Temporal Bone Fracture
Temporal bone fractures result from high-energy blunt head trauma and are found in approximately 4.7% of skull fractures and 36% of skull base fractures.[1] They carry a mortality rate of ~8% and a…
Temporal bone fractures result from high-energy blunt head trauma and are found in approximately 4.7% of skull fractures and 36% of skull base fractures.[1] They carry a mortality rate of ~8% and are associated with critical neurovascular complications including hearing loss, facial nerve paralysis, CSF leak, and vascular injury.[1-3] Initial management follows ATLS principles, as these fractures rarely occur in isolation — 67% have additional skull fractures and 78% have associated intracranial hemorrhage.[1]
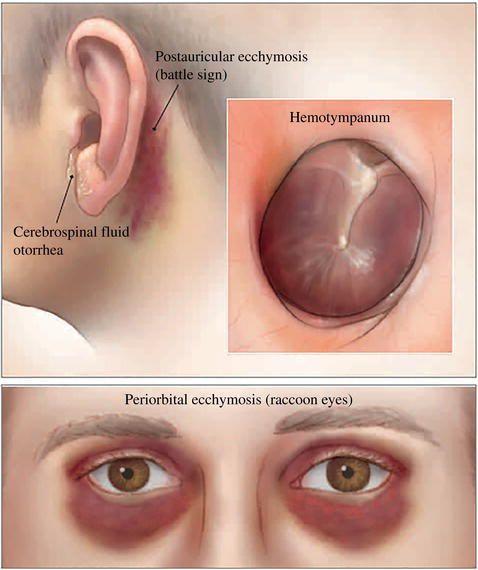
The following figure illustrates the classic physical exam findings of basilar skull fracture, which are frequently associated with temporal bone fractures:
View full figure Figure 1. Findings suggestive of basilar skull fractures are Battle sign, hemotympanum, cerebrospinal fluid otorrhea, or raccoon eyes. Adult Blunt Head Injury. Evidence‐Based Emergency Care. December 31, 2022.
1. History
- Mechanism: High-energy blunt trauma — motor vehicle collisions, falls (now the leading cause at ~42%), assaults, pedestrian-vehicle collisions[1][3]
- Laterality of impact: Lateral blows to temporal/parietal skull → longitudinal fractures; frontal/occipital blows → transverse fractures[5]
- Hearing changes: Acute hearing loss (unilateral), tinnitus, aural fullness
- Otologic symptoms: Bleeding from the ear, clear fluid from the ear or nose, vertigo/dizziness
- Facial weakness: Onset timing is critical — immediate vs. delayed facial weakness has different prognostic and management implications[6-7]
- Important negatives: Loss of consciousness, amnesia, seizure, neck pain, visual changes, other neurologic deficits
2. Alarm Features
- Immediate complete facial paralysis (House-Brackmann V–VI) — suggests nerve transection or severe compression; may require surgical exploration[6][8]
- Active CSF otorrhea or rhinorrhea — risk of ascending meningitis (meningitis rate 4.3% in otic capsule violating fractures)[9]
- Expanding hematoma or pulsatile bleeding from the ear — concern for vascular injury (internal carotid artery, sigmoid sinus)[2][10]
- Declining GCS or new focal neurologic deficits — associated intracranial hemorrhage requiring neurosurgical intervention[11]
- Bilateral temporal bone fractures — occur in ~22% of cases and indicate higher-energy mechanism[12]
- Signs of basilar skull fracture: Battle sign, raccoon eyes, hemotympanum — LR 16 for intracranial injury[11]
3. Medications
- High-dose corticosteroids: Recommended for facial nerve palsy (if not contraindicated by concurrent intracranial injury or polytrauma); however, administration in the setting of significant intracranial injury is not advised[7][13]
- Antiemetics: For acute vertigo (meclizine, ondansetron)
- Analgesics: Avoid NSAIDs acutely if concern for ongoing hemorrhage; acetaminophen preferred
- Antibiotics: Prophylactic antibiotics for CSF leak remain controversial; no strong evidence supports routine use
- Contraindicated: Ear drops through a perforated tympanic membrane (ototoxic aminoglycosides); nasal packing in CSF rhinorrhea
4. Diet
- NPO if surgical intervention anticipated or GCS depressed
- Stool softeners/avoid Valsalva if CSF leak present (to reduce intracranial pressure fluctuations)
- Hydration: Maintain euvolemia; avoid dehydration which may worsen vestibular symptoms
5. Review of Systems
- HEENT: Hearing loss, tinnitus, ear pain, ear drainage (bloody vs. clear), nasal drainage, facial asymmetry, taste changes (chorda tympani involvement)
- Neurologic: Headache, dizziness/vertigo, nausea/vomiting, vision changes, weakness, numbness, seizures, altered mental status
- Musculoskeletal: Neck pain, jaw pain (associated mandibular fractures)
- Psychiatric: Assess for intoxication (common in trauma population)
6. Collateral History and Family History
- Collateral: Witnesses to mechanism, loss of consciousness duration, anticoagulant/antiplatelet use, baseline neurologic function
- Social: Alcohol/substance use at time of injury (common contributor)
- Family history: Generally not relevant acutely; consider bleeding disorders if disproportionate hemorrhage
7. Risk Factors
- Demographics: Male predominance (~74%), mean age ~41 years[12][14]
- Mechanisms: Falls (especially elderly), MVCs, assaults, sports injuries
- Anticoagulation/antiplatelet therapy: Increases risk of intracranial hemorrhage
- Osteoporosis: Lower-energy mechanisms may cause fractures in elderly
- Alcohol intoxication: Common comorbidity in trauma, may mask symptoms and delay diagnosis[15]
8. Differential Diagnosis
- Isolated tympanic membrane perforation (without fracture)
- Mandibular condyle fracture (TMJ pain, malocclusion)
- Isolated intracranial hemorrhage without fracture
- Bell's palsy — must distinguish from traumatic facial nerve injury; history of trauma is key
- Benign paroxysmal positional vertigo — post-traumatic BPPV is common and may coexist
- Carotid artery dissection — can occur with temporal bone fractures or independently after head/neck trauma
- Cholesteatoma — delayed complication that can mimic recurrent symptoms
9. Past Medical History
- Prior ear surgery or hearing loss
- Previous head trauma
- Anticoagulant/antiplatelet use
- Bleeding disorders
- Prior neurosurgical procedures
- Chronic ear disease
10. Physical Exam
- Vital signs: Hemodynamic instability suggests polytrauma; hypertension/bradycardia (Cushing response) suggests elevated ICP
- Head: Palpate for step-offs, lacerations, depressed fractures
- Ear: Hemotympanum (most common finding, ~68% of cases), EAC lacerations, otorrhea (bloody vs. clear), TM perforation[11][16]
- Mastoid: Battle sign (postauricular ecchymosis — may take 24–48 hours to develop)
- Periorbital: Raccoon eyes (bilateral periorbital ecchymosis)
Cranial nerves
- CN VII (facial nerve): Assess all branches — forehead wrinkling, eye closure, smile, lip pucker; grade using House-Brackmann scale[6]
- CN VIII: Bedside hearing assessment (finger rub, whispered voice); Weber and Rinne tuning fork tests to differentiate conductive vs. sensorineural hearing loss
- CN V, VI: Less commonly affected but should be assessed
- Vestibular: Nystagmus, gait assessment (if patient is ambulatory)
- Neurologic: GCS, pupillary response, motor/sensory exam
11. Lab Studies
- Routine trauma labs: CBC, BMP, coagulation studies (PT/INR, PTT), type and screen
- Blood alcohol level and urine drug screen: Common in trauma workup
- Beta-2 transferrin: Gold standard to confirm CSF in ear/nasal drainage (send if clear otorrhea or rhinorrhea suspected)[3]
- Glucose testing of fluid: Bedside halo test or glucose level of drainage (less specific than beta-2 transferrin)
12. Imaging
- First-line: Non-contrast CT head — identifies 98.6% of temporal bone fractures on routine trauma CT. Evaluate for intracranial hemorrhage, pneumocephalus, fracture lines[1]
- Dedicated temporal bone CT (thin-section, 0.5–0.625 mm with multiplanar reconstructions): Indicated when facial nerve injury or vascular injury is suspected, or when routine CT is negative but clinical suspicion remains high[1-2]
- CT angiography (CTA): If fracture involves the carotid canal or there is concern for vascular injury (carotid dissection, sigmoid sinus thrombosis)[2][10]
- MRI: Reserved for evaluating facial nerve integrity, inner ear fluid signal changes, or encephalocele in subacute/chronic settings[10]
- Key imaging findings to evaluate: Otic capsule integrity, ossicular chain disruption, tegmen defects, facial nerve canal involvement, carotid canal involvement[10]
13. Special Tests
Classification Systems
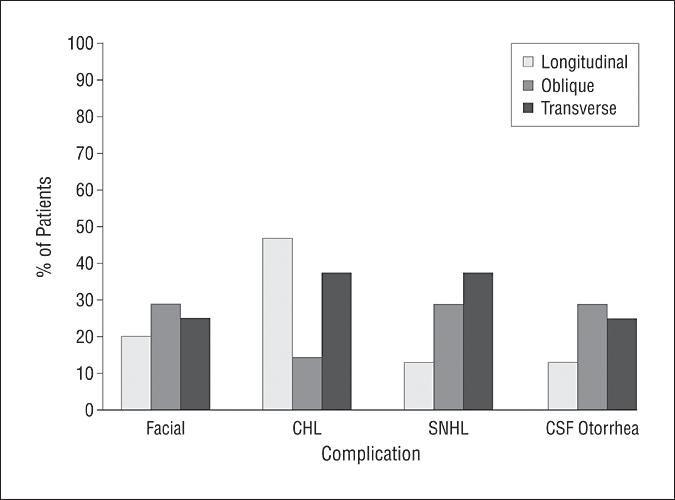
- Export Classification Categories Clinical Utility References Traditional Longitudinal (~75–80%), Transverse (~10–20%), Mixed Poor correlation with complications; longitudinal from lateral blows, transverse from frontal/occipital[1-2]
- Otic Capsule (preferred) Otic Capsule Sparing (OCS, ~90%) vs. Otic Capsule Violating (OCV, ~10%) OCV strongly predicts SNHL (OR 4.89), higher CSF leak and meningitis rates[3-4]
- Electroneurography (ENoG): Indicated for complete facial paralysis; >90% degeneration within 2 weeks suggests poor prognosis and may warrant surgical decompression[3][6]
- Electromyography (EMG): Assess for voluntary motor unit potentials; useful 2–3 weeks post-injury
- Audiometry: Formal audiogram once patient is stable — differentiates conductive vs. sensorineural vs. mixed hearing loss[9]
- Schirmer's test: Assesses lacrimation; helps localize facial nerve injury level[8]
14. ECG
- Not specifically indicated for temporal bone fracture itself
- Obtain per standard trauma protocols if polytrauma, hemodynamic instability, or elderly patient
- Monitor for arrhythmias if significant intracranial hypertension (Cushing reflex)
15. Assessment
- Severity stratification is driven by the otic capsule classification rather than the traditional longitudinal/transverse system:[9][17-18]
- Otic capsule sparing (OCS): ~90% of fractures. Functional hearing recovery (≥30 dB improvement) in 90.4% at 24 months. Conductive hearing loss predominates. Complication rate ~6%[9]
- Otic capsule violating (OCV): ~10% of fractures. 0% functional hearing recovery at 24 months. Complication rate ~31.5%, including CSF leak (13.8%) and meningitis (4.3%). Associated with irreversible sensorineural hearing loss and higher rates of facial nerve injury[9][19]
Key complications to anticipate
- Immediate: Intracranial hemorrhage, facial nerve paralysis, CSF leak, vascular injury
- Short-term: Hearing loss (CHL ~31%, SNHL ~13% in pediatric series), vertigo, meningitis[20]
- Delayed: Cholesteatoma, encephalocele, post-traumatic BPPV, late meningitis[3]
16. Treatment Plan
Initial Stabilization
- ATLS protocol; address life-threatening injuries first[3]
- Secure airway, C-spine precautions, treat intracranial hemorrhage
CSF Leak Management
- Conservative first: Head of bed elevation (30°), bed rest, avoid straining/nose blowing, stool softeners
- Most CSF leaks resolve spontaneously within 7–10 days[9][19]
- Lumbar drain if persistent beyond 7–14 days
- Surgical repair for refractory leaks[21]
Facial Nerve Injury
- Delayed-onset palsy (most common): High-dose corticosteroids (e.g., prednisone 1 mg/kg/day taper); excellent prognosis, >90% recover spontaneously[6-7]
- Immediate complete paralysis: Corticosteroids + serial ENoG monitoring. If >90% degeneration on ENoG within 2 weeks → consider surgical decompression[6][22]
- Surgical decompression ideally within 8 weeks of injury yields best outcomes (91.7% achieve HB I–II)[22]
- Eye care: Artificial tears, lubricating ointment, moisture chamber/taping at night to prevent exposure keratopathy[6]
Hearing Loss
- Conductive: Often from hemotympanum (resolves) or ossicular disruption (may require ossiculoplasty after 3–6 months)[8][19]
- Sensorineural: No proven medical treatment; consider hearing aids or cochlear implantation for severe/profound loss[9]
Vestibular Symptoms
- Post-traumatic BPPV: Epley maneuver
- Acute vestibular suppression: Short-term vestibular suppressants; early vestibular rehabilitation
17. Disposition
Admission criteria
- GCS < 15 or declining neurologic status
- Associated intracranial hemorrhage or polytrauma
- Active CSF leak
- Immediate facial nerve paralysis
- Otic capsule violating fracture
- Suspected vascular injury
- Need for neurosurgical monitoring
- Inpatient ENT/Otolaryngology consultation triggers (high sensitivity screening): Acute facial nerve paresis/paralysis, clear otorrhea, bloody otorrhea, or otic capsule involvement on CT — this approach captures 93.5% of patients with post-traumatic facial nerve dysfunction and 100% of CSF leaks[12]
Outpatient follow-up appropriate if
- Isolated OCS fracture without facial weakness, CSF leak, or significant otorrhea
- Neurologically intact (GCS 15)
- No other injuries requiring admission
- This approach can safely reduce inpatient ENT consults by ~43%[12]
18. Follow Up / Return Precautions
Follow-up timing
- ENT/Otolaryngology: Within 1–2 weeks for all temporal bone fractures; sooner if facial weakness or CSF leak
- Audiology: Formal audiogram once hemotympanum resolves (typically 4–6 weeks)
- Neurosurgery: As indicated for intracranial pathology
Return precautions — seek immediate care for
- New or worsening facial weakness
- Clear fluid draining from ear or nose (CSF leak)
- Fever, severe headache, neck stiffness (meningitis)
- Worsening hearing loss
- New-onset seizures
- Increasing dizziness or inability to ambulate
Patient counseling
- Keep ear dry; no water in the ear canal
- Do not insert anything into the ear canal
- Avoid nose blowing, straining, heavy lifting (if CSF leak concern)
- Hearing loss from hemotympanum typically improves over weeks as blood resorbs
- Delayed complications (cholesteatoma, late meningitis) can occur months to years later — long-term otologic follow-up is important[3]
Expected recovery
- OCS fractures: Excellent hearing recovery in ~90% at 24 months[9]
- OCV fractures: Hearing deficits are typically permanent[9]
- Delayed facial palsy: >90% spontaneous recovery[6]
- Immediate complete facial palsy with surgical decompression within 8 weeks: ~80–92% achieve HB I–II[8][22]
References
1. Temporal Bone Fracture: Evaluation in the Era of Modern Computed Tomography. — Schubl SD, Klein TR, Robitsek RJ, et al. Injury. 2016.
2. Temporal Bone Trauma and the Role of Multidetector CT in the Emergency Department. — Zayas JO, Feliciano YZ, Hadley CR, Gomez AA, Vidal JA. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2011.
3. Temporal Bone Fracture: Evaluation and Management in the Modern Era. — Johnson F, Semaan MT, Megerian CA. Otolaryngologic Clinics of North America. 2008.
4. Adult Blunt Head Injury. — Ian T. Ferguson, Christopher R. Carpenter Evidence‐Based Emergency Care. 2023.
5. Radiographic Classification of Temporal Bone Fractures: Clinical Predictability Using a New System. — Little SC, Kesser BW. Archives of Otolaryngology--Head & Neck Surgery. 2006.
6. Temporal Bone Fracture Related Facial Palsy: Efficacy of Decompression With and Without Grafting. — Natour A, Doyle E, DeDio R, Samy RN. Current Opinion in Otolaryngology & Head and Neck Surgery. 2024.
7. Management of Facial Nerve Trauma. — Greiner RC, Kohlberg GD, Lu GN. Current Opinion in Otolaryngology & Head and Neck Surgery. 2024.
8. Facial Nerve Decompression After Temporal Bone Fracture-the Bangalore Protocol. — Honnurappa V, Vijayendra VK, Mahajan N, Redleaf M. Frontiers in Neurology. 2019.
9. Audiometric and Vestibular Outcomes Following Temporal Bone Fractures: A Retrospective Analysis of a Major Trauma Center Cohort in China. — Wu C, He Q. Frontiers in Medicine. 2025.
10. Temporal Bone Trauma: Typical CT and MRI Appearances and Important Points for Evaluation. — Kurihara YY, Fujikawa A, Tachizawa N, et al. Radiographics : A Review Publication of the Radiological Society of North America, Inc. 2020.
11. Will Neuroimaging Reveal a Severe Intracranial Injury in This Adult With Minor Head Trauma?The Rational Clinical Examination Systematic Review. — Easter JS, Haukoos JS, Meehan WP, Novack V, Edlow JA. The Journal of the American Medical Association. 2015.
12. Management of Temporal Bone Fractures: Optimizing the Role of Otolaryngology Consultation. — Wen CZ, Pope P, Christou AS, et al. Otolaryngology--Head and Neck Surgery : Official Journal of American Academy of Otolaryngology-Head and Neck Surgery. 2026.
13. A Large Case Series of Temporal Bone Fractures at a UK Major Trauma Centre With an Evidence-Based Management Protocol. — Kanona H, Anderson C, Lambert A, et al. The Journal of Laryngology and Otology. 2020.
14. Our Experience on Temporal Bone Fractures: Retrospective Analysis of 141 Cases. — Ricciardiello F, Mazzone S, Longo G, et al. Journal of Clinical Medicine. 2021.
15. Incidence and Management of Facial Paralysis After Skull Base Trauma, an Administrative Database Study. — Wamkpah NS, Kallogjeri D, Snyder-Warwick AK, Buss JL, Durakovic N. Otology & Neurotology : Official Publication of the American Otological Society, American Neurotology Society European Academy of Otology and Neurotology. 2022.
16. Hearing Loss in Pediatric Temporal Bone Fractures: Evaluating Two Radiographic Classification Systems as Prognosticators. — Bhindi A, Carpineta L, Al Qassabi B, et al. International Journal of Pediatric Otorhinolaryngology. 2018.
17. Temporal Bone Fractures: Traditional Classification and Clinical Relevance. — Ishman SL, Friedland DR. The Laryngoscope. 2004.
18. Pediatric Temporal Bone Fractures: Current Trends and Comparison of Classification Schemes. — Dunklebarger J, Branstetter B, Lincoln A, et al. The Laryngoscope. 2014.
19. Clinical Characteristics and Management Outcomes of Pediatric Temporal Bone Fractures: A Retrospective Cohort Study. — Bulut O, Şevik Eliçora S, Erdem D. The Journal of Craniofacial Surgery. 2026.
20. Complications After Pediatric Temporal Bone Fractures by Classification System: A Systematic Review and Meta-Analysis. — Poupore NS, Britt AF, Nguyen SA, White DR. Otolaryngology--Head and Neck Surgery : Official Journal of American Academy of Otolaryngology-Head and Neck Surgery. 2024.
21. Endonasal Endoscopic and Hybrid Surgery Techniques for Blunt Trauma Fractures of the Skull Base With Cerebrospinal Fluid Leaks. — Palma Díaz M, Martínez Anda JJ, Guerrero Suarez PD, et al. The Journal of Craniofacial Surgery. 2021.
22. Management of Facial Palsy After Temporal Bone Fracture via the Transmastoid Approach. — Liu Y, Liu S, Li J, et al. Acta Oto-Laryngologica. 2015.