Spontaneous Abortion (Threatened)
Threatened Spontaneous Abortion (Threatened Miscarriage)
Threatened Spontaneous Abortion (Threatened Miscarriage)
Threatened abortion is defined as vaginal bleeding through a closed cervical os, with or without abdominal pain, during the first 20 weeks of pregnancy, with a confirmed viable intrauterine pregnancy.[1-2] It occurs in approximately 25% of all pregnancies, and about 10–20% of these will progress to complete miscarriage.[1-2] The pooled risk of miscarriage across all recognized pregnancies is approximately 15.3%.[3]
1. History
- Bleeding characterization: onset, duration, color (bright red vs. brown), volume (spotting vs. pad-soaking), passage of clots or tissue
- Pain: presence, location (midline vs. unilateral), severity, cramping vs. sharp
- Timing: gestational age by LMP, prior ultrasound dating
- Triggers: post-coital bleeding, trauma, exertion
- Associated symptoms: nausea/vomiting (presence is protective — associated with lower miscarriage risk of ~9.7%), dizziness, syncope[4-5]
- Important negatives: passage of tissue (suggests inevitable/incomplete abortion), fever, purulent discharge, unilateral pain (raises concern for ectopic)[6]
- Obstetric history: number of prior pregnancies, prior miscarriages (strongest predictor of recurrence), prior ectopic pregnancies, gestational trophoblastic disease[7-8]
2. Alarm Features
- Hemodynamic instability (tachycardia, hypotension) — suggests hemorrhage or ruptured ectopic[9]
- Heavy bleeding (soaking >1 pad/hour) with clots — increased risk of pregnancy loss (HR 5.03 when combined with cramping)[5]
- Passage of tissue or products of conception visible on exam — indicates inevitable or incomplete abortion[6]
- Open cervical os — abortion is inevitable once the cervix dilates[10]
- Severe unilateral pelvic/abdominal pain — raises concern for ectopic pregnancy[11]
- Peritoneal signs (rebound, guarding) — suggests ruptured ectopic with hemoperitoneum[9]
- Fever with vaginal bleeding — consider septic abortion[12]
3. Medications
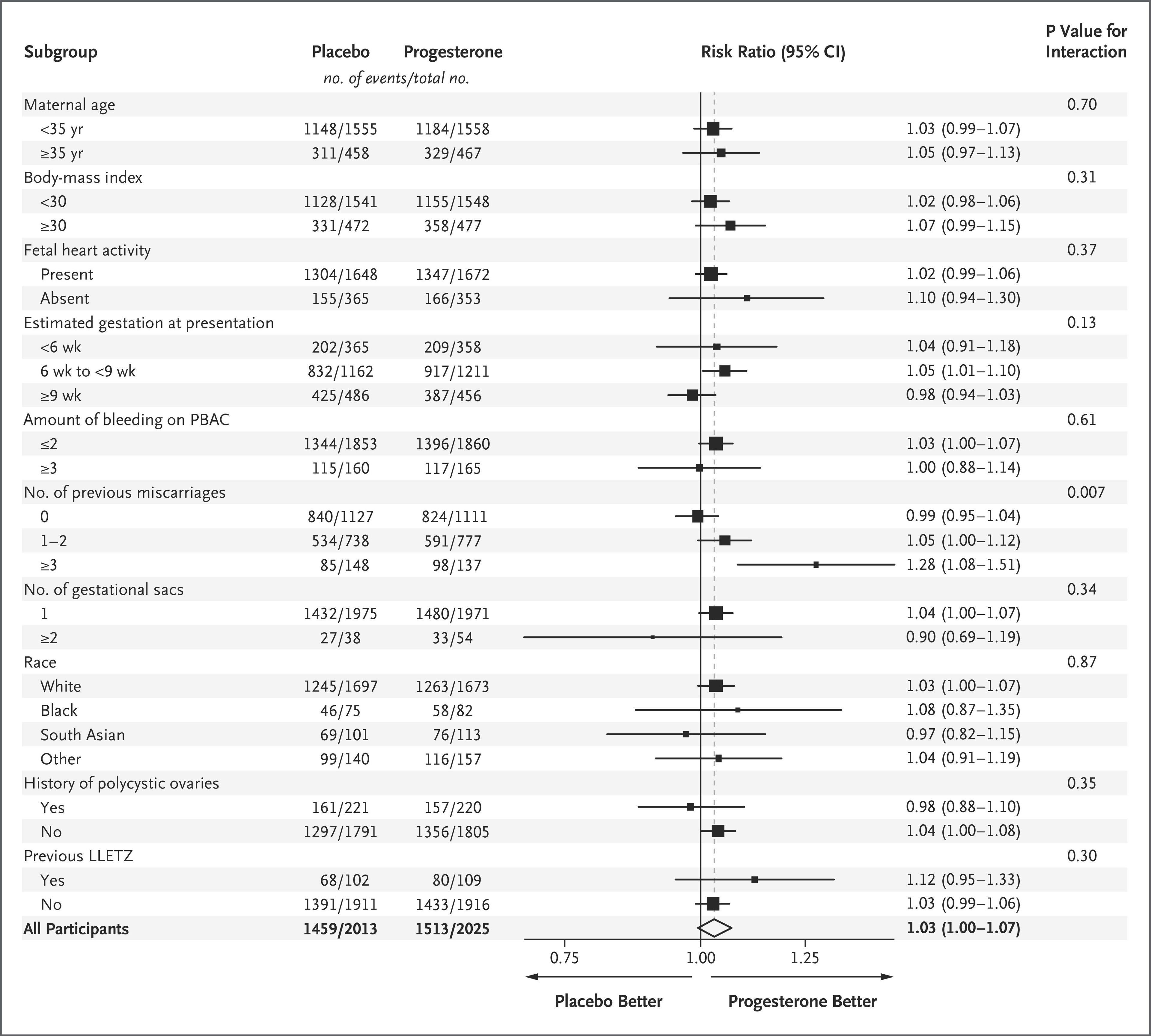
- Vaginal micronized progesterone (400 mg BID): recommended for women with early pregnancy bleeding AND a history of ≥1 prior miscarriage; continued to 16 weeks of gestation. The PRISM trial showed a 5% absolute increase in live births in women with bleeding and ≥1 prior miscarriage, and a 15% increase in those with ≥3 prior miscarriages[4][13-14]
- No proven benefit of progesterone in women with threatened miscarriage and no prior miscarriage history[15-16]
- Bed rest: does NOT improve outcomes and is not recommended[17]
- Oral dydrogesterone: not shown to reduce miscarriage rate compared to placebo[18]
- NSAIDs: avoid — associated with increased miscarriage risk[19]
- Rh(D) immune globulin: administer to Rh-negative, unsensitized women, especially later in the first trimester[7]
- Anticoagulants/aspirin: not shown to reduce early pregnancy loss except in antiphospholipid syndrome[7]
- The PRISM trial subgroup analysis demonstrated a significant interaction by number of previous miscarriages, as shown in the following figure:
- View full figure Figure 2. Subgroup Analysis. A Randomized Trial of Progesterone in Women with Bleeding in Early Pregnancy. N Engl J Med. May 8, 2019.
4. Diet
- Caffeine: high intake (>200–300 mg/day) is associated with increased miscarriage risk; advise moderation[21]
- Alcohol: any consumption during pregnancy is associated with increased miscarriage risk; advise complete abstinence[3]
- Hydration: maintain adequate hydration, especially if bleeding is significant
- Folic acid: continue prenatal supplementation (standard of care, though not specifically proven to prevent threatened miscarriage)
5. Review of Systems
- GI: nausea/vomiting (protective sign), diarrhea
- GU: dysuria, frequency (UTI can trigger uterine irritability)
- Constitutional: fever, chills (infection), lightheadedness, syncope (hemorrhage)
- Musculoskeletal: back pain (may accompany cramping)
- Endocrine: symptoms of thyroid disease (thyroid autoantibodies and subclinical hypothyroidism are associated with miscarriage)[3]
6. Collateral History and Family History
- Partner: paternal age >40 years is independently associated with increased miscarriage risk[3]
- Family history: recurrent pregnancy loss, thrombophilias (Factor V Leiden, prothrombin gene mutation), antiphospholipid syndrome, chromosomal rearrangements (balanced translocations in ~2–5% of couples with RPL)[3][22]
- Social context: domestic violence screening, psychosocial stressors (persistent stress is associated with increased risk), occupational exposures (night shifts, pesticides, air pollution)[3]
7. Risk Factors
- Advanced maternal age: risk rises from 12% (age 20–29) → 20% (age 35) → 40% (age 40) → 65% (age ≥45)[3][7]
- Prior miscarriage: risk increases ~10% per additional miscarriage (11% with none → 42% with ≥3)[3]
- Chromosomal abnormalities: account for ~50% of all early pregnancy losses[7]
- Smoking and alcohol[3]
- Obesity (BMI >24.9) or underweight (BMI <18.5)[3]
- Uterine anomalies (septate uterus, fibroids)[3]
- Antiphospholipid syndrome, thyroid autoantibodies, subclinical hypothyroidism[3]
- Infections: bacterial vaginosis, Chlamydia, TORCH infections[3]
- Poorly controlled diabetes[21]
8. Differential Diagnosis
- Ectopic pregnancy — cannot-miss diagnosis; 1–2% of pregnancies, accounts for 6% of maternal deaths. Unilateral pain, β-hCG above discriminatory zone without visible IUP[11][17]
- Inevitable/incomplete abortion — open cervical os, passage of tissue
- Missed abortion — no fetal cardiac activity, closed os, no active bleeding
- Molar pregnancy (gestational trophoblastic disease) — "snowstorm" ultrasound pattern, markedly elevated β-hCG[7]
- Cervical pathology — cervicitis, cervical polyp, cervical ectropion (post-coital bleeding)
- Subchorionic hemorrhage — common ultrasound finding; associated with increased but not definitive risk of loss[7]
- Implantation bleeding — typically light, self-limited, occurs around expected menses
- Ovarian torsion, ruptured corpus luteum cyst — unilateral pain, may have free fluid[11]
9. Past Medical History
- Prior miscarriages (number, gestational age, any workup performed)
- Prior ectopic pregnancies
- Uterine surgery (myomectomy, D&C, cesarean section — cervical trauma from LEEP increases mid-trimester loss risk)[23]
- Autoimmune conditions (antiphospholipid syndrome, SLE)
- Endocrine disorders (thyroid disease, PCOS, diabetes)
- Thrombophilias
- History of assisted reproductive technology
10. Physical Exam
- Vitals: heart rate, blood pressure (assess for hemodynamic instability), temperature (fever → infection)
- Abdominal exam: tenderness (diffuse vs. localized/unilateral), peritoneal signs, uterine size relative to dates (discrepancy ≥4 weeks is a predictor of nonviable pregnancy)[6]
Speculum exam (critical)
- Assess cervical os — closed os = threatened abortion; open os = inevitable abortion[1][10]
- Quantify bleeding, identify source (cervical vs. uterine)
- Look for visible tissue/products of conception in the os or vaginal vault
- Evaluate for cervical lesions, polyps, lacerations
- Bimanual exam: uterine size, tenderness, adnexal masses or tenderness (ectopic)
11. Lab Studies
- Quantitative β-hCG: essential for establishing pregnancy viability and trending
- Normal rise: ≥49% increase over 48 hours (for initial hCG <1,500 mIU/mL)[24]
- Discriminatory level: 1,500–3,000 mIU/mL — IUP should be visible on TVUS above this level[17][25]
- Abnormal rise or plateau raises concern for ectopic or nonviable pregnancy
- Blood type and Rh status: for Rh(D) immune globulin decision
- CBC: assess for anemia if significant bleeding
- Serum progesterone: low levels (<35 nmol/L) are the strongest predictor of miscarriage in threatened abortion (OR 26.3)[26-27]
- TSH: if thyroid disease suspected
- Consider coagulation studies if heavy bleeding or history of bleeding disorder
12. Imaging
- First-line: Transvaginal ultrasound (TVUS) combined with transabdominal US — the preferred modality for evaluating first-trimester bleeding[7][28]
- Confirm intrauterine pregnancy location
- Assess fetal cardiac activity
- Evaluate for subchorionic hemorrhage
- Diagnostic criteria for pregnancy loss (ACOG/Society of Radiologists in Ultrasound):[4][28]
- CRL ≥7 mm with no cardiac activity = diagnostic of pregnancy loss
- Mean sac diameter ≥25 mm with no embryo = diagnostic of pregnancy loss
- CRL <7 mm without cardiac activity = suspicious → repeat US in 7–10 days
- Suggestive but not diagnostic findings: slow fetal heart rate (<100 bpm at 5–7 weeks), enlarged yolk sac (>7 mm), subchorionic hemorrhage[7][28]
- MRI pelvis without contrast: may be appropriate when US is limited by habitus or nontubal ectopic is suspected[28]
- CT: generally avoided due to ionizing radiation; reserved for suspected surgical emergency
13. Special Tests
- Serial β-hCG (48-hour interval): for pregnancy of unknown location or uncertain viability[24]
- Serum progesterone: single level can serve as triage tool; ≥35 nmol/L associated with 9.6% miscarriage rate vs. 70.8% when <35 nmol/L[27]
- Point-of-care ultrasound (POCUS): in the ED, can rapidly identify IUP, free fluid, or adnexal mass
- Rh antibody screen: in Rh-negative patients
- Recurrent pregnancy loss workup (if ≥2 losses): antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, anti-β2 glycoprotein I), parental karyotyping, uterine cavity evaluation[22]
14. ECG
- Not routinely indicated
- Consider if hemodynamically unstable, significant hemorrhage, or pre-procedural assessment
- Evaluate for tachycardia patterns if concern for hypovolemic shock
15. Assessment
- Threatened abortion is a clinical diagnosis defined by vaginal bleeding with a closed cervix and a confirmed viable intrauterine pregnancy.[1-2] The key clinical priorities are:
- Confirm intrauterine pregnancy and viability (rule out ectopic — the most dangerous diagnosis to miss)
- Assess hemodynamic stability
- Risk-stratify based on bleeding severity, prior miscarriage history, maternal age, and ultrasound findings
- Approximately 50% of women with threatened abortion will carry to term.[2] Heavy bleeding combined with cramping carries the highest risk of loss (cumulative incidence ~81%).[5] Threatened miscarriage is also associated with later pregnancy complications including preterm delivery (OR 2.05), fetal growth restriction (OR 1.54), and placental abruption.[3]
16. Treatment Plan
Initial stabilization
- IV access and fluid resuscitation if hemodynamically unstable
- Type and screen; crossmatch if significant hemorrhage
- Expectant management is the standard treatment for threatened abortion with confirmed viable IUP:[17]
- No specific intervention has been proven to prevent progression in women without prior miscarriage history
- Bed rest is NOT recommended — no evidence of benefit[17]
Progesterone supplementation (for eligible patients)
- Vaginal micronized progesterone 400 mg BID, started at onset of bleeding, continued to 16 weeks
- Indicated in women with early pregnancy bleeding AND ≥1 prior miscarriage
- NNT = 18 for one additional live birth (in women with ≥1 prior miscarriage)[4]
Supportive care
- Analgesics (acetaminophen preferred; avoid NSAIDs)
- Rh(D) immune globulin if Rh-negative[7]
- Emotional support and counseling — miscarriage causes significant anxiety, depression, and PTSD symptoms[1]
17. Disposition
- Discharge criteria (majority of threatened abortions are managed outpatient):
- Hemodynamically stable
- Confirmed viable IUP on ultrasound
- Bleeding is not heavy/life-threatening
- Ectopic pregnancy excluded
- Reliable follow-up arranged
Admission criteria
- Hemodynamic instability or significant hemorrhage
- Suspected ectopic pregnancy requiring urgent intervention
- Severe pain uncontrolled with oral analgesics
- Inability to arrange timely follow-up
- Signs of infection (septic abortion)
Observation indications
- Pregnancy of unknown location with β-hCG near discriminatory zone
- Uncertain viability requiring serial assessment
Specialist consultation triggers
- OB/GYN consultation for any hemodynamically unstable patient, suspected ectopic, or need for surgical intervention
- Maternal-fetal medicine referral for recurrent pregnancy loss workup
18. Follow Up / Return Precautions
Follow-up timing
- OB/GYN or early pregnancy unit follow-up within 48–72 hours for repeat β-hCG and/or ultrasound if viability uncertain
- If viable IUP confirmed, follow-up in 7–14 days for repeat ultrasound to reassess viability[7]
- Routine prenatal care if pregnancy continues
- Return precautions — instruct patient to return immediately for:
- Heavy bleeding (soaking >1 pad/hour for ≥2 hours)
- Passage of tissue or clots
- Severe or worsening abdominal/pelvic pain
- Dizziness, lightheadedness, or syncope
- Fever or chills
- Shoulder pain (referred pain from diaphragmatic irritation — ruptured ectopic)
Patient counseling
- Light spotting may continue and does not necessarily indicate worsening
- Avoid intercourse, tampons, and douching until bleeding resolves and cleared by provider
- Continue prenatal vitamins
- Once fetal heart activity is confirmed at 8 weeks, the likelihood of live birth approaches 97–98%[3]
- Emotional support resources; miscarriage is associated with significant psychological morbidity[3]
References
1. Baseline Levels of Serum Progesterone and the First Trimester Pregnancy Outcome in Women with Threatened Abortion: A Retrospective Cohort Study. — Deng Y, Chen C, Chen S, et al. BioMed Research International. 2019.
2. Progestogen for Treating Threatened Miscarriage. — Wahabi HA, Fayed AA, Esmaeil SA, Bahkali KH. The Cochrane Database of Systematic Reviews. 2018.
3. Miscarriage Matters: The Epidemiological, Physical, Psychological, and Economic Costs of Early Pregnancy Loss. — Quenby S, Gallos ID, Dhillon-Smith RK, et al. Lancet. 2021.
4. Sporadic Miscarriage: Evidence to Provide Effective Care. — Coomarasamy A, Gallos ID, Papadopoulou A, et al. Lancet. 2021.
5. Signs and Symptoms Associated With Early Pregnancy Loss: Findings From a Population-Based Preconception Cohort. — Sapra KJ, Buck Louis GM, Sundaram R, et al. Human Reproduction. 2016.
6. Threatened Abortion: Prediction of Viability Based on Signs and Symptoms. — Chung TK, Sahota DS, Lau TK, et al. The Australian & New Zealand Journal of Obstetrics & Gynaecology. 1999.
7. ACOG Practice Bulletin No. 200: Early Pregnancy Loss. — Committee on Practice Bulletins—Gynecology Obstetrics and Gynecology. 2018.
8. Predictive Models of Miscarriage on the Basis of Data From a Preconception Cohort Study. — Yland JJ, Zad Z, Wang TR, et al. Fertility and Sterility. 2024.
9. Ectopic Pregnancy. — Barnhart KT. The New England Journal of Medicine. 2009.
10. Spontaneous Abortion. — Boyd ME. Canadian Journal of Surgery. Journal Canadien De Chirurgie. 1989.
11. Does This Woman Have an Ectopic Pregnancy?The Rational Clinical Examination Systematic Review. — Crochet JR, Bastian LA, Chireau MV. The Journal of the American Medical Association. 2013.
12. Complications of Unsafe and Self-Managed Abortion. — Harris LH, Grossman D. The New England Journal of Medicine. 2020.
13. Micronized Vaginal Progesterone to Prevent Miscarriage: A Critical Evaluation of Randomized Evidence. — Coomarasamy A, Devall AJ, Brosens JJ, et al. American Journal of Obstetrics and Gynecology. 2020.
14. Progesterone to Prevent Miscarriage in Women With Early Pregnancy Bleeding: The PRISM RCT. — Coomarasamy A, Harb HM, Devall AJ, et al. Health Technology Assessment. 2020.
15. Progestogens for Preventing Miscarriage: A Network Meta-Analysis. — Devall AJ, Papadopoulou A, Podesek M, et al. The Cochrane Database of Systematic Reviews. 2021.
16. Progesterone for Women With Threatened Miscarriage (STOP Trial): A Placebo-Controlled Randomized Clinical Trial. — McLindon LA, James G, Beckmann MM, et al. Human Reproduction. 2023.
17. First Trimester Bleeding: Evaluation and Management. — Hendriks E, MacNaughton H, MacKenzie MC. American Family Physician. 2019.
18. Use of Oral Progestogen in Women With Threatened Miscarriage in the First Trimester: A Randomized Double-Blind Controlled Trial. — Chan DMK, Cheung KW, Ko JKY, et al. Human Reproduction. 2021.
19. Vitamin Supplementation for Preventing Miscarriage. — Balogun OO, da Silva Lopes K, Ota E, et al. The Cochrane Database of Systematic Reviews. 2016.
20. A Randomized Trial of Progesterone in Women with Bleeding in Early Pregnancy. — Coomarasamy A, Devall AJ, Cheed V, et al. The New England Journal of Medicine. 2019.
21. Combined Oestrogen and Progesterone for Preventing Miscarriage. — Lim CE, Ho KK, Cheng NC, Wong FW. The Cochrane Database of Systematic Reviews. 2013.
22. Cytogenetic signatures of recurrent pregnancy losses. — Yatsenko SA, Quesada-Candela C, Saller DN, et al. Prenatal Diagnosis. 2021.
23. Triage and Care for Women With Symptoms or Diagnosis of Pregnancy Loss Between 14 + 0 and 21 + 6 weeks' Gestation. — Fox CE, Kaur R, Vigneswaran K, et al. International Journal of Gynaecology and Obstetrics: The Official Organ of the International Federation of Gynaecology and Obstetrics. 2025.
24. ACOG Practice Bulletin No. 193: Tubal Ectopic Pregnancy. — Committee on Practice Bulletins—GynecologyThis Practice Bulletin was developed by the Committee on Practice Bulletins—Gynecology in collaboration with Kurt T Obstetrics and Gynecology. 2018.
25. ACR Appropriateness Criteria® Acute Pelvic Pain in the Reproductive Age Group: 2023 Update. — Brook OR, Dadour JR, Robbins JB, et al. Journal of the American College of Radiology : JACR. 2024.
26. A Risk Prediction Model of Spontaneous Miscarriage in Women With Threatened Miscarriage: A Prospective Cohort Study. — Ku CW, Tan YB, Tan MMT, et al. Frontiers in Medicine. 2025.
27. Novel Approach Using Serum Progesterone as a Triage to Guide Management of Patients With Threatened Miscarriage: A Prospective Cohort Study. — Tan TC, Ku CW, Kwek LK, et al. Scientific Reports. 2020.
28. ACR Appropriateness Criteria® First Trimester Vaginal Bleeding: 2025 Update. — Expert Panel on GYN and OB Imaging, Laifer-Narin SL, Fruauff A, et al. Journal of the American College of Radiology : JACR. 2025.