Sudden Infant Death Syndrome (SIDS)
SIDS is the sudden, unexplained death of an apparently healthy infant younger than 1 year of age that remains unexplained after a thorough investigation including autopsy, death scene investigation…
SIDS is the sudden, unexplained death of an apparently healthy infant younger than 1 year of age that remains unexplained after a thorough investigation including autopsy, death scene investigation, and review of clinical history.[1-2] Approximately 3,500 infants die annually in the US from sleep-related deaths, with SIDS accounting for ~41% of all sudden unexpected infant deaths (SUID).[1][3] The triple risk model — convergence of an intrinsically vulnerable infant, a critical developmental period, and an exogenous stressor — is the most widely accepted pathogenic framework.[4]
1. History
- SIDS is a diagnosis of exclusion made postmortem; there is no "presenting history" in the traditional sense. The clinical encounter typically involves either risk reduction counseling or ED presentation of an unresponsive/deceased infant.[1-2]
For risk assessment, key HPI elements include
- Sleep environment: position placed, surface type, bedding, co-sleeping, room temperature[2]
- Feeding method: breastfeeding vs. formula, pacifier use[2]
- Prenatal exposures: tobacco, alcohol, marijuana, opioids[1]
- Recent illness: URI symptoms, fever, immunization timing[5]
- Timing: most deaths occur during sleep, often overnight or during naps[1]
- For Brief Resolved Unexplained Events (BRUE) — formerly ALTE — presenting with apnea, color change, tone change, or altered responsiveness, a detailed event history is critical[6]
2. Alarm Features
- Recurrent BRUEs (multiple events increase risk of serious underlying diagnosis)[7]
- Infant found prone or face-down in unsafe sleep environment[2]
- Signs of non-accidental trauma: bruising, retinal hemorrhages, fractures[8]
- History of prior sibling death under same caregiver (raises concern for infanticide, estimated <5% of SUID)[5]
- Apnea or cyanosis requiring CPR by bystander[9]
- Features suggesting underlying cardiac (prolonged QT), metabolic, or neurologic disease[4][8]
3. Medications
- No medications prevent SIDS. Home cardiorespiratory monitors do not reduce SIDS risk and should not be used as a prevention strategy.[1-2]
Prenatal/postnatal substance exposure increases risk
- Nicotine (smoking/vaping) — strongest modifiable prenatal risk factor[1][3]
- Alcohol, marijuana, opioids, illicit drugs[1]
- Caffeine citrate is used for apnea of prematurity in preterm infants but is not a SIDS prevention strategy
- Immunizations are protective — routine vaccination per AAP/CDC schedule is recommended (Level A)[1][3]
4. Diet
- Breastfeeding is protective and is an AAP Level A recommendation:[1]
- Exclusive breastfeeding for 6 months is ideal; however, any amount of breast milk is protective[2]
- Protective effect increases with duration of breastfeeding[2]
- No specific dietary triggers for SIDS
- Adequate hydration and nutrition support normal infant development and arousal mechanisms
5. Review of Systems
- Respiratory: apnea episodes, noisy breathing, stridor, snoring
- Cardiac: cyanotic episodes, feeding intolerance (may suggest structural heart disease or channelopathy)
- Neurologic: seizure-like activity, abnormal tone, altered consciousness
- GI: significant reflux, choking/gagging episodes, vomiting
- Infectious: recent URI, fever, rhinorrhea (mild infection present in ~50% of SIDS cases)[5]
- General: excessive sweating during sleep (overheating), poor weight gain
6. Collateral History and Family History
- Family history of SIDS in a sibling (OR 4.31)[10]
- Family history of sudden cardiac death before age 50, unexplained drowning, unexplained seizures, or syncope — raises concern for inherited channelopathies (long QT syndrome, Brugada, CPVT)[11-12]
- Family history of inborn errors of metabolism (e.g., MCAD deficiency)[4-5]
- Social context: caregiver substance use, mental health, socioeconomic status, housing stability, access to prenatal care[2][13]
- Collateral from anyone present at the time of the event or who last saw the infant alive
7. Risk Factors
Nonmodifiable
- Export Risk Factor Odds Ratio References Preterm birth (37 weeks) 11.7 (1.8–74.1)[1]
- Birth weight 2,500 g 3.3[1]
- Poverty 2.3 (1.1–5.1)[1]
- Male sex 1.7[1]
- No prenatal care 1.7[1]
- African American, Native American, Alaska Native race/ethnicity 2–3× national average[2]
Modifiable
- Prone/side sleep position (strongest modifiable risk factor — Back to Sleep campaign reduced SIDS by 39%)
- Bed sharing/surface sharing (≥2× increased risk; higher if <12 weeks, with smoker, or with intoxicated caregiver)
- Soft bedding, loose blankets, pillows, crib bumpers
- Tobacco/nicotine exposure (prenatal and postnatal; dose-dependent)
- Alcohol, marijuana, opioid use during pregnancy and after birth
- Overheating/overbundling, head covering
- Inclined sleep surfaces, car seats/strollers used as purposeful sleep surfaces
- Young maternal age (<25 years), short interpregnancy interval, multiple gestation[10][15]
8. Differential Diagnosis
- SIDS is a diagnosis of exclusion within the broader category of SUID. Causes that must be ruled out:[1][5][8]
- Accidental suffocation/asphyxia — soft bedding overlay, wedging, entrapment
- Non-accidental trauma (child abuse) — intentional suffocation, shaken baby syndrome
- Cardiac channelopathies — long QT syndrome (~5–10% of SUID), Brugada syndrome, CPVT[4][11]
- Inborn errors of metabolism — MCAD deficiency (~1% of SUID), fatty acid oxidation disorders[5]
- Infection — sepsis, meningitis, myocarditis (mild antecedent infection in ~50% of SIDS cases)[5]
- Congenital cardiac anomalies — structural heart disease
- Epilepsy/seizure disorders — undiagnosed epilepsy
- Toxic ingestion — accidental or intentional poisoning
- Cardiomyopathy — hypertrophic cardiomyopathy[16]
9. Past Medical History
- Prematurity (4× increased SIDS risk)[3][17]
- Low birth weight or intrauterine growth restriction[2]
- NICU admission[18]
- Prior BRUE/ALTE episodes[6]
- Known cardiac, metabolic, or neurologic conditions
- Newborn screening results — review for undiagnosed metabolic disorders[4][19]
- Prenatal history: adequacy of prenatal care, maternal smoking, substance use, complications[1]
10. Physical Exam
- In the context of a BRUE evaluation or well-child risk assessment:
- Vital signs: temperature (overheating), heart rate, respiratory rate, oxygen saturation
- General: overall appearance, tone, activity level, dysmorphic features
- HEENT: nasal patency, oropharyngeal obstruction, signs of trauma
- Cardiovascular: murmurs, rhythm irregularities, perfusion
- Respiratory: work of breathing, stridor, wheezing
- Neurologic: tone (hyper/hypotonia), reflexes, fontanelle fullness, eye movements
- Skin: bruising (especially in pre-mobile infants — red flag for abuse), petechiae, rashes
- Musculoskeletal: tenderness, swelling suggesting occult fractures
- In the setting of a deceased infant: full external examination noting lividity pattern, rigor, signs of trauma; formal autopsy is required[12][20]
11. Lab Studies
For BRUE workup (targeted, not routine)
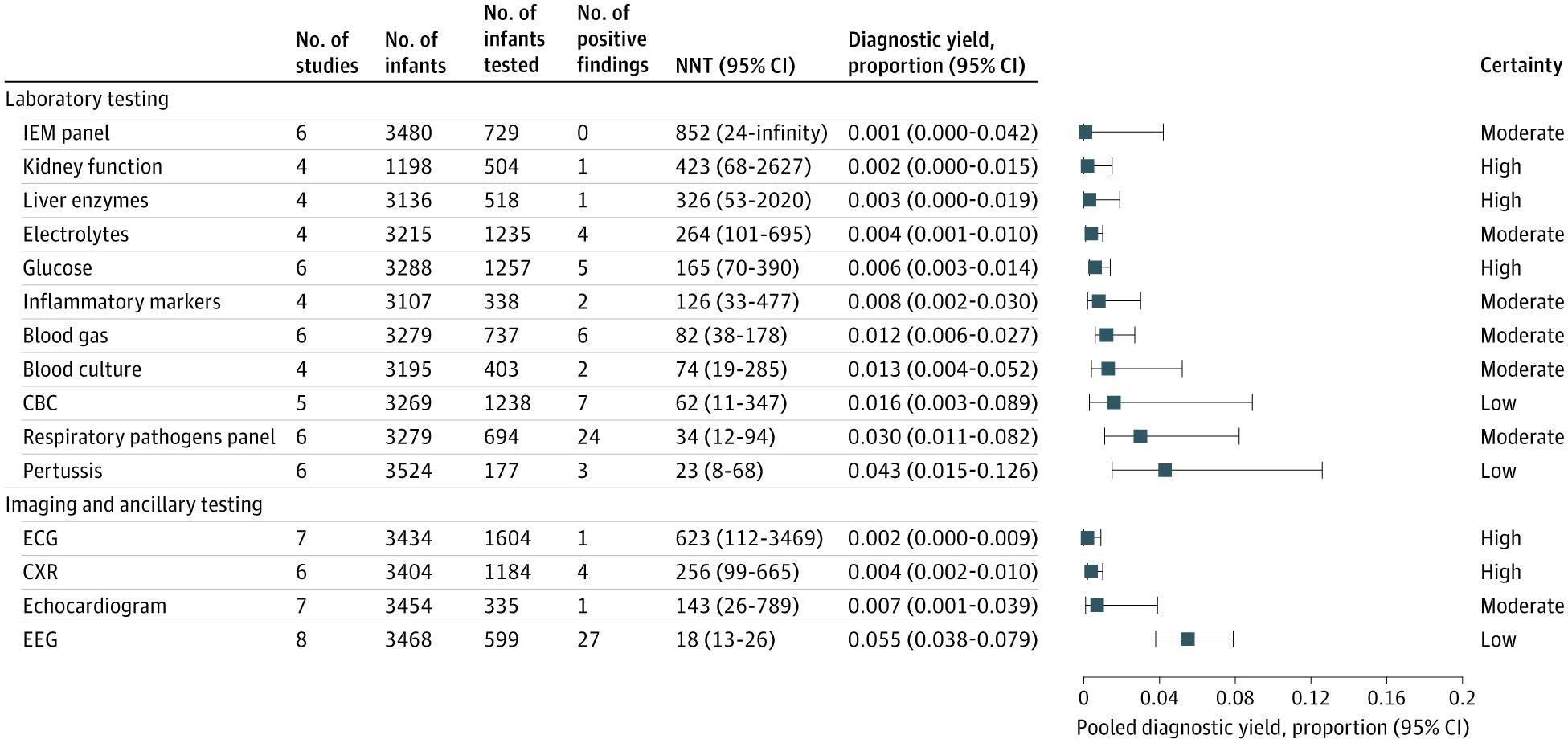
- Routine labs (metabolic panels, electrolytes) have exceedingly low yield (<0.5%) and are not recommended as screening[7]
If clinical suspicion warrants
- CBC, blood culture, urinalysis (infection)
- Blood glucose, lactate, ammonia, serum amino acids, urine organic acids (metabolic disease)
- Acylcarnitine profile (fatty acid oxidation disorders)
- Toxicology screen
- Postmortem: genetic testing for cardiac channelopathies and metabolic disorders is recommended when autopsy is inconclusive[12]
12. Imaging
- Not routinely indicated for SIDS risk assessment
- For BRUE evaluation: chest radiograph yield is only 0.4% (NNT = 256)[7]
- If non-accidental trauma suspected: skeletal survey, head CT/MRI[8]
- Echocardiography if structural heart disease suspected[8]
- Postmortem imaging (CT/MRI) may complement autopsy in SUID investigation[8]
13. Special Tests
- ECG: low yield as routine screening in BRUE (0.2%, NNT = 623), but indicated if family history of sudden cardiac death, long QT, or syncope[7][11]
- EEG: higher yield than other tests when seizure is suspected[7]
- Polysomnography: not routinely recommended; may be considered in select cases with recurrent apnea
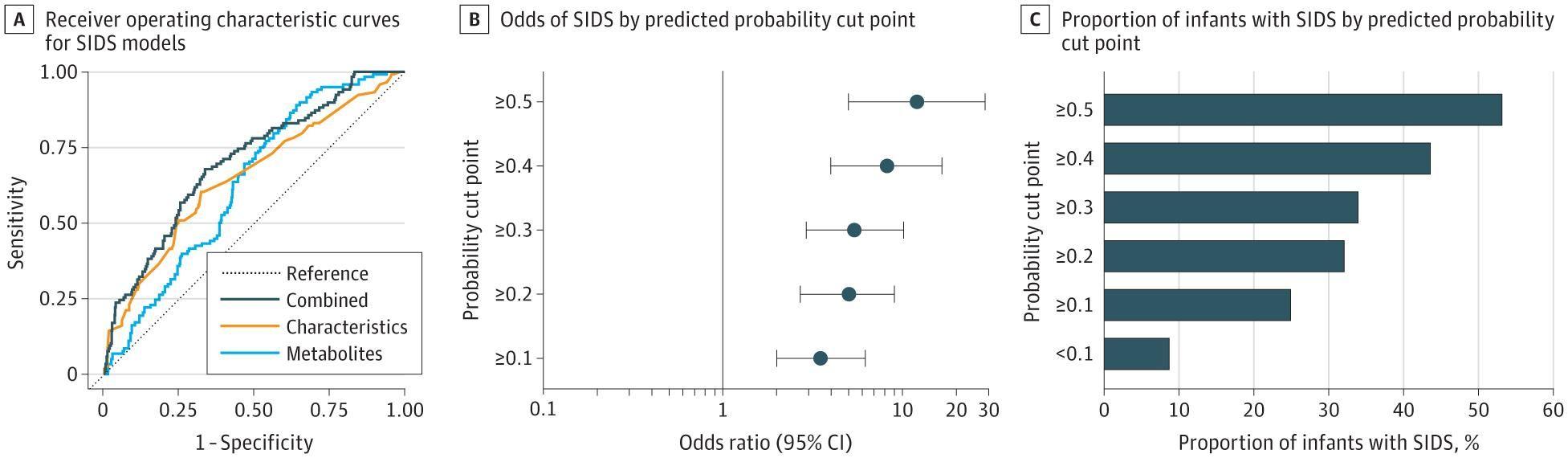
- Newborn metabolic screening: review results; emerging evidence suggests metabolic patterning from NBS may enhance SIDS risk prediction[19]
- Postmortem genetic testing (molecular autopsy): recommended when conventional autopsy is non-diagnostic, especially for cardiac channelopathy genes (SCN5A, KCNQ1, KCNH2, RYR2)[4][12][16]
14. ECG
- Routine neonatal ECG screening for SIDS prevention is not currently recommended by the AAP
- Long QT syndrome accounts for an estimated 5–10% of SUID cases[4][11]
- QTc prolongation >470 ms in neonates is concerning
- Abnormal T-wave morphology may suggest specific genotypes
- Brugada pattern: coved ST elevation in V1–V2[11]
- Wolff-Parkinson-White: delta waves, short PR
- ECG should be obtained in any infant with a BRUE if there is clinical suspicion for arrhythmia, family history of sudden death, or syncope[11]
- First-degree relatives of SIDS victims should be referred for cardiac evaluation including ECG[12]
15. Assessment
- SIDS is the leading cause of postneonatal infant mortality (ages 1–12 months) in the US[3]
- Peak incidence: 1–4 months of age; 90% occur before 6 months; uncommon after 8 months[4][14]
- Incidence: ~0.4–0.5 per 1,000 live births[3][21]
- More common in males (60:40 ratio), winter months, and among socioeconomically disadvantaged populations[14-15]
- The triple risk model remains the dominant conceptual framework: intrinsic vulnerability + critical developmental period + exogenous stressor[4]
- Despite the 1992 Back to Sleep campaign reducing SIDS by ~50%, rates have plateaued since ~2000, and overall SUID rates remain stable due to diagnostic reclassification[2-3]
- Racial/ethnic disparities persist: African American, Native American, and Alaska Native infants have 2–3× the national average SIDS rate[14]
16. Treatment Plan
- SIDS is inherently a prevention-focused condition. There is no treatment once death has occurred.
Primary Prevention (AAP Level A Recommendations)
- Supine sleep position for every sleep
- Firm, flat, noninclined sleep surface (crib, bassinet, or play yard meeting CPSC standards)
- Room sharing without bed sharing for at least the first 6 months (ideally 12 months)
- No soft bedding: remove pillows, blankets, bumpers, stuffed animals
- Breastfeeding: exclusive for 6 months; any amount is protective
- Pacifier use at sleep onset (even if expelled during sleep)[4]
- Avoid tobacco/nicotine exposure — prenatal and postnatal
- Avoid alcohol, marijuana, opioids, illicit drugs during pregnancy and postpartum
- Avoid overheating: dress infant in no more than 1 layer beyond what an adult would wear; no hats indoors[1]
- Regular prenatal care
- Routine immunizations per AAP/CDC schedule
- Supervised awake tummy time to promote development
What does NOT reduce SIDS risk
- Home cardiorespiratory monitors
- Commercial devices marketed for SIDS prevention
- Swaddling (no evidence of SIDS reduction; discontinue when infant attempts to roll)
After a SIDS death
- Complete unrestricted autopsy (preferably by pathologist with cardiovascular expertise)
- Death scene investigation with doll reenactment
- Postmortem genetic testing if autopsy is non-diagnostic
- Referral of first-degree family members for cardiac evaluation and genetic counseling
- Compassionate, non-accusatory family support and grief counseling
17. Disposition
- BRUE — Lower risk: may be managed with brief observation (1–4 hours) and discharged with close follow-up; routine admission is not recommended[6]
- BRUE — Higher risk (age ≤60 days, preterm, multiple events, CPR required): admission for monitoring and targeted workup[22]
- Infant found deceased: pronouncement of death, notification of medical examiner/coroner, initiation of death scene investigation[20]
Specialist consultation triggers
- Cardiology: family history of sudden death, abnormal ECG, recurrent cyanosis[11-12]
- Genetics/Metabolism: abnormal newborn screen, suspected inborn error of metabolism[4]
- Child abuse team: any suspicion of non-accidental trauma[8]
- Pulmonology: recurrent apnea, airway abnormalities
18. Follow Up / Return Precautions
For families with a living infant at risk
- Reinforce safe sleep practices at every well-child visit through age 12 months
- Counsel on return precautions: apnea, cyanosis, limpness, unresponsiveness → call 911 immediately
- Smoking cessation support for all household members
- Breastfeeding support and lactation consultation
After a SIDS event
- Schedule follow-up within 1–2 weeks for surviving family members
- Monitor for complicated grief, depression, PTSD, and relationship strain
- Refer to mental health professionals and peer support groups (First Candle, Share Pregnancy and Infant Loss Support, The Compassionate Friends)[2]
- Evaluate surviving siblings and future pregnancies for potential inherited conditions (cardiac channelopathies, metabolic disorders)[12]
- Offer to review autopsy and investigation findings with the family when available[20]
- Counsel that subsequent siblings are at slightly increased risk; reinforce safe sleep practices for all future infants
- Relevant images 2 items
- Model-Derived Area Under the Receiver Operating Characteristic Curve and Predicted Probability Statistics
- JAMA Pediatr October 31, 2024
- Summary of Diagnostic Test Yields in Infants With a Brief Resolved Unexplained Event
- JAMA Pediatr January 25, 2026
References
1. Sleep-Related Infant Deaths: Updated 2022 Recommendations for Reducing Infant Deaths in the Sleep Environment. — Moon RY, Carlin RF, Hand I. Pediatrics. 2022.
2. Sudden Infant Death Syndrome: Common Questions and Answers. — Darrow HJ, Carman KA, Wheeler V. American Family Physician. 2025.
3. Risk Factors, Protective Factors, and Current Recommendations to Reduce Sudden Infant Death Syndrome: A Review. — Carlin RF, Moon RY. JAMA Pediatrics. 2017.
4. Evidence Base for 2022 Updated Recommendations for a Safe Infant Sleeping Environment to Reduce the Risk of Sleep-Related Infant Deaths. — Moon RY, Carlin RF, Hand I. Pediatrics. 2022.
5. The Sudden Infant Death Syndrome. — Kinney HC, Thach BT. The New England Journal of Medicine. 2009.
6. Brief Resolved Unexplained Events (Formerly Apparent Life-Threatening Events) and Evaluation of Lower-Risk Infants. — Tieder JS, Bonkowsky JL, Etzel RA, et al. Pediatrics. 2016.
7. Infant Outcomes, Risk Factors, and Diagnostic Yield After a Brief Resolved Unexplained Event. — Nama N, Liebert S, Abaji M, et al. JAMA Pediatrics. 2026.
8. Child Neurology: A Case Illustrating the Role of Imaging in Evaluation of Sudden Infant Death. — Kranick SM, Ganesh J, Coughlin CR, Licht DJ. Neurology. 2009.
9. Brief Resolved Unexplained Events: A New Diagnosis, With Implications for Evaluation and Management. — Ramgopal S, Colgan JY, Roland D, Pitetti RD, Katsogridakis Y. European Journal of Pediatrics. 2022.
10. Development of a Risk Score to Predict Sudden Infant Death Syndrome. — Polavarapu M, Klonoff-Cohen H, Joshi D, et al. International Journal of Environmental Research and Public Health. 2022.
11. Sudden Death in the Young: Information for the Primary Care Provider. — Erickson CC, Salerno JC, Berger S, et al. Pediatrics. 2021.
12. Part 8: Pediatric Advanced Life Support: 2025 American Heart Association and American Academy of Pediatrics Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Lasa JJ, Dhillon GS, Duff JP, et al. Pediatrics. 2026.
13. Changes in Background Characteristics and Risk Factors Among SIDS Infants in England: Cohort Comparisons From 1993 to 2020. — Pease A, Turner N, Ingram J, et al. BMJ Open. 2023.
14. Sudden Infant Death Syndrome. — Moon RY, Horne RS, Hauck FR. Lancet. 2007.
15. Infant Pacifiers for Reduction in Risk of Sudden Infant Death Syndrome. — Psaila K, Foster JP, Pulbrook N, Jeffery HE. The Cochrane Database of Systematic Reviews. 2017.
16. Post-Mortem Whole-Exome Analysis in a Large Sudden Infant Death Syndrome Cohort With a Focus on Cardiovascular and Metabolic Genetic Diseases. — Neubauer J, Lecca MR, Russo G, et al. European Journal of Human Genetics : EJHG. 2017.
17. Physiology During Sleep in Preterm Infants: Implications for Increased Risk for the Sudden Infant Death Syndrome. — Horne RS, Harrewijn I, Hunt CE. Sleep Medicine Reviews. 2024.
18. Newborn auditory brainstem response and sudden infant death syndrome. — Maylott SE, Zeng G, Leung TS, et al. Journal of Neuroscience Research. 2024.
19. Early Newborn Metabolic Patterning and Sudden Infant Death Syndrome. — Oltman SP, Rogers EE, Baer RJ, et al. JAMA Pediatrics. 2024.
20. Half Century Since SIDS: A Reappraisal of Terminology. — Shapiro-Mendoza CK, Palusci VJ, Hoffman B, et al. Pediatrics. 2021.
21. Cardiac Genetic Predisposition in Sudden Infant Death Syndrome. — Tester DJ, Wong LCH, Chanana P, et al. Journal of the American College of Cardiology. 2018.
22. A Framework for Evaluation of the Higher-Risk Infant After a Brief Resolved Unexplained Event. — Merritt JL, Quinonez RA, Bonkowsky JL, et al. Pediatrics. 2019.