Subdural Hematoma
1. History
1. History
- Mechanism of injury: Falls (most common in elderly), MVCs, assaults, ground-level falls; in chronic SDH, trauma may be trivial or absent[1-2]
- Timing: Acute SDH presents within hours of injury; chronic SDH may develop weeks to months after initial trauma, often with an insidious course[1][3]
- Headache characterization: Acute-onset headache is the most common symptom in spontaneous ASDH (87%); chronic SDH presents with progressive headache, cognitive decline, or personality changes[1][4]
- Symptom progression: Ask about worsening confusion, increasing drowsiness, progressive weakness, speech difficulty, gait instability[1-2]
- Lucid interval: Classic "talk and deteriorate" pattern — initial alertness followed by neurologic decline suggests expanding hematoma
- Anticoagulant/antiplatelet use: Type, dose, and time of last dose are critical[5-6]
- Important negatives: Absence of trauma history does not exclude SDH — spontaneous SDH accounts for ~5% of acute cases; ask about CSF leak symptoms (positional headache suggesting intracranial hypotension)[4][7]
2. Alarm Features
- GCS decline ≥2 points from baseline or any decline after initial assessment[8-9]
- Pupillary asymmetry (anisocoria) or fixed/dilated pupil — suggests uncal herniation[9]
- Rapid neurologic deterioration: New hemiparesis, aphasia, or obtundation
- Cushing triad: Hypertension, bradycardia, irregular respirations (late sign of herniation)
- Seizures or status epilepticus — occurs in up to 41% of acute SDH patients[10]
- Vomiting (especially repeated) — posttest probability of intracranial injury rises to ~21% with ≥2 episodes after minor head trauma[8]
- Signs of basilar skull fracture: Battle sign, raccoon eyes, hemotympanum, CSF otorrhea/rhinorrhea[8]
3. Medications
Contributing medications
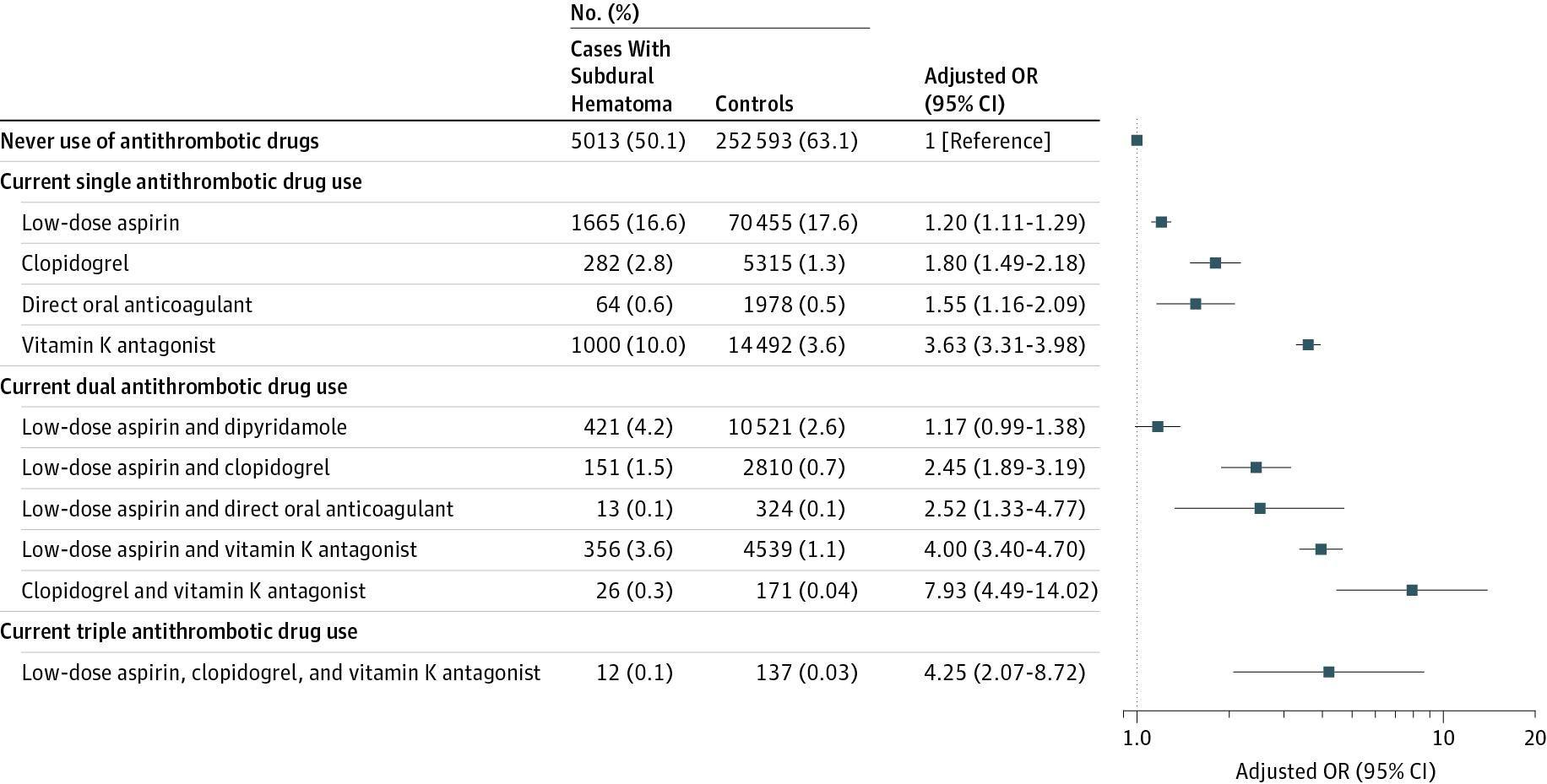
- Warfarin (VKA): Highest risk, especially with INR ≥1.4; OR ~3–4 for SDH as monotherapy[11]
- DOACs (apixaban, rivaroxaban, dabigatran): Lower risk than warfarin but still significant[1]
- Antiplatelet agents: Aspirin, clopidogrel; combination antithrombotic therapy dramatically increases risk (VKA + clopidogrel: OR ~8)[11]
- SSRIs, valproic acid (platelet dysfunction)
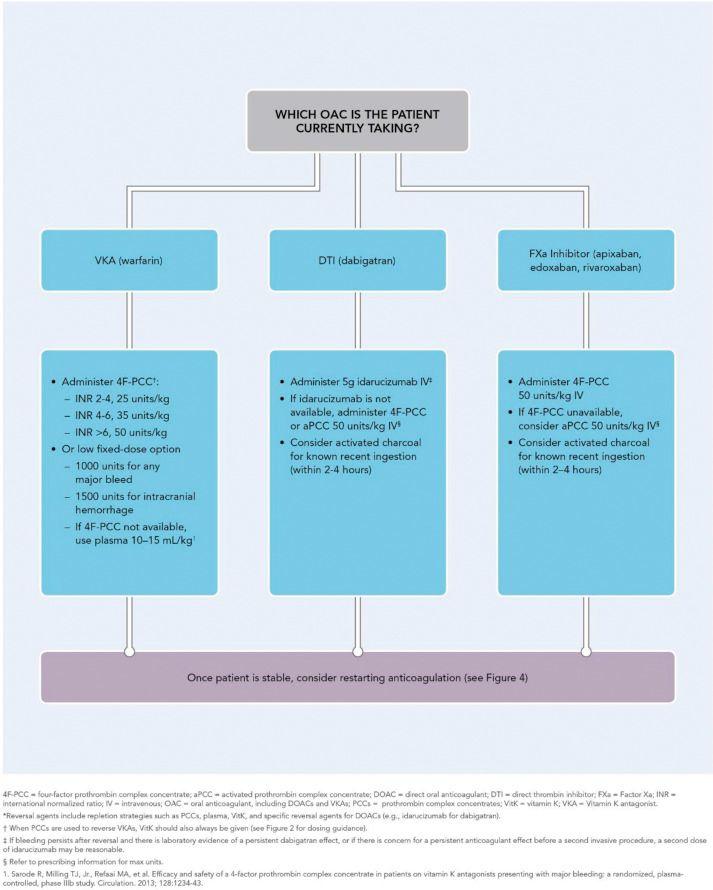
- Reversal strategies (per AHA/ASA 2022 and ACS 2024 guidelines):[5][12-13]
- Warfarin: 4-factor PCC (weight-based; lower dose 10–20 IU/kg if INR <2.0) + IV vitamin K 5–10 mg
- Factor Xa inhibitors (apixaban, rivaroxaban): 4-factor PCC or aPCC (note: andexanet alfa was withdrawn from the US market)[14]
- Dabigatran: Idarucizumab 5 g IV (two 2.5 g boluses); if unavailable, PCC/aPCC ± hemodialysis[13]
- Heparin/LMWH: Protamine sulfate[13]
- Antiplatelets: Routine platelet transfusion is not recommended; desmopressin (DDAVP) may be considered[15]
Seizure prophylaxis
- Levetiracetam preferred over phenytoin (similar efficacy, fewer adverse effects) for acute SDH[16]
- 7 days of prophylaxis is standard for acute traumatic SDH per Brain Trauma Foundation guidelines[5]
- Prophylaxis for chronic SDH remains controversial and is not clearly beneficial[17]
4. Diet
- NPO if surgical intervention anticipated or GCS declining
- Maintain euvolemia; avoid hypotonic fluids (risk of cerebral edema)
- Long-term: No specific dietary triggers; ensure adequate nutrition during recovery, especially in elderly patients at risk of malnutrition
5. Review of Systems
- Neurologic: Headache, confusion, memory loss, speech changes, visual changes, weakness, numbness, gait difficulty, seizures
- Constitutional: Fatigue, lethargy, personality changes (especially chronic SDH)
- GI: Nausea/vomiting (raised ICP)
- Urologic: Incontinence (frontal lobe compression)
- Psychiatric: Behavioral changes, apathy, depression (chronic SDH can mimic dementia)
6. Collateral History and Family History
- Collateral: Witnessed fall or trauma? Timeline of symptom onset? Baseline cognitive function? Medication compliance (especially anticoagulants)?
- Elder abuse screening: SDH without adequate trauma history in elderly patients should prompt consideration of non-accidental injury[18]
- Child abuse: In pediatric patients, SDH (especially bilateral, multi-aged) is a hallmark of abusive head trauma[18]
- Family history: Connective tissue disorders (Ehlers-Danlos), polycystic kidney disease, cerebral amyloid angiopathy, bleeding disorders[19]
- Social: Alcohol use (brain atrophy, coagulopathy, fall risk), living situation, fall hazards
7. Risk Factors
- Age >65 years — most significant risk factor; incidence has tripled since 1990 in elderly[1]
- Antithrombotic therapy — dose-dependent risk; combination therapy markedly increases risk[11]
- Brain atrophy — stretches bridging veins (alcohol use, advanced age, neurodegenerative disease)
- Cerebral amyloid angiopathy (CAA) — independent risk factor for nontraumatic SDH[20]
- Coagulopathy: Liver disease, renal disease, hematologic malignancy, DIC[1]
- CSF shunting or lumbar puncture — intracranial hypotension[7]
- Prior SDH — recurrence rate 10–20% after surgical evacuation[2][21]
- Seizure disorders (fall risk)
8. Differential Diagnosis
Cannot-miss diagnoses
- Epidural hematoma — biconvex/lenticular shape on CT; often associated with temporal bone fracture and middle meningeal artery injury
- Subarachnoid hemorrhage — thunderclap headache; blood in cisterns/sulci on CT
- Ruptured intracranial aneurysm presenting as SDH (rare but reported)[19]
- Stroke (ischemic or hemorrhagic) — acute focal deficits
Important mimics
- Subdural empyema/abscess — fever, meningismus
- Subdural metastases or lymphoma — progressive headache without trauma; hyperdense on CT but hyperintense on T2 MRI[22-23]
- Subdural hygroma — CSF-density collection, often post-traumatic
- Spontaneous intracranial hypotension — bilateral SDH in younger patients with positional headache[7]
- Dementia — chronic SDH can mimic or exacerbate cognitive decline[1]
9. Past Medical History
- Prior head trauma or SDH (recurrence risk)
- Anticoagulation indication (atrial fibrillation, mechanical valve, VTE)
- Liver/renal disease (coagulopathy)
- Alcohol use disorder
- Seizure history
- Prior neurosurgery or CSF shunt
- Falls history and mobility status
10. Physical Exam
Vital signs
- Hypertension with bradycardia (Cushing response — late, ominous)
- Assess for hypotension/tachycardia (polytrauma)
Focused neurologic exam
- GCS — serial assessments are essential; decline ≥2 points is an alarm feature[8-9]
- Pupils: Size, reactivity, symmetry — anisocoria suggests ipsilateral uncal herniation
- Motor exam: Hemiparesis (contralateral or ipsilateral via Kernohan notch phenomenon)
- Speech/language: Aphasia, dysarthria
- Gait: Instability, ataxia (common in chronic SDH)[1]
- Scalp: Palpate for depressed fracture, lacerations, hematoma
- Signs of basilar skull fracture: Battle sign, raccoon eyes, hemotympanum[8]
11. Lab Studies
- CBC with platelets
- Coagulation panel: PT/INR, aPTT
- BMP (electrolytes, renal function — relevant for DOAC clearance)
- Type and screen (if surgery anticipated)
- Drug-specific anti-Xa level or thrombin time if on DOACs and timing of last dose is uncertain[5][12]
- Hepatic function panel if coagulopathy suspected
- Blood alcohol level and urine drug screen (altered mental status workup, fall etiology)
- Lactate if concern for shock or polytrauma
12. Imaging
- First-line: Non-contrast CT head[24]
- Acute SDH: Hyperdense crescent-shaped collection along cerebral convexity; crosses suture lines but not the midline falx
- Subacute SDH (1–3 weeks): Isodense to brain — may be difficult to detect; look for effacement of sulci, midline shift, or mass effect
- Chronic SDH (>3 weeks): Hypodense collection; may have mixed density with rebleeding (acute-on-chronic)
- Measure maximum thickness and midline shift — these are the strongest radiographic predictors of need for intervention[25]
Additional imaging
- CTA: If spontaneous SDH without clear trauma — evaluate for aneurysm, vascular malformation, or dural metastases[4][19]
- MRI brain: Superior for detecting subacute/isodense SDH, underlying parenchymal injury, tumor, and aging blood products[18][24]
- Repeat CT within 6 hours for conservatively managed patients to assess for expansion[26-27]
When imaging may be unnecessary
- Asymptomatic patients with known stable chronic SDH on serial imaging and no change in clinical status
13. Special Tests
Decision rules for imaging after minor head trauma
- Canadian CT Head Rule and New Orleans Criteria — validated tools to determine need for CT[8]
- Age >65, vomiting ≥2 episodes, GCS <15 at 2 hours, signs of skull fracture, anticoagulant use, and dangerous mechanism all warrant CT[8]
Scoring systems
- GCS — serial monitoring; GCS <9 defines coma and triggers ICP monitoring consideration[9]
- Markwalder Grading Scale — used for chronic SDH severity (Grade 0: asymptomatic → Grade 4: comatose)[28]
- Modified Rankin Scale (mRS) — functional outcome assessment
Point-of-care
- Bedside ultrasound: Optic nerve sheath diameter >5 mm suggests elevated ICP (adjunct, not definitive)
14. ECG
- ECG is not a primary diagnostic tool for SDH but should be obtained in:
- Elderly patients (evaluate for atrial fibrillation — indication for anticoagulation contributing to SDH)
- Syncope as presenting complaint (rule out cardiac arrhythmia as cause of fall)
- Patients with Cushing response (bradycardia)
- Intracranial pathology can cause ECG changes: ST-segment changes, T-wave inversions, QT prolongation, and arrhythmias (neurogenic cardiac effects)
15. Assessment
Classification by timing
- Acute (<3 days): Usually traumatic, high mortality (40–60% in comatose patients); most common focal lesion in TBI[29-30]
- Subacute (3–21 days): Transitional; isodense on CT, easily missed
- Chronic (>21 days): Incidence 2–21 per 100,000; rising rapidly in elderly; projected to become the most common cranial neurosurgical condition by 2030[1-2]
Severity stratification
- Mild: GCS 13–15, thin SDH (<10 mm), no midline shift — often managed conservatively[25]
- Moderate: Neurologic symptoms with moderate hematoma; close monitoring ± surgery
- Severe: GCS <9, thickness >10 mm, midline shift >5 mm, pupillary abnormalities — surgical emergency[9]
Complications
- Herniation (uncal, transtentorial)
- Seizures/status epilepticus (up to 41% in acute SDH; 10% in chronic SDH)[10][16]
- Rebleeding/recurrence (10–20% after surgical evacuation)[2][21]
- Posttraumatic epilepsy (cumulative 2-year incidence up to 40% after SDH)[31]
- Hydrocephalus
16. Treatment Plan
Initial stabilization (all patients)
- ABCs; intubate if GCS ≤8 or airway compromise
- Elevate head of bed to 30°[27]
- Maintain SBP <160 mmHg; avoid hypotension (MAP goal >80 mmHg)
- Maintain normothermia
- Reverse anticoagulation immediately (see Medications section)[5][12-13]
- Seizure prophylaxis with levetiracetam for 7 days (acute traumatic SDH)[5][16]
- Acute SDH — Surgical indications (Brain Trauma Foundation 2006):[9]
- SDH thickness >10 mm or midline shift >5 mm → surgical evacuation regardless of GCS
- Comatose patient (GCS <9) with SDH <10 mm and MLS <5 mm → surgery if GCS drops ≥2 points, asymmetric/fixed pupils, or ICP >20 mmHg
- Timing: Operate as soon as possible; mortality increases significantly if delayed >4 hours[32]
- Technique: Large frontotemporoparietal craniotomy ± decompressive craniectomy[5]
Acute SDH — Conservative management
- Appropriate for small SDH with minimal mass effect and GCS 13–15[29-30]
- Serial neurologic exams and repeat CT within 6 hours[26-27]
- ICU or step-down monitoring
Chronic SDH — Treatment
- Burr-hole drainage with subdural drain placement is the standard of care[21][33-34]
- Drain placement reduces recurrence (RR 0.46)[21][33]
- Irrigation during burr-hole drainage was shown to be non-inferior when omitted (FINISH trial)[34]
- Dexamethasone as stand-alone therapy was found inferior to surgery in the Dutch cSDH trial (NEJM 2023); the Dex-CSDH trial (NEJM 2020) showed dexamethasone resulted in fewer favorable outcomes and more adverse events than placebo when most patients also had surgery[2][28]
- Middle meningeal artery (MMA) embolization: Emerging adjunctive therapy
- SNIS 2026 recommends MMA embolization as adjunct to surgical drainage to decrease recurrence (Class I, Level A)[35]
- EMBOLISE trial (NEJM 2024) and EMMA-Can trial (JAMA 2026) demonstrated reduced recurrence with liquid embolic agents[36-37]
- EMPROTECT trial (JAMA 2025) using microparticles did not reach statistical significance[38]
- Standalone MMA embolization is reasonable in high-risk surgical patients[35]
17. Disposition
Admission criteria
- All acute SDH — ICU or neurosurgical step-down
- Chronic SDH with neurologic symptoms, significant mass effect, or need for surgical intervention
- Any patient on anticoagulation with intracranial hemorrhage
- GCS <15 or any neurologic deficit
- Inability to perform reliable serial neurologic exams (intoxication, sedation)[26]
Observation indications
- Small, minimally symptomatic chronic SDH in a reliable patient — may observe with close outpatient follow-up and repeat imaging in 1–2 weeks
Discharge criteria (chronic SDH, post-surgical)
- Neurologically stable or improved
- Adequate pain control
- Anticoagulation plan established
- Reliable follow-up arranged
Specialist consultation triggers
- Neurosurgery: All SDH — emergent for acute SDH with surgical indications; urgent for symptomatic chronic SDH
- Neurointerventional radiology: For MMA embolization consideration in chronic/recurrent SDH[35]
- Hematology: Complex coagulopathy management
- Geriatrics/social work: Fall prevention, elder abuse screening[18]
18. Follow Up / Return Precautions
Follow-up timing
- Post-surgical: Neurosurgery follow-up in 2 weeks with repeat CT[8][28]
- Conservatively managed: Repeat imaging at 1–2 weeks, then 4–6 weeks, then as clinically indicated
- Chronic SDH may take months to fully resolve radiographically
- Return precautions — instruct patients/families to return immediately for:
- Worsening headache, new or worsening confusion, excessive drowsiness
- Weakness or numbness on one side, difficulty speaking
- Seizures
- Repeated vomiting
- Vision changes
- Gait instability or falls[3]
Patient counseling
- Avoid contact sports and high-risk activities until cleared
- Hold anticoagulation per neurosurgical guidance; restart timing is individualized (typically 1–4 weeks post-injury/surgery depending on indication and risk)
- Avoid alcohol
- Fall prevention measures in elderly (home safety assessment, physical therapy)
Expected recovery
- Chronic SDH: ~57–75% achieve good functional recovery after treatment[4][33]
- Acute SDH: Prognosis depends heavily on GCS at presentation and age; mortality 40–60% in comatose patients; better outcomes with early surgery[32][39]
- Recurrence risk: ~10% after surgical evacuation of chronic SDH; MMA embolization may reduce this[21][35][40]
- Relevant images 3 items
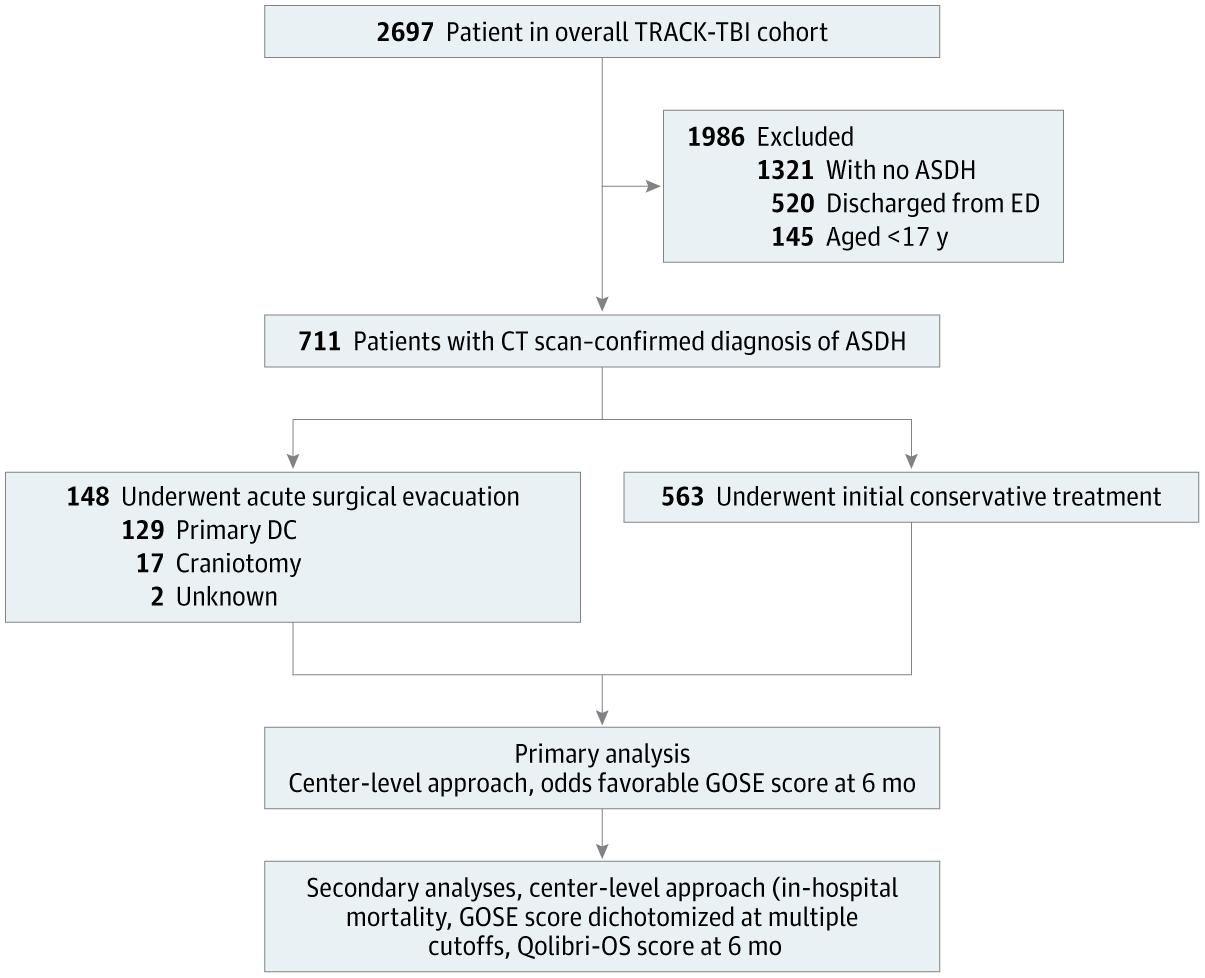
- Flow Diagram of Study Population and Data Analyses
- JAMA Netw Open September 30, 2025
- Current Use of Antithrombotic Drugs and Risk of Subdural Hematoma
- JAMA February 27, 2017
- Guidance for Administering Reversal Agents*
- JACC December 18, 2017
References
1. Chronic Subdural Hematoma: A Review of Current Knowledge, Treatment Modalities, and Clinical Trials of Middle Meningeal Artery Embolization. — Chen H, Colasurdo M, Bodanapally UK, Malhotra A, Gandhi D. Neurology. Clinical Practice. 2025.
2. Trial of Dexamethasone for Chronic Subdural Hematoma. — Hutchinson PJ, Edlmann E, Bulters D, et al. The New England Journal of Medicine. 2020.
3. Action Collaborative on Traumatic Brain Injury Care: Adapted Clinical Practice Guideline. — Silverberg ND, Lee K, Mikolić A, et al. Annals of Family Medicine. 2025.
4. Spontaneous Acute Subdural Hematoma: Etiologic Spectrum, Diagnostic Approach, and Clinical Correlates. — Gabay S, Bergman L, Niry D, et al. Clinical Neurology and Neurosurgery. 2026.
5. Best Practices In The Management Of Traumatic Brain Injury. — Geoffrey T. Manley MD PhD, Gregory W. Albert MD MPH FAANS FACS FAAP, Gretchen M. Brophy PharmD BCPS FCCP FCCM FNCS MCCM, et al American College of Surgeons (2024). 2024.
6. Coagulopathy and Haemorrhagic Progression in Traumatic Brain Injury: Advances in Mechanisms, Diagnosis, and Management. — Maegele M, Schöchl H, Menovsky T, et al. The Lancet. Neurology. 2017.
7. Spontaneous Intracranial Hypotension: Searching for the CSF Leak. — Dobrocky T, Nicholson P, Häni L, et al. The Lancet. Neurology. 2022.
8. Will Neuroimaging Reveal a Severe Intracranial Injury in This Adult With Minor Head Trauma?The Rational Clinical Examination Systematic Review. — Easter JS, Haukoos JS, Meehan WP, Novack V, Edlow JA. The Journal of the American Medical Association. 2015.
9. Surgical Management of Acute Subdural Hematomas. — Bullock MR, Chesnut R, Ghajar J, et al. Neurosurgery. 2006.
10. Seizures and Epileptiform Discharges in Patients With Acute Subdural Hematoma. — Pollandt S, Ouyang B, Bleck TP, Busl KM. Journal of Clinical Neurophysiology : Official Publication of the American Electroencephalographic Society. 2017.
11. Association of Antithrombotic Drug Use With Subdural Hematoma Risk. — Gaist D, García Rodríguez LA, Hellfritzsch M, et al. The Journal of the American Medical Association. 2017.
12. 2024 AHA/ASA Performance and Quality Measures for Spontaneous Intracerebral Hemorrhage: A Report From the American Heart Association/American Stroke Association. — Ruff IM, de Havenon A, Bergman DL, et al. Stroke. 2024.
13. 2022 Guideline for the Management of Patients With Spontaneous Intracerebral Hemorrhage: A Guideline From the American Heart Association/American Stroke Association. — Greenberg SM, Ziai WC, Cordonnier C, et al. Stroke. 2022.
14. FDA Orange Book. — FDA Orange Book. 2026.
15. Unique Considerations in the Assessment and Management of Traumatic Brain Injury in Older Adults. — Depreitere B, Becker C, Ganau M, et al. The Lancet. Neurology. 2025.
16. A Systematic Review of Epileptic Seizures in Adults With Subdural Haematomas. — Won SY, Konczalla J, Dubinski D, et al. Seizure. 2017.
17. Efficacy of Antiseizure Prophylaxis in Chronic Subdural Hematoma: A Cohort Study on Routinely Collected Health Data. — Lavergne P, Labidi M, Brunet MC, et al. Journal of Neurosurgery. 2020.
18. Best Practices Guidelines for Trauma Center Recognition of Child Abuse, Elder Abuse, and Intimate Partner Violence. — Christine S. Cocanour MD FACS FCCM, Randall S. Burd MD PhD FACS, James W Davis MD FACS, et al American College of Surgeons (2019). 2019.
19. Pearls & Oy-Sters: What Came First, the Bleed or the Fall?: An Aneurysmal Subdural Hemorrhage. — Parkin K, Taylor E, Rane N, Dawe G, Hall C. Neurology. 2024.
20. Cerebral Amyloid Angiopathy and Risk of Isolated Nontraumatic Subdural Hemorrhage. — Rivier CA, Kamel H, Sheth KN, et al. JAMA Neurology. 2024.
21. Management of Chronic Subdural Hematoma: A Systematic Review and Component Network Meta-Analysis of 455 Studies With 103 645 Cases. — Henry J, Amoo M, Kissner M, et al. Neurosurgery. 2022.
22. Pitfalls in the Diagnosis of Subdural Hemorrhage - Mimics and Uncommon Causes. — Bordia R, Le M, Behbahani S. Journal of Clinical Neuroscience : Official Journal of the Neurosurgical Society of Australasia. 2021.
23. Subdural Hematoma Mimickers: A Systematic Review. — Catana D, Koziarz A, Cenic A, et al. World Neurosurgery. 2016.
24. Imaging of Intracranial Haemorrhage. — Kidwell CS, Wintermark M. The Lancet. Neurology. 2008.
25. Risk Factors for Neurosurgical Intervention Within 48 Hours of Admission for Patients With Mild Traumatic Brain Injury and Isolated Subdural Hematoma. — Orlando A, Panchal RR, Mellor L, et al. Journal of Neurosurgery. 2025.
26. ACR Appropriateness Criteria® Head Trauma: 2021 Update. — Expert Panel on Neurological Imaging, Shih RY, Burns J, et al. Journal of the American College of Radiology : JACR. 2021.
27. Clinical Reasoning: An Older Woman With Headaches and Lethargy After a Fall. — Heide SK, Gnanaprakasam R, Bornovski Y, et al. Neurology. 2023.
28. Dexamethasone versus Surgery for Chronic Subdural Hematoma. — Miah IP, Holl DC, Blaauw J, et al. The New England Journal of Medicine. 2023.
29. Surgery Versus Conservative Treatment for Traumatic Acute Subdural Haematoma: A Prospective, Multicentre, Observational, Comparative Effectiveness Study. — van Essen TA, Lingsma HF, Pisică D, et al. The Lancet. Neurology. 2022.
30. Acute Surgery vs Conservative Treatment for Traumatic Acute Subdural Hematoma. — Van Essen TA, Yue JK, Barber J, et al. JAMA Network Open. 2025.
31. Association of Race and Ethnicity to Incident Epilepsy, or Epileptogenesis, After Subdural Hematoma. — Brown SC, King ZA, Kuohn L, et al. Neurology. 2020.
32. Brain Trauma Foundation Guidelines for the Management of Penetrating Traumatic Brain Injury, Second Edition. — Bell RS, Selph S, Ghajar J, et al. Neurosurgery. 2026.
33. Chronic Subdural Hematoma Management: A Systematic Review and Meta-Analysis of 34,829 Patients. — Almenawer SA, Farrokhyar F, Hong C, et al. Annals of Surgery. 2014.
34. Burr-Hole Drainage With or Without Irrigation for Chronic Subdural Haematoma (FINISH): A Finnish, Nationwide, Parallel-Group, Multicentre, Randomised, Controlled, Non-Inferiority Trial. — Raj R, Tommiska P, Koivisto T, et al. Lancet. 2024.
35. Current State of the Field and Recommendations for Middle Meningeal Artery Embolization in Chronic Subdural Hematoma: A Report of the SNIS Standards and Guidelines Committee, Endorsed by ANZSNR and ESMINT. — Mascitelli JR, Bulsara KR, Marden FA, et al. Journal of Neurointerventional Surgery. 2026.
36. Adjunctive Middle Meningeal Artery Embolization for Subdural Hematoma. — Davies JM, Knopman J, Mokin M, et al. The New England Journal of Medicine. 2024.
37. Management of Chronic Subdural Hematoma With Adjunctive Embolization of Middle Meningeal Artery. — Shankar JJS, Alcock S, Kashani N, et al. The Journal of the American Medical Association. 2026.
38. Meningeal Embolization for Preventing Chronic Subdural Hematoma Recurrence After Surgery. — Shotar E, Mathon B, Salle H, et al. The Journal of the American Medical Association. 2025.
39. Operative Neurosurgery for Traumatic Subdural Hematoma: Association Between Trauma Center Variation and Patient Outcomes. — Vattipally VN, Ran KR, Mukherjee D, et al. Journal of Neurosurgery. 2025.
40. Middle Meningeal Artery Embolization Versus Conventional Management for Patients With Chronic Subdural Hematoma: A Systematic Review and Meta-Analysis. — Sattari SA, Yang W, Shahbandi A, et al. Neurosurgery. 2023.