Status Asthmaticus
Status asthmaticus (acute severe asthma) is defined as severe asthma unresponsive to repeated courses of beta-agonist therapy, representing a medical emergency that requires immediate recognition a…
Status asthmaticus (acute severe asthma) is defined as severe asthma unresponsive to repeated courses of beta-agonist therapy, representing a medical emergency that requires immediate recognition and aggressive treatment.[1-2] Approximately 25,000–50,000 patients per year require ICU admission in the United States for life-threatening asthma.[3]
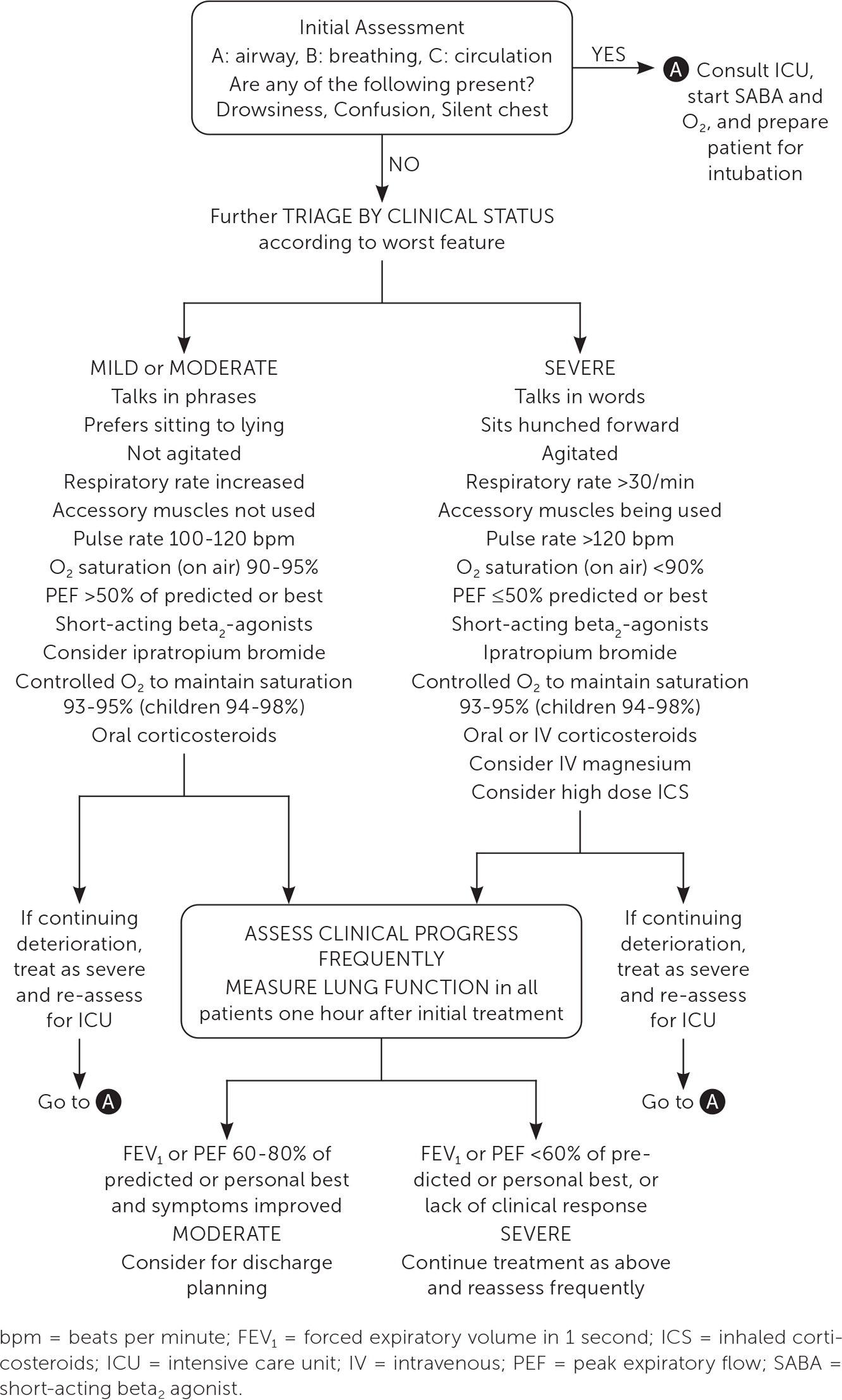
The following figure outlines the acute care management algorithm per GINA guidelines:
View full figure Figure 2. Management of asthma exacerbations in acute care facility, e.g. emergency department. Reprinted with permission from Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. 2023. Accessed June 15, 2023. https://ginasthma.org/wp-content/uploads/2023/07/GINA-2023-Full-report-23_07_06-WMS.pdf Acute Asthma Exacerbations: Management Strategies. Am Fam Physician. December 31, 2023.
1. History
- Onset and progression: Rapid vs. gradual onset (sudden-onset attacks carry higher mortality); duration of current symptoms; what triggered the episode
- Symptom characterization: Dyspnea severity, chest tightness, cough, inability to speak in full sentences, inability to lie flat, air hunger[1][5]
- Current medications: ICS use and adherence, SABA frequency (>8 puffs in prior 24 hours is a red flag), recent OCS use or withdrawal[5-6]
- Asthma morbidity history: Prior intubations, ICU admissions, ED visits, hospitalizations — these are the strongest predictors of asthma-related death[1][5]
- Triggers: Viral URI (~50% of episodes), allergen exposure (pets, mold/Alternaria), NSAID use in aspirin-sensitive patients, irritant inhalation (smoke, paint), exercise, medication nonadherence[1-2]
- Important negatives: Fever, purulent sputum, unilateral symptoms, chest pain, leg swelling, choking episode (to exclude mimics)
2. Alarm Features
- Drowsiness, confusion, or altered mental status — cerebral hypoxemia, impending arrest[5-6]
- Silent chest on auscultation — minimal ventilation, insufficient airflow to generate wheeze[5][7]
- Inability to speak or speak only in single words[1]
- Refusal to recline <30°[1-2]
- SpO₂ <92% on presentation (before treatment) — associated with high morbidity and likely need for hospitalization[6]
- Cyanosis, diaphoresis, accessory muscle use[5]
- Normalizing PaCO₂ in a tachypneic patient — indicates respiratory muscle fatigue and impending failure[7]
- Pulsus paradoxus >25 mmHg[2]
- Failure to respond to initial aggressive bronchodilator therapy[1]
3. Medications
First-line treatments
- Inhaled SABA (albuterol): Adults — 2.5–5 mg nebulized q20min × 3 doses, then 2.5–10 mg q1–4h; or continuous nebulization 10–15 mg/hr. Children — 0.15 mg/kg (min 2.5 mg) q20min × 3[4]
- Ipratropium bromide: 0.5 mg nebulized q20min × 3 doses (adults); 0.25–0.5 mg (children). Reduces ED time and hospitalization rates; benefit not sustained after admission[1][4]
- Systemic corticosteroids: Adults — prednisone/methylprednisolone 40–80 mg/day; children — 1–2 mg/kg/day (max 60 mg). Administer within the first hour; clinical benefit takes 6–12 hours[1][4][8]
- Oxygen: Target SpO₂ 93–95% in adults/adolescents. Avoid excessive O₂ which may worsen hypercapnia[4]
Second-line/adjunctive
- IV magnesium sulfate: 2 g over 20 minutes (adults); modestly reduces hospitalizations in severe exacerbations[4]
- High-dose ICS: ≥2 mg beclomethasone equivalent within the first hour may reduce need for hospitalization[4]
- IM epinephrine: For anaphylaxis-associated asthma or severe refractory cases; adults 0.3–0.5 mg, children 0.01 mg/kg[4]
Refractory/ICU-level therapies
- IV terbutaline or epinephrine for refractory bronchospasm[7][9]
- Ketamine: 0.5–2 mg/kg/h continuous infusion; bronchodilator and anti-inflammatory properties; preferred induction agent if intubation needed. Evidence for routine use is limited[7][10-11]
- Heliox (70:30 or 80:20 He:O₂): Reduces airway resistance; may improve nebulized drug delivery. Not routinely recommended but may be considered as rescue therapy[7]
- Inhaled anesthetics (sevoflurane, isoflurane): Last-line for intubated patients with refractory bronchospasm; requires anesthesiology involvement[7][12]
Medication cautions
- Avoid beta-blockers (including ophthalmic)
- NSAIDs contraindicated in aspirin-exacerbated respiratory disease
- Avoid sedatives/anxiolytics in non-intubated patients (risk of respiratory depression)
- Prolonged neuromuscular blockade + corticosteroids → risk of critical illness myopathy[13]
4. Diet
- NPO if severe/critical and intubation is possible
- Hydration: Many patients are dehydrated from tachypnea, diaphoresis, and poor oral intake; IV fluid resuscitation is important, especially before positive-pressure ventilation (risk of hypotension)[14]
- Long-term: Identify and avoid known food allergens (food allergy is a risk factor for asthma-related death); sulfite-containing foods/beverages may trigger bronchospasm in susceptible individuals[5]
5. Review of Systems
- Pulmonary: Cough, wheeze, dyspnea, sputum production, hemoptysis
- Cardiac: Chest pain, palpitations (beta-agonist effects, consider PE or cardiac mimics)
- ENT: Nasal congestion, postnasal drip, sore throat (URI trigger, vocal cord dysfunction)
- GI: GERD symptoms (trigger for asthma)
- Psychiatric: Anxiety, panic (both a mimic and comorbidity)
- Allergic/Immunologic: Recent allergen exposures, anaphylaxis symptoms (urticaria, angioedema)
6. Collateral History and Family History
- Collateral: Confirm medication adherence, actual inhaler technique, home nebulizer use, recent controller changes, prior action plan compliance
- Family history: Asthma, atopy, eczema, allergic rhinitis, sudden cardiac death
- Social context: Smoking/vaping, secondhand smoke, occupational exposures, illicit drug use (cocaine can cause bronchospasm), housing conditions (mold, pests), psychiatric disorders, dysfunctional family settings in children — all risk factors for asthma-related death[5]
7. Risk Factors
Risk factors for asthma-related death
- Prior intubation or ICU admission for asthma
- ≥2 hospitalizations or ≥3 ED visits in the past year
- SABA overuse (>1 canister/month)
- Poor adherence to or absence of ICS therapy
- Recent OCS withdrawal
- Food allergy in an atopic individual
- Psychiatric disorders, illicit drug use
- Low socioeconomic status, limited healthcare access
Common triggers
- Viral respiratory infections (~50%)
- Allergen exposure (pets, mold, dust mites, pollen)
- NSAID/aspirin in sensitive patients
- Irritant inhalation (smoke, chemicals)
- Exercise, cold air
- Medication nonadherence
8. Differential Diagnosis
- Anaphylaxis — urticaria, angioedema, hypotension; administer epinephrine
- Vocal cord dysfunction (VCD) — inspiratory stridor, flattened inspiratory loop on flow-volume curve
- Foreign body aspiration — sudden onset, unilateral wheeze, especially in children
- Pulmonary embolism — pleuritic chest pain, risk factors, unilateral leg swelling
- Pneumothorax/tension pneumothorax — sudden pleuritic pain, unilateral absent breath sounds; critical in mechanically ventilated patients[15]
- Decompensated heart failure/pulmonary edema — "cardiac asthma," orthopnea, JVD, crackles
- COPD exacerbation — older patients, smoking history
- Pneumonia/lower respiratory tract infection — fever, productive cough, focal findings
- Epiglottitis/upper airway obstruction — stridor, drooling, toxic appearance
- Hyperventilation syndrome/panic attack — perioral/extremity paresthesias, normal SpO₂[5]
9. Past Medical History
- Prior asthma severity: Frequency of exacerbations, prior intubations, ICU admissions, near-fatal episodes
- Comorbidities: Allergic rhinitis, nasal polyps, GERD, obesity, OSA, eczema, aspirin-exacerbated respiratory disease
- Surgical history: Prior ENT surgery (polyps), prior tracheostomy
- Chronic medications: Current controller regimen, biologic therapy, OCS dependence
10. Physical Exam
Vital signs
- Tachypnea (RR >30 in adults), tachycardia (HR >120), SpO₂ <92%, pulsus paradoxus >12 mmHg (>25 mmHg = severe)[1-2]
Focused exam
- General: Tripod positioning, inability to speak in sentences, diaphoresis, agitation vs. obtundation
- Lungs: Diffuse expiratory wheezing → progressing to silent chest (ominous); prolonged expiratory phase; air trapping[5][7]
- Accessory muscles: SCM, intercostal, subcostal, supraclavicular retractions[1]
- Cardiac: Tachycardia, assess for pulsus paradoxus
- Skin: Cyanosis (late finding), urticaria/angioedema (anaphylaxis)
- ENT: Nasal polyps, nasal congestion, oropharyngeal edema
11. Lab Studies
- ABG/VBG: Not routine; obtain if SpO₂ <90–92% or signs of severe exacerbation. Expect initial respiratory alkalosis → normalizing or rising PaCO₂ is ominous (muscle fatigue) → respiratory/metabolic acidosis in severe cases[5][7]
- Basic metabolic panel: Hypokalemia (from beta-agonists and corticosteroids), hyperglycemia
- Lactate: May be elevated from respiratory distress and beta-agonist use
- Troponin: Consider in adults with chest pain or cardiac risk factors; may be elevated in children on continuous albuterol (24% in one study)[16]
- CBC: Leukocytosis may be from steroids or stress; eosinophilia suggests allergic component
- Magnesium level: Check before/after IV magnesium
- Blood gas monitoring: Serial if intubated or critically ill
12. Imaging
- Chest X-ray: Not routinely recommended in uncomplicated exacerbations. Obtain if:[4-5]
- Suspected pneumothorax, pneumomediastinum
- Fever or focal findings suggesting pneumonia
- Foreign body concern
- Failure to respond to treatment
- Subcutaneous emphysema on exam
- Expected findings: Hyperinflation, flattened diaphragms, peribronchial thickening
- Concerning findings: Pneumothorax, pneumomediastinum, lobar consolidation, atelectasis from mucus plugging
- CT chest: Rarely needed acutely; consider for PE (CTA) or if alternative diagnosis suspected
13. Special Tests
- Peak expiratory flow (PEF) / FEV₁: Objective severity assessment; more reliable than symptoms. Pre-treatment <25% predicted → hospitalization recommended; post-treatment >60% predicted → consider discharge[6][17]
- Pediatric Asthma Score (PAS): Bedside scoring tool for children 2–18 years assessing RR, O₂ requirements, auscultation, retractions, and dyspnea (score 5–15)[6]
- PRAM and PASS scores: Validated for pediatric exacerbation severity[6]
- Point-of-care ultrasound: Assess for pneumothorax (absent lung sliding), pleural effusion, cardiac function (RV strain)
- Capnography (ETCO₂): Useful for monitoring ventilation trends; rising ETCO₂ suggests worsening obstruction
14. ECG
- Indications: Obtain in severe exacerbations, patients on continuous albuterol, cardiac symptoms, or ICU-level care.
Common findings
- Sinus tachycardia — most common; beta-agonist effect and sympathetic drive
- Right axis deviation, P pulmonale (peaked P waves in II, III, aVF) — from acute RV strain/pulmonary hyperinflation[19]
- Low voltage QRS — from hyperinflation
- ST-segment depression/T-wave inversions (especially inferior leads) — seen in 30% of children on continuous albuterol; correlates with severity; usually reversible[16][20]
- Premature ventricular contractions (PVCs) — more common with beta-agonist use[18]
- SVT — rare but reported with high-dose SABA, especially in children[21]
- QTc prolongation — monitor with hypokalemia and high-dose beta-agonists
- Dangerous patterns: New arrhythmia, wide-complex tachycardia, ST elevation (consider tension pneumothorax, myocardial ischemia)
15. Assessment
Severity stratification
Export Feature Mild-Moderate Severe Life-Threatening Speech Sentences Words/phrases Unable to speak Position Can lie flat Prefers sitting upright Tripod/unable to recline Mental status Alert Agitated Drowsy/confused RR (adult) Increased >30/min Bradypnea (ominous) HR 120 >120 Bradycardia (ominous) SpO₂ >95% 90–95% 90% PEF >50% predicted 25–50% predicted 25% predicted Auscultation Wheeze Loud wheeze Silent chest References[1-2]
- A normalizing PaCO₂ in a tachypneic patient indicates impending respiratory failure[7]
- Clinical status and lung function 1 hour after treatment are more reliable predictors of outcome than status on arrival[6][17]
- Complications: pneumothorax, pneumomediastinum, atelectasis from mucus plugging, respiratory arrest, cardiac arrest from hypoxia/hyperinflation
16. Treatment Plan
Initial stabilization (first 60 minutes)
- Continuous albuterol nebulization (10–15 mg/hr) or MDI 4–10 puffs q20min × 3
- Ipratropium 0.5 mg nebulized q20min × 3 doses
- Systemic corticosteroids within the first hour (prednisone 40–80 mg PO or methylprednisolone 125 mg IV)
- Oxygen to target SpO₂ 93–95%
- IV magnesium sulfate 2 g over 20 minutes if severe/refractory[4][8]
Escalation for refractory cases
- IV access, continuous monitoring, IV fluids (anticipate dehydration)[14]
- IV terbutaline or epinephrine drip[7]
- Heliox-driven nebulization if available[7]
- NIV (BiPAP): May reduce need for intubation; use in cooperative patients[3][22]
- Ketamine infusion: 0.5–2 mg/kg/h; consider for sedation and bronchodilation[7][11]
If intubation required
- Induction: Ketamine (1–2 mg/kg IV) preferred for bronchodilatory properties; avoid histamine-releasing agents
- Paralysis: Succinylcholine or rocuronium
- Ventilator strategy: Permissive hypercapnia is standard
- Low RR (8–12 breaths/min), Vt 6–8 mL/kg
- Prolonged expiratory time (I:E ratio ≥1:3–1:4)
- Low PEEP (titrate to intrinsic PEEP)
- Plateau pressure <25–30 cmH₂O, peak pressure <40 cmH₂O
- Tolerate pH >7.2 and elevated PaCO₂
- Sedation: Ketamine or propofol (both have bronchodilatory properties)[3]
- Neuromuscular blockade: Use sparingly; risk of critical illness myopathy with concurrent steroids[13]
- Last-line: Inhaled anesthetics (sevoflurane/isoflurane), ECMO for refractory respiratory failure (survival 83.5–100%)[7][15]
17. Disposition
ICU admission criteria
- Drowsiness, confusion, or silent chest
- Requiring intubation or NIV
- Persistent hypoxia (SpO₂ <90%) despite treatment
- Worsening or no improvement after 1–2 hours of aggressive therapy
- Hemodynamic instability
- Need for continuous IV bronchodilators
Hospital admission criteria
- Pre-treatment FEV₁/PEF <25% predicted
- Post-treatment FEV₁/PEF <40% predicted
- Persistent oxygen requirement
- Inadequate response to bronchodilators after 1–3 hours
- Prior intubation or recent hospitalization for asthma
- 8 SABA puffs in prior 24 hours
Discharge criteria
- Symptom improvement with sustained response
- Post-treatment FEV₁/PEF >60% predicted
- SpO₂ >94% on room air
- Able to tolerate oral medications
- Adequate social support and follow-up access
- Specialist consultation triggers: Pulmonology, allergy/immunology for recurrent severe exacerbations; anesthesiology for inhaled anesthetics; surgery/ECMO team for refractory cases
18. Follow Up / Return Precautions
Follow-up timing
- Adults/adolescents: 2–7 days after ED discharge[4]
- Children: 1–2 working days[4]
- Post-hospitalization: Within 1 week; reassess at 1–3 months
Discharge prescriptions
- OCS: Prednisone 40–50 mg/day × 5–7 days (adults); 1–2 mg/kg/day × 3–5 days (children)[4][8]
- Initiate or step up ICS before discharge[4]
- Ensure rescue inhaler with spacer
- Provide written asthma action plan
- Return precautions — instruct patients to seek immediate care for:
- Worsening shortness of breath or inability to speak
- No improvement with rescue inhaler
- Chest pain or palpitations
- Confusion, drowsiness, or blue lips
- Fever with worsening respiratory symptoms
Patient counseling
- Medication adherence (ICS is the cornerstone of prevention)
- Proper inhaler technique
- Allergen avoidance and trigger identification
- Smoking/vaping cessation
- Ensure follow-up with PCP and/or specialist for long-term asthma management and step-up therapy evaluation[4]
References
1. Acute Severe Asthma (Status Asthmaticus). — Agnihotri NT, Saltoun C. Allergy and Asthma Proceedings. 2019.
2. Chapter 14: Acute Severe Asthma (Status Asthmaticus). — Shah R, Saltoun CA. Allergy and Asthma Proceedings. 2012.
3. Management of Life-Threatening Asthma: Severe Asthma Series. — Garner O, Ramey JS, Hanania NA. Chest. 2022.
4. Acute Asthma Exacerbations: Management Strategies. — Dabbs W, Bradley MH, Chamberlin SM. American Family Physician. 2024.
5. Asthma. — Papi A, Brightling C, Pedersen SE, Reddel HK. Lancet. 2018.
6. 2025 Global Strategy for Asthma Management and Prevention. — Helen Reddel, Eric Bateman, Gerard FitzGerald, et al Global Initiative for Asthma. 2025.
7. ATS Pediatric Core Curriculum 2024: The Role of the Pediatric Pulmonologist in the Intensive Care Unit. — Leon-Astudillo C, Prero MY, Dy FJ, et al. Pediatric Pulmonology. 2025.
8. 2024 Summary Guide for Asthma Management and Prevention. — Helen Reddel, Arzu Yorgancioglu, Mark L. Levy, Rebecca Decker, Kristi Ruey Global Initiative for Asthma. 2024.
9. Pharmacological Management of Pediatric Critical Asthma. — Rogerson CM, White BR, Abu-Sultaneh S. Respiratory Care. 2025.
10. Use of Ketamine in Patients With Refractory Severe Asthma Exacerbations: Systematic Review of Prospective Studies. — La Via L, Sanfilippo F, Cuttone G, et al. European Journal of Clinical Pharmacology. 2022.
11. Use of Ketamine in Asthmatic Children to Treat Respiratory Failure Refractory to Conventional Therapy. — Rock MJ, Reyes de la Rocha S, L'Hommedieu CS, Truemper E. Critical Care Medicine. 1986.
12. Severe Status Asthmaticus: Management With Permissive Hypercapnia and Inhalation Anesthesia. — Mutlu GM, Factor P, Schwartz DE, Sznajder JI. Critical Care Medicine. 2002.
13. The Assessment and Management of Adults With Status Asthmaticus. — Corbridge TC, Hall JB. American Journal of Respiratory and Critical Care Medicine. 1995.
14. Evaluation and Management of the Critically Ill Adult Asthmatic in the Emergency Department Setting. — Long B, Lentz S, Koyfman A, Gottlieb M. The American Journal of Emergency Medicine. 2021.
15. Part 10: Adult and Pediatric Special Circumstances of Resuscitation: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Cao D, Arens AM, Chow SL, et al. Circulation. 2025.
16. Diastolic Hypotension, Troponin Elevation, and Electrocardiographic Changes Associated With the Management of Moderate to Severe Asthma in Children. — Fagbuyi DB, Venkataraman S, Ralphe JC, et al. Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine. 2016.
17. 2023 GINA Report, Global Strategy for Asthma Management and Prevention. — Helen K. Reddel, Leonard B. Bacharier, Eric D. Bateman, et al Global Initiative for Asthma. 2023.
18. Cardiac Arrhythmias in Adult Patients With Asthma. — Warnier MJ, Rutten FH, Kors JA, et al. The Journal of Asthma : Official Journal of the Association for the Care of Asthma. 2012.
19. Reversible Electrocardiographic Changes in Severe Acute Asthma. — Siegler D. Thorax. 1977.
20. Reversible T-Wave Abnormality in Severe Acute Asthma: An Electrocardiographic Sign of Severity. — Efthimiou J, Hassan AB, Ormerod O, Benson MK. Respiratory Medicine. 1991.
21. Supraventricular tachycardia diagnosis in asthma patients is associated with adverse health outcomes. — Markus H, Ceneviva GD, Thomas NJ, Krawiec C. Pediatric Pulmonology. 2024.
22. Emergency Treatment of Asthma. — Lazarus SC. The New England Journal of Medicine. 2010.
23. Mechanical Ventilation for Severe Asthma. — Leatherman J. Chest. 2015.
24. Invasive Respiratory Support in Critical Pediatric Asthma. — Newth CJL, Ross PA. Respiratory Care. 2025.