
5. Delayed Onset Postoperative Spinal Epidural Hematoma after Lumbar Spinal Surgery: Incidence, Risk Factors, and Clinical Outcomes. — Wang L, Wang H, Zeng Y, et al. BioMed Research International. 2020.
6. Spontaneous Spinal Hematoma in Patients Using Antiplatelets and Anticoagulants: A Systematic Review. — Kumar N, Palmisciano P, Dhawan S, et al. World Neurosurgery. 2024.
7. How to Avoid Misdiagnosing Spontaneous Cervical Spinal Epidural Hematoma as Ischemic Stroke: 3 Case Reports and Literature Review. — Hu Y, Su J, Cui X, et al. Cerebrovascular Diseases. 2022.
8. Acute Spinal Cord Compression. — Ropper AE, Ropper AH. The New England Journal of Medicine. 2017.
9. Prognostic Factors and Surgical Outcomes of Spontaneous Spinal Epidural Haematoma: A Systematic Review and Meta-Analysis. — Vastani A, Baig Mirza A, Khoja AK, et al. Neurosurgical Review. 2022.
10. 2017 ACC Expert Consensus Decision Pathway for Periprocedural Management of Anticoagulation in Patients With Nonvalvular Atrial Fibrillation: A Report of the American College of Cardiology Clinical Expert Consensus Document Task Force. — Doherty JU, Gluckman TJ, Hucker WJ, et al. Journal of the American College of Cardiology. 2017.
11. New Oral Anticoagulants-Induced Spinal Epidural Haematomas: Case Series and Review of Literature. — Montalbetti A, Crobeddu E, Fornaro R, et al. Neurosurgical Review. 2025.
12. Regional Anesthesia in the Patient Receiving Antithrombotic or Thrombolytic Therapy: American Society of Regional Anesthesia and Pain Medicine Evidence-Based Guidelines (Fifth Edition). — Kopp SL, Vandermeulen E, McBane RD, et al. Regional Anesthesia and Pain Medicine. 2025.
13. 2024 AHA/ASA Performance and Quality Measures for Spontaneous Intracerebral Hemorrhage: A Report From the American Heart Association/American Stroke Association. — Ruff IM, de Havenon A, Bergman DL, et al. Stroke. 2024.
14. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. — Greenberg SM, Ziai WC, Cordonnier C, et al. Stroke. 2022.
15. FDA Orange Book. — FDA Orange Book. 2026.
16. Best Practices Guidelines Spine Injury. — Gregory D. Schroeder MD, Alexander R. Vaccaro MD PhD MBA, William C. Welch MD FACS FAANS FICS FAANOS, et al American College of Surgeons (2022). 2022.
17. Cardiovascular Complications After Acute Spinal Cord Injury: Pathophysiology, Diagnosis, and Management. — Furlan JC, Fehlings MG. Neurosurgical Focus. 2008.
18. Prognostic Factors and Treatment Efficacy in Spontaneous Spinal Epidural Hematoma: A Single Center Experience and Literature Review. — Hsu CJ, Lin PZ, Ju DT, Hueng DY, Tseng KY. In Vivo. 2024.
19. Approach to Acute or Subacute Myelopathy. — Schmalstieg WF, Weinshenker BG. Neurology. 2010.
20. Spinal Hematomas: What a Radiologist Needs to Know. — Pierce JL, Donahue JH, Nacey NC, et al. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2018.
21. Reliability of Preoperative MRI Findings for Differentiating Spontaneous Spinal Subdural and Epidural Hematomas: A Multi-Institutional Retrospective Study of 27 Surgically Treated Cases. — Okuwaki S, Takahashi H, Nagashima K, et al. Journal of Clinical Medicine. 2026.
22. What individuals with Spinal Cord Injury should know about the exam. — American Spinal Injury Association (2022). 2022.
23. International Standards for Neurological Classification of Spinal Cord Injury: Revised 2019. — Rupp R, Biering-Sørensen F, Burns SP, et al. Topics in Spinal Cord Injury Rehabilitation. 2021.
24. MR Imaging of Spinal Haematoma: A Pictorial Review. — Moriarty HK, O Cearbhaill R, Moriarty PD, et al. The British Journal of Radiology. 2019.
25. MRI Findings in Spinal Subdural and Epidural Hematomas. — Braun P, Kazmi K, Nogués-Meléndez P, Mas-Estellés F, Aparici-Robles F. European Journal of Radiology. 2007.
26. Acute Spontaneous Spinal Epidural Hematomas. — Fukui MB, Swarnkar AS, Williams RL. AJNR. American Journal of Neuroradiology. 1999.
27. Spinal Epidural Haematoma: Report of 11 Cases and Review of the Literature. — Boukobza M, Guichard JP, Boissonet M, et al. Neuroradiology. 1994.
28. ACR Appropriateness Criteria® Myelopathy: 2021 Update. — Expert Panel on Neurological Imaging, Agarwal V, Shah LM, et al. Journal of the American College of Radiology : JACR. 2021.
29. Cardiovascular Abnormalities Accompanying Acute Spinal Cord Injury in Humans: Incidence, Time Course and Severity. — Lehmann KG, Lane JG, Piepmeier JM, Batsford WP. Journal of the American College of Cardiology. 1987.
30. The Heart-Brain-Metabolism Axis in Cardiovascular and Neurologic Disease. — Tardo DT, Cortes-Canteli M, Fuster V, Sachdev PS, Kovacic JC. Journal of the American College of Cardiology. 2025.
31. Cardiac Electrophysiology of Patients With Spinal Cord Injury. — Manogue M, Hirsh DS, Lloyd M. Heart Rhythm. 2017.
32. 2017 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. — Tomaselli GF, Mahaffey KW, Cuker A, et al. Journal of the American College of Cardiology. 2017.
33. Ultraearly Hematoma Evacuation (<12 Hours) Associated With Better Functional Outcome in Patients With Symptomatic Spontaneous Spinal Epidural Hematoma. — Nakamura S, Yoshida S, Matsuda H, et al. World Neurosurgery. 2023.
34. Clinical Outcome After Surgical Management of Spontaneous Spinal Epidural Hematoma. — Kissling C, Häni L, Schär RT, et al. Acta Neurochirurgica. 2024.