Syncope (Cardiac)
Cardiac syncope accounts for 5% to 21% of ED syncope presentations and carries the highest morbidity and mortality among syncope etiologies, with 1-year mortality 2 to 5 times that of noncardiac sy…
Cardiac syncope accounts for 5% to 21% of ED syncope presentations and carries the highest morbidity and mortality among syncope etiologies, with 1-year mortality 2 to 5 times that of noncardiac syncope.[1-2] It results from a marked reduction in cardiac output due to arrhythmia, structural heart disease, or cardiopulmonary pathology leading to cerebral hypoperfusion.[3] The following is a comprehensive clinical summary organized for emergency medicine and primary care workflows.
1. History
- Onset and prodrome: Sudden loss of consciousness without prodrome or with only brief palpitations strongly suggests cardiac etiology; prolonged prodrome (nausea, warmth, diaphoresis) favors vasovagal[1][4]
- Activity at time of event: Syncope during exertion (not post-exertion) or while supine is highly concerning for cardiac cause[4]
- Associated symptoms: Chest pain, dyspnea, or palpitations immediately preceding the event[1]
- Duration and recovery: Typically brief LOC with rapid return to baseline; prolonged confusion suggests seizure
- Number of episodes: Low number of episodes (1–2) is more associated with cardiac syncope; >4 years of recurrent episodes suggests lower cardiac risk[1][4]
- Witnessed features: Ask bystanders about cyanosis during the event (LR 6.2 for cardiac syncope), seizure-like activity, and duration of unconsciousness[3]
- Important negatives: Absence of positional triggers, emotional triggers, prolonged standing, or post-event nausea argues against vasovagal[3]
2. Alarm Features
- Syncope during exertion[1][4]
- Syncope while supine or at rest[4]
- Sudden onset without prodrome[4-5]
- Chest pain or dyspnea preceding the event[1]
- Palpitations immediately before LOC[5]
- Witnessed cyanosis during the episode[3]
- Family history of sudden cardiac death <50 years of age or inheritable cardiac conditions (LQTS, Brugada, HCM)[4][6]
- Known structural heart disease, reduced LVEF, or prior arrhythmias[4-5]
- Abnormal ECG (see ECG section below)[1]
- SBP <90 mmHg on presentation[1][7]
3. Medications
- Medications that can cause or contribute to cardiac syncope:
- QT-prolonging drugs (>200 drugs): antiarrhythmics (sotalol, dofetilide, quinidine, procainamide, ibutilide), antipsychotics (haloperidol, thioridazine), antibiotics (erythromycin, fluoroquinolones, azithromycin), antidepressants (citalopram, TCAs), methadone, ondansetron[5][8]
- Bradycardia-inducing agents: beta-blockers, non-DHP calcium channel blockers, digoxin, amiodarone, clonidine
- Hypotension-inducing agents: antihypertensives, diuretics, alpha-blockers, nitrates, vasodilators, dopaminergics[1]
- Proarrhythmic antiarrhythmics: Class IC agents (flecainide, propafenone) in patients with structural heart disease
Key medication cautions
- Maintain K⁺ >4.0 mEq/L and Mg²⁺ >2.0 mg/dL in patients on QT-prolonging drugs[8]
- Avoid combining multiple QT-prolonging agents
- Check www.crediblemeds.org for updated QT-prolonging drug lists[5]
4. Diet
- Hydration: Dehydration and volume depletion can exacerbate arrhythmia-related hemodynamic compromise
- Electrolytes: Hypokalemia, hypomagnesemia, and hypocalcemia increase arrhythmia risk and can precipitate torsades de pointes[8]
- Alcohol and stimulants: Excessive alcohol, caffeine, and energy drinks can trigger arrhythmias
- Long-term: Patients with heart failure–related cardiac syncope should follow sodium and fluid restriction per GDMT guidelines
5. Review of Systems
- Cardiovascular: Palpitations, chest pain, dyspnea on exertion, orthopnea, PND, lower extremity edema
- Neurologic: Headache, focal weakness, speech changes, seizure activity (to distinguish from neurologic mimics)
- GI: Hematemesis, melena, hematochezia (GI bleed as alternative cause)
- Pulmonary: Pleuritic chest pain, calf swelling (PE as alternative cause)
- Psychiatric: Anxiety, panic symptoms, hyperventilation (psychogenic pseudosyncope)
6. Collateral History and Family History
- Bystander account is critical: witnessed cyanosis, duration of LOC, seizure-like movements, recovery time[1][3]
- Family history of sudden cardiac death <50 years, unexplained drowning, or unexplained seizures[4]
- Inheritable conditions: Brugada syndrome, HCM, LQTS, CPVT, ARVC[4][6]
- Social context: Occupation (driving, operating machinery), fall risk, living situation
7. Risk Factors
- Age >60 years (strongest demographic predictor)[4]
- Male sex[4]
- Known structural heart disease: ischemic cardiomyopathy, reduced LVEF, valvular disease[4-5]
- Prior arrhythmias or history of atrial fibrillation (LR 7.3 for cardiac syncope)[3]
- Congenital heart disease[4]
- Family history of SCD or channelopathies[4][6]
- Abnormal baseline ECG[1]
- Age at first syncope ≥35 years (LR 3.3 for cardiac syncope; age <35 has LR 0.13)[3]
8. Differential Diagnosis
Cardiac arrhythmic causes
- Ventricular tachycardia (sustained VT) — most dangerous, especially with structural heart disease
- Bradyarrhythmias: sick sinus syndrome, high-grade AV block (Mobitz II, complete heart block), sinus pauses >3 seconds[9]
- Supraventricular tachycardia with rapid ventricular response
- Channelopathies: Long QT syndrome, Brugada syndrome, CPVT, WPW syndrome[4-5]
- Pacemaker/ICD malfunction[9]
Cardiac structural causes
- Severe aortic stenosis — classic exertional syncope in elderly
- Hypertrophic cardiomyopathy — exertional syncope in young patients, family history of SCD[1]
- Acute myocardial infarction/ischemia[1]
- Cardiac tamponade, aortic dissection[1]
- Pulmonary embolism[1]
- Atrial myxoma or intracardiac tumor[9]
- ARVC[4]
Cannot-miss diagnoses
- Aortic dissection (hypotension, tearing chest/back pain)
- Massive PE (dyspnea, tachycardia, hypoxia)
- Acute MI (chest pain, diaphoresis, ECG changes)
- Cardiac tamponade (Beck's triad)
Key mimics to distinguish
- Vasovagal syncope (prodrome, triggers, post-event nausea)[3]
- Orthostatic hypotension (positional, medication-related)[1]
- Seizure (prolonged postictal state, tongue biting, incontinence)
- Psychogenic pseudosyncope (prolonged duration, eyes closed, normal vitals)[1]
9. Past Medical History
- Prior syncope episodes and their evaluation
- Known coronary artery disease, heart failure, cardiomyopathy
- Prior arrhythmias (AF, VT, SVT)
- Cardiac devices (pacemaker, ICD) — interrogation is essential
- Valvular heart disease (especially aortic stenosis)
- Prior cardiac surgery or catheterization
- Congenital heart disease
- Chronic conditions: diabetes (autonomic neuropathy), CKD (electrolyte derangements)
10. Physical Exam
Vital signs
- Heart rate and rhythm: Bradycardia (<50 bpm), tachycardia, irregular rhythm[1]
- Blood pressure: SBP <90 mmHg or >180 mmHg indicates higher risk[1]
- Orthostatic vitals: Supine → standing at 1 and 3 minutes (drop ≥20 mmHg systolic or ≥10 mmHg diastolic = orthostatic hypotension)[1]
- Oxygen saturation
Focused cardiac exam
- Murmurs: Systolic crescendo-decrescendo (aortic stenosis), systolic murmur increasing with Valsalva (HCM)[1]
- Gallops (S3, S4): Suggest heart failure or cardiomyopathy
- JVD, peripheral edema: Right heart failure, tamponade, PE
- Pulsus paradoxus: Tamponade
- Unequal pulses/BP: Aortic dissection
Neurologic exam
- Focal deficits suggest stroke/TIA rather than syncope[1]
- Mental status — should be fully normal after true syncope
11. Lab Studies
- Troponin: Elevated levels associated with higher risk of adverse outcomes; should be obtained when cardiac syncope is suspected[1]
- BNP/NT-proBNP: Elevated levels suggest structural heart disease or heart failure; BNP ≥300 pg/mL is a component of the ROSE rule[1][7]
- Basic metabolic panel: Electrolytes (K⁺, Mg²⁺, Ca²⁺), renal function, glucose
- CBC: Hemoglobin/hematocrit (Hct <30% is a San Francisco Syncope Rule criterion; rule out GI bleed)[7]
- D-dimer: If PE is suspected
- hCG: Women of childbearing age
- Lactate: If concern for shock or hypoperfusion
- Labs to rule out dangerous conditions: troponin (ACS), BNP (HF), hemoglobin (hemorrhage), D-dimer (PE)[1]
12. Imaging
First-line
- Transthoracic echocardiography (TTE): Recommended when history, exam, or ECG suggest structural heart disease — identifies aortic stenosis, HCM, pericardial effusion/tamponade, RV strain (PE), reduced LVEF[1][10]
When indicated
- CT pulmonary angiography: Only if PE is clinically suspected[1]
- Cardiac MRI: If ARVC or cardiac sarcoidosis is suspected[10]
- CT/MRI head: Only if head trauma or neurologic findings; <0.1% diagnostic yield for syncope without these features[1]
When imaging is unnecessary
- Routine head CT in the absence of trauma or focal neurologic deficits[1]
- Carotid ultrasound without focal neurologic findings[1]
13. Special Tests
Risk stratification scores
- Canadian Syncope Risk Score (CSRS): Most validated tool; components include ECG findings, clinical diagnosis, vasovagal predisposition, heart disease history, SBP, and troponin. Very low/low risk (CSRS <0): <1% 30-day serious outcome rate; no deaths or ventricular arrhythmias in validation[1][11]
- FAINT score: Designed for patients ≥40 years; low-risk score (FAINT = 0) had 96.7% sensitivity and 98.8% NPV for serious cardiac outcomes in a recent US validation[12]
- San Francisco Syncope Rule: 5 criteria (abnormal ECG, Hct <30%, CHF history, SOB, SBP <90); sensitivity 87% but limited specificity[7][13]
Other tests
- Electrophysiology study (EPS): For patients with structural heart disease and unexplained syncope; can induce VT/VF to guide ICD placement[14-15]
- Tilt table testing: Primarily for suspected reflex syncope when diagnosis is uncertain[1]
- Carotid sinus massage: For patients >40 years with syncope suggestive of carotid sinus hypersensitivity[1]
- Exercise stress testing: When syncope occurs during or after exertion[1]
14. ECG
- A resting 12-lead ECG is a Class I recommendation in all patients with syncope (ACC/AHA/HRS 2017).[4]
High-risk ECG findings suggesting cardiac syncope
- Export ECG Finding Clinical Significance Ref Mobitz type II or 3rd-degree AV block High risk; may need pacing[1-2]
- Sinus bradycardia 40 bpm or pauses >3 sec Sick sinus syndrome[1-2]
- Alternating LBBB/RBBB Severe conduction disease[2]
- VT or SVT Arrhythmic syncope[1-2]
- Short PR + delta wave Wolff-Parkinson-White syndrome[1, 3]
- Coved ST elevation V1-V2 + inverted T waves Brugada syndrome (Type 1)[1, 3][4]
- Prolonged QTc (>470 ms ♂, >480 ms ♀) Long QT syndrome (congenital or acquired)[1, 5]
- LVH voltage criteria Suggests HCM or hypertensive heart disease[3, 6]
- Epsilon waves + T-wave inversions V1-V3 ARVC[3]
- Q waves, ST changes (ischemic pattern) Prior MI or acute ischemia[1]
- Bifascicular block Risk of intermittent complete heart block[1]
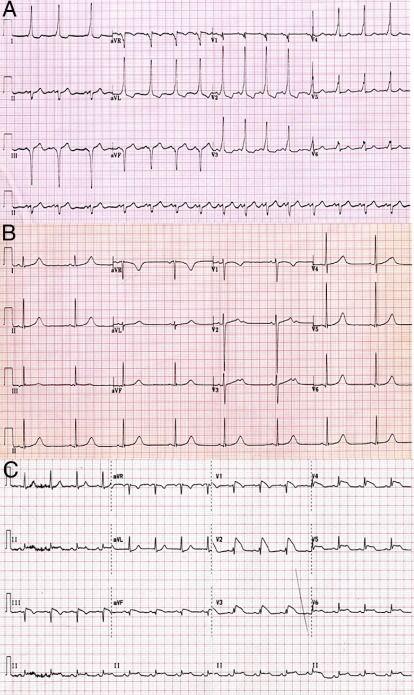
- The following figure illustrates characteristic ECG patterns of WPW, LQTS, and Brugada syndrome — three critical channelopathies to recognize in syncope evaluation:
- View full figure Figure 3. Electrocardiographic Patterns Observed in Electrical Cardiac Abnormalities Associated With Sudden Cardiac Death Sudden Cardiac Death in Young Athletes: Practical Challenges and Diagnostic Dilemmas. J Am Coll Cardiol. March 11, 2013.
15. Assessment
Clinical summary
- Cardiac syncope is a high-risk diagnosis with significant short- and long-term mortality[2]
- The immediate cause is cerebral hypoperfusion from reduced cardiac output (arrhythmic or structural)[3]
- Approximately 10% of ED syncope patients have a serious underlying cardiac condition[7][12]
- The 2017 ACC/AHA/HRS guidelines emphasize that history, physical exam, and ECG can establish the diagnosis or identify high-risk features in the majority of patients[4]
Severity stratification
- High risk: Abnormal ECG, known structural heart disease, syncope during exertion or supine, no prodrome, family history of SCD, SBP <90, elevated troponin/BNP[1][4][7]
- Intermediate risk: Age ≥50, prior cardiac history, concerning but nondiagnostic ECG, symptoms inconsistent with reflex syncope[4]
- Low risk: Young age, clear vasovagal or orthostatic trigger, normal ECG, no cardiac history[1][11]
- Complications to consider: Sudden cardiac death, traumatic injury from falls, recurrent syncope with driving/occupational hazards, heart failure progression
16. Treatment Plan
Initial stabilization (ED)
- ABCs, continuous cardiac monitoring, IV access
- Treat hemodynamically unstable arrhythmias per ACLS protocols
- Correct reversible causes: electrolyte repletion (K⁺ >4.0, Mg²⁺ >2.0), discontinue offending medications[8]
- Transcutaneous or transvenous pacing for symptomatic bradycardia/high-grade AV block
- Definitive treatment is directed at the underlying etiology:[1]
- Bradyarrhythmias (sinus node dysfunction, AV block): Permanent pacemaker implantation[4]
- Ventricular tachycardia with structural heart disease: ICD implantation; antiarrhythmic therapy (amiodarone); catheter ablation[4][14-15]
- Unexplained syncope + reduced LVEF + inducible VT on EPS: ICD recommended (Class I)[4][14]
- Unexplained syncope + nonischemic DCM + significant LV dysfunction: ICD is reasonable[4]
- SVT (WPW, AVNRT): Catheter ablation is often curative
- Channelopathies: Beta-blockers for LQTS and CPVT; ICD for high-risk patients with Brugada, LQTS refractory to beta-blockers, or CPVT with syncope on therapy[19]
- Structural causes: Aortic valve replacement for critical AS; septal myectomy or alcohol ablation for obstructive HCM; treatment of PE, tamponade, or dissection per standard protocols
- Guideline-directed medical therapy (GDMT) for underlying cardiomyopathy (ACEi/ARB/ARNI, beta-blocker, MRA, SGLT2i)[4]
17. Disposition
Admission criteria (ACC/AHA/HRS Class I)
- Serious medical condition identified during initial evaluation potentially relevant to syncope
- Documented arrhythmia as cause of syncope requiring treatment
- Syncope with hemodynamic instability
- Syncope causing significant injury
- High-risk features: abnormal ECG, known structural heart disease, syncope during exertion, family history of SCD, elevated troponin
Observation (structured ED protocol)
- Reasonable for intermediate-risk patients (Class IIa); structured ED observation with expedited cardiac testing reduces admissions without adverse outcomes[4]
- Telemetry monitoring >12 hours has higher sensitivity for arrhythmia detection than shorter intervals[1]
Discharge criteria
- Clear low-risk etiology identified (vasovagal, orthostatic with identifiable cause)
- Normal ECG, no structural heart disease, normal troponin
- CSRS very low/low risk (<0): <1% 30-day serious outcome; no deaths or VT in validation cohorts[1][11]
Specialist consultation triggers
- Cardiology/electrophysiology for suspected arrhythmic syncope, abnormal ECG, structural heart disease, or need for device evaluation
- Cardiac surgery for critical valvular disease
- Genetics for suspected channelopathy with family screening
18. Follow Up / Return Precautions
Follow-up timing
- High-risk discharged patients: Cardiology follow-up within 1–2 weeks with ambulatory cardiac monitoring (15-day monitoring shows greater sensitivity than shorter intervals)[1][20]
- Medium-risk patients: Follow-up within 1–2 weeks with 15-day cardiac monitoring if discharged[20]
- Low-risk patients: PCP follow-up as needed[20]
- If cause remains unknown after initial workup and cardiac cause is still suspected, consider implantable loop recorder for long-term monitoring[1]
- Return precautions — instruct patients to return immediately for:
- Recurrent syncope or presyncope
- Palpitations, chest pain, or dyspnea
- Sustained dizziness or lightheadedness
- New neurologic symptoms (weakness, speech difficulty, vision changes)
Patient counseling points
- Driving restrictions: Patients with cardiac syncope should be counseled to avoid driving until the underlying cause is identified and treated; specific restrictions vary by jurisdiction and etiology
- Avoid known triggers and offending medications
- Ensure medication compliance for cardiac conditions
- Family members should know CPR if high-risk arrhythmia is suspected
- Expected course: Prognosis depends entirely on the underlying etiology. Patients with identified and treated arrhythmias (e.g., pacemaker for AV block, ICD for VT) generally have good outcomes. Untreated cardiac syncope carries significant risk of recurrence and sudden death.[1-2]
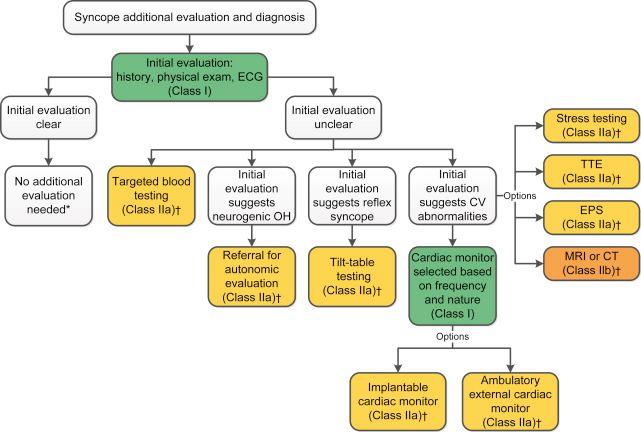
- The following figure from the 2017 ACC/AHA/HRS guidelines illustrates the algorithm for additional evaluation and diagnosis after initial syncope assessment:
References
1. Syncope: Evaluation and Differential Diagnosis. — Bayard M, Gerayli F, Holt J. American Family Physician. 2023.
2. Near-Syncope After Exercise. — Ziegelstein RC. The Journal of the American Medical Association. 2004.
3. Did This Patient Have Cardiac Syncope?The Rational Clinical Examination Systematic Review. — Albassam OT, Redelmeier RJ, Shadowitz S, et al. The Journal of the American Medical Association. 2019.
4. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients With Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Shen WK, Sheldon RS, Benditt DG, et al. Journal of the American College of Cardiology. 2017.
5. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
6. Sudden Death in the Young: Information for the Primary Care Provider. — Erickson CC, Salerno JC, Berger S, et al. Pediatrics. 2021.
7. Canadian Syncope Risk Score: A Validated Risk Stratification Tool. — Meisenheimer ES, Rogers TS, Saguil A. American Family Physician. 2021.
8. Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association. — Tisdale JE, Chung MK, Campbell KB, et al. Circulation. 2020.
9. New Concepts in the Assessment of Syncope. — Brignole M, Hamdan MH. Journal of the American College of Cardiology. 2012.
10. AHA/ACCF Scientific Statement on the Evaluation of Syncope: From the American Heart Association Councils on Clinical Cardiology, Cardiovascular Nursing, Cardiovascular Disease in the Young, and Stroke, and the Quality of Care and Outcomes Research Interdisciplinary Working Group; And the American College of Cardiology Foundation in Collaboration With the Heart Rhythm Society. — Strickberger SA, Benson DW, Biaggioni I, et al. Journal of the American College of Cardiology. 2006.
11. Multicenter Emergency Department Validation of the Canadian Syncope Risk Score. — Thiruganasambandamoorthy V, Sivilotti MLA, Le Sage N, et al. JAMA Internal Medicine. 2020.
12. Validation of 2 Syncope Risk Scores and Comparison With Physician Risk Estimation. — Suh EH, Winskill C, Sacco DL, et al. JAMA Network Open. 2026.
13. Risk-Stratification Tools for Emergency Department Patients With Syncope: A Systematic Review and Meta-Analysis of Direct Evidence for SAEM GRACE. — Wakai A, Sinert R, Zehtabchi S, et al. Academic Emergency Medicine : Official Journal of the Society for Academic Emergency Medicine. 2025.
14. 2012 ACCF/AHA/HRS Focused Update Incorporated Into the ACCF/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. — Epstein AE, DiMarco JP, Ellenbogen KA, et al. Journal of the American College of Cardiology. 2013.
15. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons. — Epstein AE, DiMarco JP, Ellenbogen KA, et al. Journal of the American College of Cardiology. 2008.
16. ECG Features That Suggest a Potentially Life-Threatening Arrhythmia as the Cause for Syncope. — Marine JE. Journal of Electrocardiology. 2013.
17. Brugada Syndrome and Syncope: A Practical Approach for Diagnosis and Treatment. — Mascia G, Bona RD, Ameri P, et al. Europace : European Pacing, Arrhythmias, and Cardiac Electrophysiology : Journal of the Working Groups on Cardiac Pacing, Arrhythmias, and Cardiac Cellular Electrophysiology of the European Society of Cardiology. 2021.
18. Sudden Cardiac Death in Young Athletes: Practical Challenges and Diagnostic Dilemmas. — Chandra N, Bastiaenen R, Papadakis M, Sharma S. Journal of the American College of Cardiology. 2013.
19. Management of Ventricular Arrhythmias Worldwide: Comparison of the Latest ESC, AHA/ACC/HRS, and CCS/CHRS Guidelines. — Könemann H, Ellermann C, Zeppenfeld K, Eckardt L. JACC. Clinical Electrophysiology. 2023.
20. Development of Practice Recommendations Based on the Canadian Syncope Risk Score and Identification of Barriers and Facilitators for Implementation. — Hudek N, Brehaut JC, Rowe BH, et al. Cjem. 2023.