Third-Degree AV Block
Third-degree (complete) AV block is defined as the complete absence of AV conduction, with no atrial impulses reaching the ventricles. The heart depends entirely on a junctional or ventricular esca…
Third-degree (complete) AV block is defined as the complete absence of AV conduction, with no atrial impulses reaching the ventricles. The heart depends entirely on a junctional or ventricular escape rhythm for cardiac output. This is a potentially life-threatening conduction disturbance that almost always requires permanent pacemaker implantation unless attributable to a clearly reversible cause.[1-2]
1. History
- Syncope/presyncope: Most common presenting symptom; ask about sudden loss of consciousness, prodromal lightheadedness, or near-falls
- Exertional dyspnea, fatigue, exercise intolerance: Due to inability to augment heart rate
- Heart failure symptoms: Orthopnea, PND, lower extremity edema
- Chest pain: May indicate ischemic etiology (inferior or anterior MI)
- Palpitations: Awareness of slow or irregular heartbeat
- Timing: Acute onset (ischemia, drug toxicity) vs. insidious (degenerative, infiltrative)
- Medication history: Recent initiation or dose changes of AV nodal blocking agents
- Tick exposure, rash, travel: Lyme carditis in endemic areas[2]
- Recent cardiac surgery, catheter ablation, or TAVR[1]
2. Alarm Features
- Hemodynamic instability: Hypotension, altered mental status, signs of shock
- Ventricular escape rate <40 bpm or wide QRS escape rhythm (infra-Hisian origin — unreliable, may fail abruptly)[1-2]
- Asystolic pauses ≥3 seconds while awake[3-4]
- Associated acute MI (especially anterior — less likely to resolve)[1][5]
- Syncope or seizure-like activity (Stokes-Adams attacks)
- New heart failure or pulmonary edema
- Ventricular arrhythmias (pause-dependent VT/torsades)
3. Medications
Causative/contributing agents
- Beta-blockers, verapamil, diltiazem, digoxin
- Class I and III antiarrhythmics (flecainide, amiodarone, sotalol)
- Nutraceuticals (e.g., lily of the valley)
Acute treatment agents
- Atropine 0.5–1.0 mg IV (effective for AV nodal block; may worsen infranodal block — use judiciously with wide QRS)
- Epinephrine infusion (2–10 mcg/min) or push-dose (10–20 mcg boluses)
- Dopamine infusion (5–20 mcg/kg/min)
- Isoproterenol (enhances both nodal and His-Purkinje conduction)
- Aminophylline IV — may be considered in acute inferior MI[1]
- Glucagon — for beta-blocker toxicity
- Cautions: Atropine is unlikely to improve infranodal block and may paradoxically worsen conduction in patients with wide QRS complexes suggesting His-Purkinje disease.[1]
4. Diet
- No specific dietary triggers for complete heart block
- Ensure adequate hydration, especially in patients with low cardiac output
- Monitor potassium and magnesium — hyperkalemia can exacerbate conduction block[8]
- Digoxin toxicity risk increases with hypokalemia, hypomagnesemia, and hypercalcemia
5. Review of Systems
- Cardiovascular: Syncope, presyncope, dyspnea, chest pain, palpitations, exercise intolerance
- Neurologic: Dizziness, confusion, seizure-like episodes (Stokes-Adams)
- Pulmonary: Dyspnea on exertion, orthopnea (heart failure)
- Musculoskeletal: Muscle weakness (neuromuscular diseases — myotonic dystrophy, Kearns-Sayre)[1][9]
- Dermatologic: Erythema migrans (Lyme), malar rash (SLE)
- Constitutional: Fatigue, weight loss (sarcoidosis, malignancy)
- Rheumatologic: Joint pain, dry eyes/mouth (autoimmune etiologies)
6. Collateral History and Family History
- Family history: Sudden cardiac death, congenital heart block, cardiomyopathy, neuromuscular disease
- Maternal history: SLE or anti-Ro/La antibodies (congenital complete heart block)[1][9]
- Genetic conditions: SCN5A mutations, lamin A/C mutations, TRPM4[9]
- Social context: Outdoor activities in tick-endemic areas (Lyme), travel to Central/South America (Chagas)
- Collateral from witnesses: Observed syncope, seizure-like activity, duration of unresponsiveness
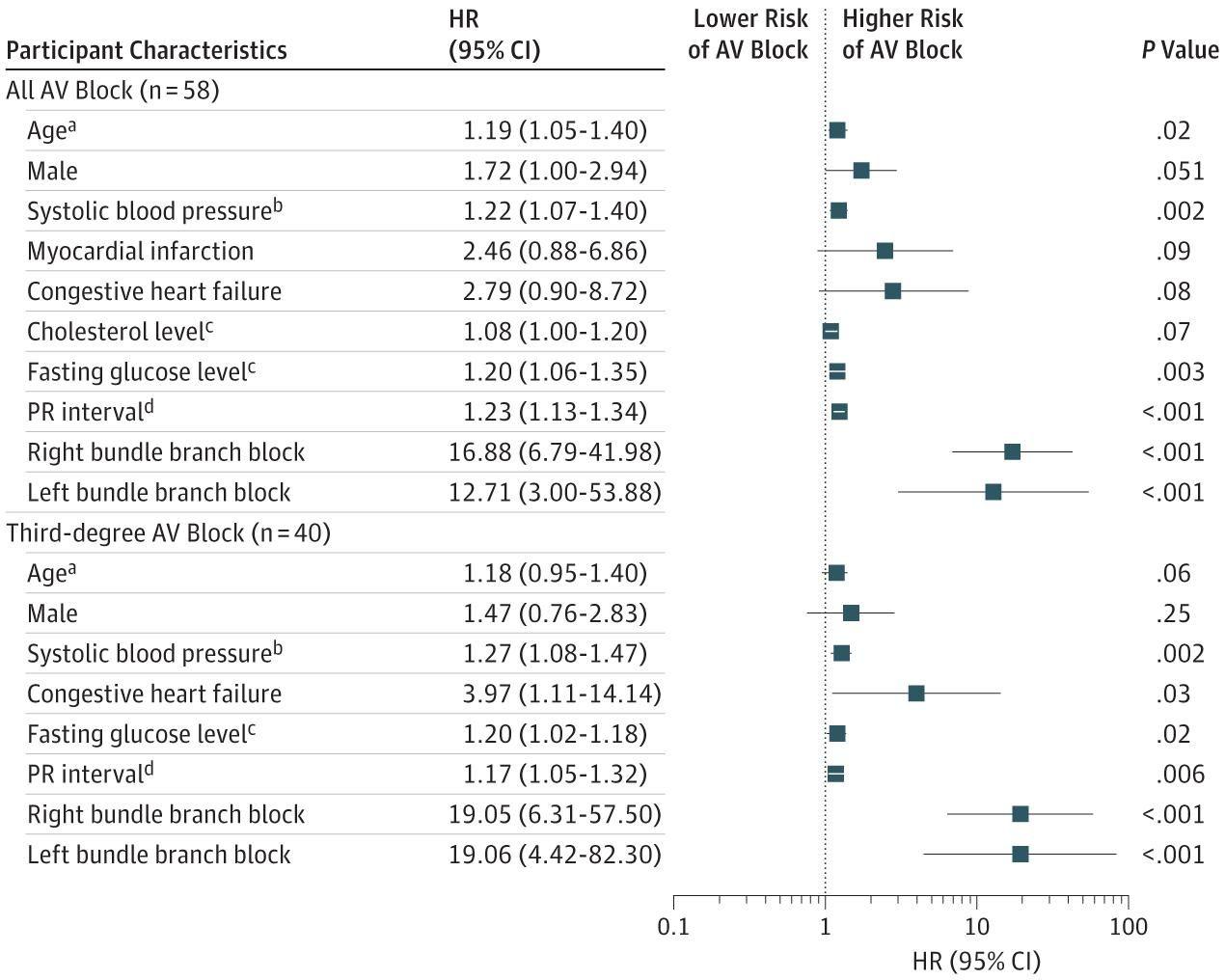
7. Risk Factors
- A population-based study identified the following independent risk factors for AV block:[10]
- Advanced age (degenerative fibrosis — Lev's/Lenegre's disease)
- Chronic hypertension and elevated systolic blood pressure
- Diabetes mellitus / elevated fasting glucose
- Pre-existing bundle branch block (RBBB or LBBB — strongest ECG predictors)
- Coronary artery disease / prior MI
- Structural heart disease (valvular, cardiomyopathy)
- AV nodal blocking medications
- Infiltrative diseases: Sarcoidosis (AV block in 23–30%), amyloidosis[9]
- Post-cardiac surgery (especially valve surgery) or TAVR[1]
- Neuromuscular diseases: Myotonic dystrophy, Kearns-Sayre syndrome[1]
- The following figure illustrates multivariable-adjusted hazard ratios for risk factors associated with AV block:
8. Differential Diagnosis
- Isorhythmic AV dissociation: Atrial and ventricular rates are similar but independent — not true block (no treatment needed)[1-2]
- High-grade (advanced) second-degree AV block: ≥2 consecutive non-conducted P waves but some conduction preserved[1]
- Sinus bradycardia with junctional escape: Sinus rate slower than junctional rate — not AV block
- Drug-induced AV block: Beta-blockers, CCBs, digoxin, antiarrhythmics — may be reversible[2][6]
- Hyperkalemia: Can mimic or cause complete heart block
- Acute MI: Inferior MI (AV nodal block, often transient) vs. anterior MI (infranodal, worse prognosis)[1]
- Lyme carditis: Reversible with antibiotics; median resolution 6 days[1-2]
- Cardiac sarcoidosis: May present with AV block as initial manifestation[9]
9. Past Medical History
- Prior conduction abnormalities (first-degree AV block, bundle branch block)
- History of MI, coronary artery disease, heart failure
- Prior cardiac surgery or catheter ablation
- Autoimmune/rheumatologic disease (SLE, sarcoidosis, RA)
- Neuromuscular disease
- Thyroid disease (both hypo- and hyperthyroidism)[8]
- Prior Lyme disease or tick-borne illness
- Medication list — especially AV nodal blocking agents
10. Physical Exam
- Vital signs: Bradycardia (typically 25–50 bpm), hypotension, may have normal or low BP
- Irregular cannon A waves in JVP (atrial contraction against closed tricuspid valve)[11]
- Varying intensity of S1 (hallmark — due to changing PR relationship)[11]
- Varying pulse volume[11]
- Signs of heart failure: Elevated JVP, pulmonary crackles, peripheral edema
- Skin: Erythema migrans (Lyme), malar rash (SLE), erythema nodosum (sarcoidosis)
- Neurologic: Muscle wasting, myotonia (neuromuscular disease)
- Focused exam: Assess perfusion (capillary refill, mental status, urine output)
11. Lab Studies
- Troponin: Rule out acute MI as cause
- BMP/CMP: Potassium (hyperkalemia), calcium, magnesium, renal function
- TSH: Hypothyroidism or hyperthyroidism[8]
- Digoxin level: If on digoxin therapy
- Lyme serologies: In endemic areas or with suggestive history[2]
- ESR/CRP, ANA, anti-Ro/La: If autoimmune etiology suspected
- ACE level, lysozyme: If sarcoidosis suspected (low sensitivity)
- BNP/NT-proBNP: Assess for heart failure
- CBC: Infection workup
12. Imaging
- Transthoracic echocardiography (TTE): First-line — assess LV function, wall motion abnormalities, valvular disease, infiltrative cardiomyopathy[11]
- Chest X-ray: Cardiomegaly, pulmonary congestion, hilar lymphadenopathy (sarcoidosis)
- Cardiac MRI: Gold standard for sarcoidosis (late gadolinium enhancement), myocarditis, infiltrative disease
- Coronary angiography: If ischemic etiology suspected[11]
- PET scan: Cardiac sarcoidosis evaluation
- Imaging is unnecessary when the etiology is clearly degenerative in an elderly patient with known conduction disease
13. Special Tests
- Electrophysiology study (EPS): Determines site of block (supra-Hisian, intra-Hisian, infra-Hisian) when not apparent from ECG; HV interval ≥70 ms suggests infranodal disease[2][5]
- Exercise stress testing: AV block worsening with exercise suggests infranodal disease (poor prognosis); supra-Hisian block typically improves with exercise[12]
- Ambulatory ECG monitoring (Holter/event monitor): For paroxysmal complete heart block
- Carotid sinus massage: If carotid sinus hypersensitivity suspected (with caution)
14. ECG
Diagnostic criteria
- AV dissociation: P waves and QRS complexes march independently at different rates
- Atrial rate > ventricular rate (P-P interval < R-R interval)
- Regular R-R intervals (escape rhythm is regular)
- No consistent PR interval (varying PR relationship)
Key features to assess
- Narrow QRS escape (≤120 ms): Suggests junctional (AV nodal) origin — more stable, rate ~40–60 bpm, may respond to atropine
- Wide QRS escape (>120 ms): Suggests ventricular (infranodal) origin — less reliable, rate ~20–40 bpm, higher risk of asystole[1-2]
- QTc prolongation: Risk for torsades de pointes
- ST changes: Concurrent ischemia
- In atrial fibrillation: Complete heart block is suggested by a slow (<50 bpm) and regular ventricular response[1-2]
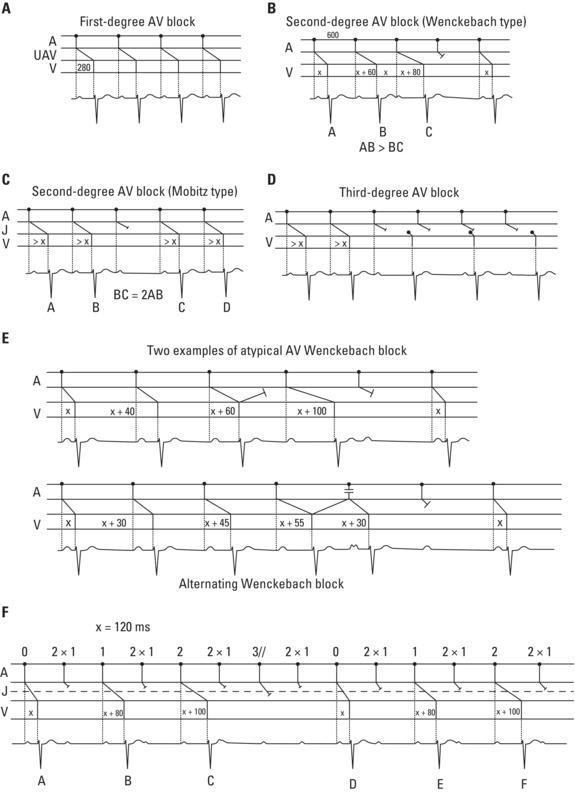
- The following figure illustrates the ECG patterns of different degrees of AV block, including third-degree block with AV dissociation (Panel D):
View full figure Figure 20. (A) First‐degree AV block. The PR interval is always prolonged (>200 ms); (B) second‐degree AV block 4 × 3 (Wenckebach type). The criterion AB > BC also applies in this case (see text and Figure B); (C) second‐degree AV block (Mobitz type) (BC = 2AB); (D) third‐degree AV block. A clear AV dissociation may be seen. After two QRS complexes have been conducted, there is a pause, followed by QRS (at slow frequencies) dissociated from P waves. In this case, the QRS complexes are junctional; (E) atypical Wenckebach blocks. Top: With abnormal lengthening of the increase preceding the pause (PR = x + 100) due to a concealed retrograde conduction of the preceding complex in the AV junction. Bottom: The abnormal PR shortening is due to the existence of a reciprocal complex in the AV junction; (F) example of an alternating Wenckebach block (see text). Mechanisms, Classification, and Clinical Aspects of Arrhythmias. Clinical Electrocardiography. December 31, 2020.
15. Assessment
Severity stratification depends on
- Hemodynamic stability: Stable vs. unstable (hypotension, altered mental status, shock)
- Escape rhythm characteristics: Narrow QRS (junctional) = more stable; wide QRS (ventricular) = high risk[1-2][14]
- Site of block: AV nodal block has slower progression and more reliable escape; infranodal block may progress rapidly and unpredictably[2][14]
- Etiology: Reversible (Lyme, drug toxicity, inferior MI) vs. irreversible (degenerative, post-surgical)
- Complications: Heart failure, ventricular arrhythmias, cardiogenic shock
- Third-degree AV block in the setting of anterior MI carries a worse prognosis than inferior MI, as it indicates extensive septal necrosis and infranodal block.[1][5]
16. Treatment Plan
Initial stabilization
- ABCs, IV access, continuous telemetry, transcutaneous pacing pads applied immediately
- Atropine 0.5–1.0 mg IV q3–5 min (max 3 mg) — for suspected AV nodal block (narrow QRS). Avoid or use cautiously with wide QRS escape
- If atropine fails: Transcutaneous pacing as bridge, or epinephrine/dopamine infusion
- Temporary transvenous pacing for refractory symptomatic bradycardia[7-8][15]
Definitive treatment
- Permanent pacemaker implantation is recommended (Class I) for acquired third-degree AV block not attributable to reversible or physiologic causes, regardless of symptoms[1-2]
- In patients with reversible causes (Lyme carditis, drug toxicity), treat the underlying cause first with temporary pacing support as needed; permanent pacing if block does not resolve[2][8]
- For cardiac sarcoidosis: Permanent pacing with consideration of ICD capability[2][8]
- For acute MI: Temporary pacing; permanent pacing only if block persists after revascularization[1]
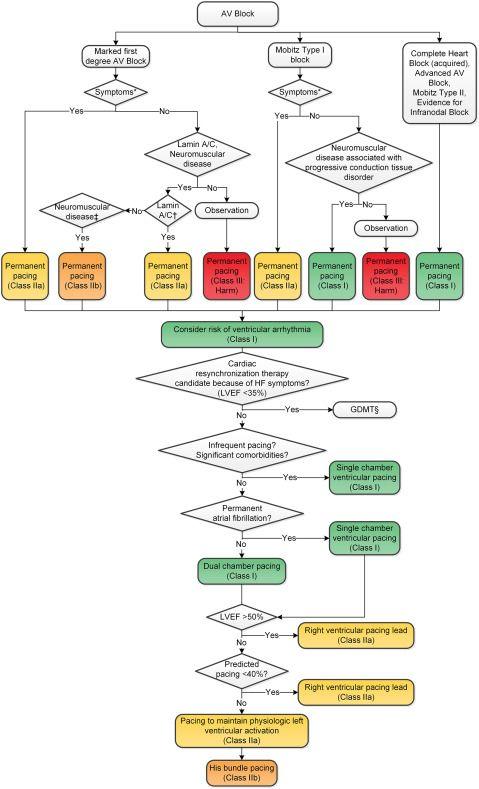
- The 2018 ACC/AHA/HRS guideline algorithm for management of chronic AV block is shown below:
View full figure Figure 7. Management of Bradycardia or Pauses Attributable to Chronic Atrioventricular Block Algorithm 2018 ACC/AHA/HRS Guideline on The Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. J Am Coll Cardiol. August 19, 2019.
17. Disposition
- All patients with third-degree AV block require admission with continuous telemetry monitoring[14]
- ICU/CCU admission: Hemodynamically unstable, requiring temporary pacing, or associated with acute MI
- Telemetry floor: Hemodynamically stable with reliable junctional escape, awaiting permanent pacemaker
- Cardiology/EP consultation: Required for all patients — for permanent pacemaker planning
- Discharge: Only after permanent pacemaker implantation or after confirmed resolution of a reversible cause with appropriate follow-up
- Distal (infranodal) block requires arrhythmia monitoring until pacemaker implantation, as it can progress rapidly and unpredictably and has been associated with sudden death[14]
18. Follow Up / Return Precautions
Post-pacemaker implantation
- Device check at 2–12 weeks, then every 6–12 months (or per remote monitoring schedule)
- Wound check at 1–2 weeks
- Activity restrictions for 4–6 weeks (avoid raising ipsilateral arm above shoulder)
- Return precautions (pre-pacemaker or if discharged with reversible cause):
- Return immediately for syncope, presyncope, severe dizziness, chest pain, or dyspnea
- New or worsening heart failure symptoms
- Palpitations or awareness of very slow heart rate
Expected course
- Lyme carditis: AV block typically resolves within 1–2 weeks of antibiotics (median 6 days, range up to 42 days)[1-2]
- Inferior MI: AV block often resolves within days to weeks[1]
- Degenerative/irreversible causes: Permanent pacemaker provides definitive treatment with excellent long-term outcomes[2]
References
1. 2018 ACC/AHA/HRS Guideline on The Evaluation and Management Of Patients With Bradycardia and Cardiac Conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Kusumoto FM, Schoenfeld MH, Barrett C, et al. Journal of the American College of Cardiology. 2019.
2. 2018 ACC/AHA/HRS Guideline on The evaluation and Management Of patients With Bradycardia and Cardiac conduction Delay: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Writing Committee Members, Kusumoto FM, Schoenfeld MH, et al. Heart Rhythm. 2019.
3. 2012 ACCF/AHA/HRS Focused Update Incorporated Into the ACCF/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Heart Rhythm Society. — Epstein AE, DiMarco JP, Ellenbogen KA, et al. Journal of the American College of Cardiology. 2013.
4. ACC/AHA/HRS 2008 Guidelines for Device-Based Therapy of Cardiac Rhythm Abnormalities: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guideline Update for Implantation of Cardiac Pacemakers and Antiarrhythmia Devices) Developed in Collaboration With the American Association for Thoracic Surgery and Society of Thoracic Surgeons. — Epstein AE, DiMarco JP, Ellenbogen KA, et al. Journal of the American College of Cardiology. 2008.
5. Pacemakers. — Aldaas OM, Roberge-Lacharite AS, Birgersdotter-Green U. NEJM Evidence. 2025.
6. Clinical Significance and Management of Atrioventricular Block Associated With Bradycardic/Antiarrhythmic Drug Therapy: Drug‐Induced or Drug‐Revealed?. — Sfairopoulos D, Bazoukis G, Sideris S, et al. Journal of Cardiovascular Electrophysiology. 2025.
7. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Wigginton JG, Agarwal S, Bartos JA, et al. Circulation. 2025.
8. 2018 ACC/AHA/HRS Guideline on The evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. — Writing Committee Members, Kusumoto FM, Schoenfeld MH, et al. Heart Rhythm. 2019.
9. Etiology and device therapy in complete atrioventricular block in pediatric and young adult population: Contemporary review and new perspectives. — Cioffi GM, Gasperetti A, Tersalvi G, et al. Journal of Cardiovascular Electrophysiology. 2021.
10. Risk Factors Associated With Atrioventricular Block. — Kerola T, Eranti A, Aro AL, et al. JAMA Network Open. 2019.
11. An Unusual Cause of Atrioventricular Block. — Rajendran K, Alphonse AJ, Desabandhu V. JAMA Internal Medicine. 2025.
12. 2021 PACES Expert Consensus Statement on the Indications and Management of Cardiovascular Implantable Electronic Devices in Pediatric Patients. — Writing Committee Members, Shah MJ, Silka MJ, et al. Heart Rhythm. 2021.
13. Mechanisms, Classification, and Clinical Aspects of Arrhythmias. — Antoni Bayés De Luna, Miquel Fiol‐Sala, Antoni Bayés‐Genís, et al. Clinical Electrocardiography. 2021.
14. Update to Practice Standards for Electrocardiographic Monitoring in Hospital Settings: A Scientific Statement From the American Heart Association. — Sandau KE, Funk M, Auerbach A, et al. Circulation. 2017.
15. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Panchal AR, Bartos JA, Cabañas JG, et al. Circulation. 2020.
16. 2018 ACC/AHA/HRS Guideline on The Evaluation and Management of Patients With Bradycardia and Cardiac Conduction Delay: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. — Kusumoto FM, Schoenfeld MH, Barrett C, et al. Journal of the American College of Cardiology. 2019.