Torsades de Pointes
Torsades de pointes is a life-threatening polymorphic ventricular tachycardia occurring in the setting of QT prolongation, characterized by a distinctive waxing and waning QRS amplitude ("twisting…
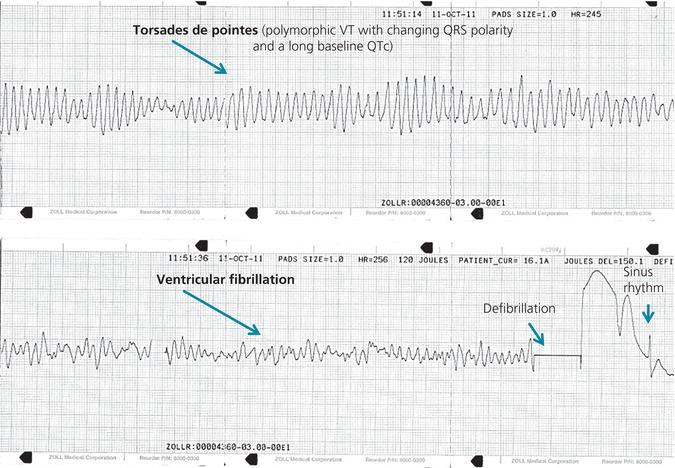
Torsades de pointes is a life-threatening polymorphic ventricular tachycardia occurring in the setting of QT prolongation, characterized by a distinctive waxing and waning QRS amplitude ("twisting of the points") around the isoelectric baseline.[1-3] It typically presents as recurrent, self-terminating salvos of hemodynamically unstable VT, often with associated bradycardia, but can degenerate into ventricular fibrillation and sudden cardiac death.[1-2]
The following ECG strip demonstrates TdP degenerating into VF, followed by successful defibrillation back to sinus rhythm:
1. History
- Presenting symptoms: Palpitations, dizziness, lightheadedness, presyncope, syncope, or cardiac arrest[2]
- Timing: Episodes are often paroxysmal and self-terminating (usually <30 seconds), but may cluster ("electrical storm")[1][5]
- Triggers: Recent medication changes (new QT-prolonging drug, dose increase), vomiting/diarrhea (electrolyte depletion), fasting, recent hospitalization
- Medication history: Detailed review of all prescription, OTC, and herbal medications — specifically QT-prolonging agents[6]
- Important negatives: Chest pain (ischemia-related polymorphic VT), exertional triggers (catecholaminergic polymorphic VT), family history of sudden death (congenital LQTS)
2. Alarm Features
- Sustained TdP or degeneration to VF — immediate defibrillation required[1]
- Recurrent episodes despite initial treatment — suggests refractory electrical storm[5]
- QTc >500 ms — high-risk threshold for TdP[6-7]
- QTc increase ≥60 ms from baseline after drug initiation[6-7]
- T-wave alternans (macroscopic) — sign of electrical instability and impending TdP[7]
- New ventricular ectopy with "short-long-short" initiating sequences[7-8]
- Hemodynamic instability: Hypotension, altered mental status, signs of cardiogenic shock
3. Medications
- Common culprit drug classes (known TdP risk per CredibleMeds/AHA):[6][9-10]
- Antiarrhythmics: Sotalol, dofetilide, quinidine, procainamide, ibutilide, dronedarone, amiodarone (lower risk)
- Antibiotics: Erythromycin, clarithromycin, azithromycin, moxifloxacin, levofloxacin, fluconazole, pentamidine
- Antipsychotics: Haloperidol, thioridazine, chlorpromazine, pimozide
- Antidepressants: Citalopram, escitalopram
- Others: Methadone, ondansetron, droperidol, cocaine, domperidone
Contraindicated in TdP
- All QT-prolonging antiarrhythmics — can worsen the arrhythmia[1][11]
- Acute β-blockers in acquired TdP — may precipitate bradycardia and worsen TdP (note: β-blockers ARE first-line for congenital LQTS)[1]
- Concomitant use of ≥2 QT-prolonging drugs[6]
Treatment medications
- IV magnesium sulfate 1–2 g (first-line, even with normal serum Mg)[1][5][12]
- Isoproterenol (for acquired LQTS with bradycardia-dependent TdP; avoid in congenital LQTS)[12-13]
- Mexiletine 200–450 mg/day (for refractory cases, especially LQT3)[6][13]
- Lidocaine (may be considered in refractory cases)[13]
4. Diet
- Electrolyte-rich diet — maintain adequate potassium and magnesium intake
- Avoid excessive alcohol — can cause electrolyte depletion and QT prolongation
- Grapefruit juice — inhibits CYP3A4, can increase levels of QT-prolonging drugs
- Correct dehydration aggressively — vomiting, diarrhea, and poor oral intake are common precipitants of hypokalemia/hypomagnesemia
5. Review of Systems
- Cardiovascular: Palpitations, syncope, presyncope, chest pain
- Neurological: Seizure-like activity (may mimic TdP-related syncope), altered consciousness
- GI: Nausea, vomiting, diarrhea (electrolyte losses)
- Endocrine: Symptoms of hypothyroidism (associated with QT prolongation)
- Psychiatric: Medication use for depression, psychosis, anxiety (many are QT-prolonging)
6. Collateral History and Family History
- Family history of sudden cardiac death, unexplained drowning, or seizures in young family members → raises suspicion for congenital LQTS[1]
- Family history of syncope or known LQTS — nearly 30% of drug-induced TdP patients carry mutations in major LQTS genes[6]
- Collateral from pharmacy — complete medication reconciliation including recently discontinued drugs
- Social history: Methadone use, cocaine use, nutritional status
7. Risk Factors
- Per the AHA Scientific Statement, drug-induced TdP is rare without risk factors:[6]
- QTc >500 ms or QTc increase ≥60 ms from baseline
- Female sex (longer baseline QTc)
- Age >65 years
- Bradycardia
- Acute myocardial infarction
- Hypokalemia, hypomagnesemia, hypocalcemia
- Heart failure with reduced ejection fraction
- Concomitant ≥2 QT-prolonging drugs
- History of prior drug-induced TdP
- Renal or hepatic impairment (impaired drug clearance)
- Genetic predisposition (subclinical congenital LQTS)[6]
- Rapid IV administration of QT-prolonging drugs[6]
8. Differential Diagnosis
- The critical distinction is between TdP and other causes of polymorphic VT, as treatment differs significantly:[1][14]
- Polymorphic VT without QT prolongation (ischemic) — most common cause; triggered by acute MI/ischemia; treat with β-blockers, revascularization, amiodarone/lidocaine (magnesium NOT effective without long QT)[1][11]
- Catecholaminergic polymorphic VT (CPVT) — exercise/emotion-triggered, normal QT; treat with β-blockers, flecainide[1]
- Ventricular fibrillation — may be difficult to distinguish from sustained TdP; both require defibrillation[1]
- Short QT syndrome — polymorphic VT with QTc <330–370 ms[1]
- Bidirectional VT — alternating QRS axis, classic for digitalis toxicity[1]
- "Pseudo-TdP" — polymorphic VT with mildly prolonged QT but short coupling interval; behaves like ischemic polymorphic VT, not true TdP[14]
- Short-coupled VF — initiated by very short-coupled PVCs, normal QT[1]
- Key distinguishing feature: The baseline QTc interval (measured when NOT in VT) is the most critical diagnostic feature — TdP requires QT prolongation.[1] The coupling interval of the initiating PVC also helps: true TdP has a long coupling interval (~580 ms) vs. short-coupled polymorphic VT (~360 ms).[14]
9. Past Medical History
- Prior episodes of TdP or drug-induced QT prolongation
- Congenital LQTS (personal or family diagnosis)
- Structural heart disease, heart failure (reduced repolarization reserve)
- Chronic kidney disease or liver disease (impaired drug metabolism)
- Hypothyroidism, anorexia nervosa (electrolyte/metabolic derangements)
- History of bradyarrhythmias, heart block, or pacemaker
10. Physical Exam
- Vitals: Bradycardia (common precipitant), hypotension during episodes, tachycardia during VT
- Cardiovascular: Irregular rhythm, signs of heart failure (JVD, edema, rales), murmurs suggesting structural disease
- Neurological: Post-syncopal confusion, signs of anoxic injury if prolonged arrest
- General: Signs of dehydration, malnutrition, thyroid disease
11. Lab Studies
- Stat electrolytes: K⁺, Mg²⁺, Ca²⁺ — critical[1][6][12]
- Target K⁺ ≥4.0 mEq/L (some guidelines suggest 4.5–5.0 mEq/L)[12-13]
- Target Mg²⁺ ≥2.0 mg/dL[6]
- Renal function (BUN/Cr) — affects drug clearance
- Hepatic function — affects drug metabolism
- Troponin — rule out acute MI as cause of polymorphic VT
- TSH — hypothyroidism can prolong QT
- Drug levels when applicable (digoxin, antiarrhythmics, methadone)
- Toxicology screen if overdose suspected
12. Imaging
- Echocardiogram — assess for structural heart disease, LV function (HFrEF is a risk factor)[6]
- Chest X-ray — evaluate for pulmonary edema, cardiomegaly
- Coronary angiography — if acute ischemia suspected as cause of polymorphic VT (non-TdP)[1]
- Imaging is not diagnostic for TdP itself — diagnosis is electrocardiographic
13. Special Tests
- Tisdale Risk Score — validated tool for predicting QT prolongation risk in hospitalized patients[7]
- CredibleMeds QT drug lists (www.crediblemeds.org) — essential resource for identifying culprit medications[6][15]
- Genetic testing — consider for suspected congenital LQTS (not currently recommended for routine screening of drug-induced TdP)[3][6]
- Schwartz Score — clinical diagnostic criteria for congenital LQTS
- Epinephrine QT stress test — may unmask latent LQTS in select cases
14. ECG
Diagnostic ECG findings
- Prolonged QTc interval (measured during sinus rhythm, NOT during VT) — QTc >500 ms is high-risk
- Polymorphic VT with characteristic "twisting of the points" — waxing and waning QRS amplitude
- "Short-long-short" initiating sequence — PVC → compensatory pause → another PVC triggering TdP[8]
- T-wave alternans — beat-to-beat variation in T-wave morphology (sign of impending TdP)[7]
- T-U wave distortion accentuated after pauses[7]
- Bradycardia — often present at baseline
Dangerous patterns to recognize
- QTc >500 ms on any ECG
- New ventricular ectopy with couplets or NSVT after pauses
- Degeneration of TdP into VF
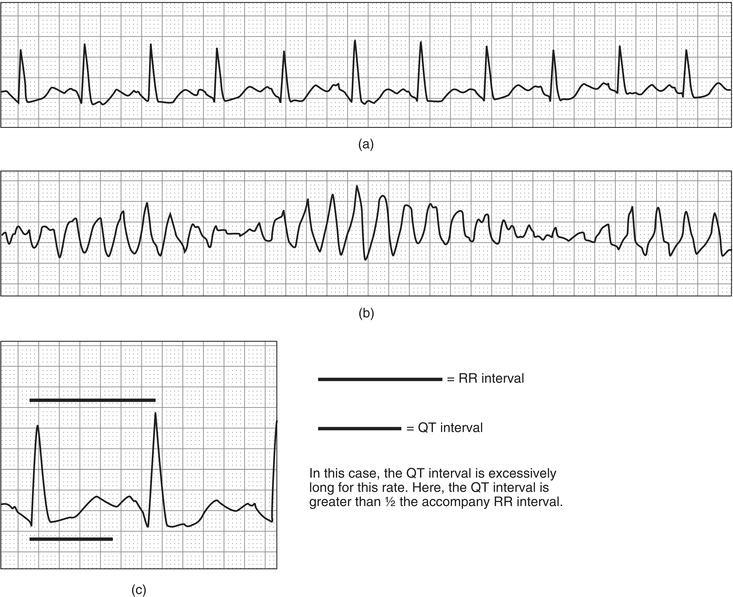
- The following figure illustrates the progression from QT prolongation to TdP:
15. Assessment
- TdP is a medical emergency that requires immediate recognition and treatment. The clinical summary should address:
- Acquired vs. congenital — acquired (drug-induced) is far more common; treatment strategies differ[9]
- Severity: Self-terminating salvos vs. sustained TdP vs. VF
- Precipitant identification: Offending drug, electrolyte abnormality, bradycardia, or combination
- Typical presentation: Recurrent self-terminating episodes of dizziness/syncope with polymorphic VT on monitor, often in a hospitalized patient recently started on a QT-prolonging drug[2]
- Atypical: May present as "seizure" (actually syncopal TdP), unexplained cardiac arrest, or isolated QT prolongation without overt arrhythmia
- Complications: VF, sudden cardiac death, anoxic brain injury, cardiogenic shock
16. Treatment Plan
Immediate stabilization
- Sustained/pulseless TdP → Unsynchronized defibrillation at maximum energy (synchronized cardioversion is unreliable for polymorphic VT)[1]
- IV magnesium sulfate 1–2 g over 1–2 minutes, may repeat; effective even with normal serum Mg[1][5][12]
- Discontinue ALL QT-prolonging drugs immediately[6][13]
- Correct electrolytes: K⁺ to ≥4.0 mEq/L (consider 4.5–5.0), Mg²⁺ to ≥2.0 mg/dL[6][12]
Recurrent/refractory TdP
- Overdrive pacing (transvenous, atrial or ventricular) at 90–110 bpm — eliminates pauses and shortens QT; highly effective[3][12]
- Isoproterenol infusion (2–10 mcg/min) — temporizing measure to increase heart rate while awaiting pacing; avoid in congenital LQTS[1][13][17]
- Mexiletine 200–450 mg/day PO — for refractory cases, particularly LQT2 and LQT3[6][13]
- Lidocaine IV — may be considered as adjunct[13]
- Critical pitfall: Do NOT treat TdP with standard antiarrhythmics (amiodarone, procainamide, sotalol) — these prolong QT and will worsen TdP. β-blockers given acutely can also worsen bradycardia-dependent TdP.[1][11]
17. Disposition
- All TdP episodes require admission — typically to a cardiac ICU or telemetry unit with continuous monitoring and immediate defibrillation capability[7]
- ICU admission criteria: Sustained TdP, recurrent episodes, hemodynamic instability, need for overdrive pacing or isoproterenol, electrical storm[5]
- Telemetry admission: Single self-terminating episode with identified and corrected precipitant, stable hemodynamics
- Electrophysiology consultation — recommended for all cases, especially recurrent TdP, suspected congenital LQTS, or refractory arrhythmia[1][12]
- Cardiology consultation — for structural heart disease evaluation, consideration of ICD if congenital LQTS
18. Follow Up / Return Precautions
Before discharge
- QTc should be trending toward normal and stable
- Offending drug permanently discontinued with documentation in allergy/adverse reaction list
- Electrolytes normalized and stable
- Comprehensive medication reconciliation to avoid future QT-prolonging drugs
Outpatient follow-up
- Cardiology/EP follow-up within 1–2 weeks
- 12-lead ECG at follow-up to confirm QTc normalization
- If congenital LQTS suspected → genetic testing and family screening[6]
- Patients on long-term QT-prolonging drugs should have ECG monitoring every 3–6 months[6]
Return precautions — counsel patients on
- Return immediately for palpitations, dizziness, near-syncope, syncope, or seizure-like episodes
- Avoid all QT-prolonging medications (provide written list; reference www.crediblemeds.org)[6][15]
- Maintain adequate hydration and electrolyte intake; seek care during illness with vomiting/diarrhea
- Expected recovery: If acquired and precipitant removed, QTc typically normalizes within days; prognosis is excellent with appropriate management[2]
References
1. Part 9: Adult Advanced Life Support: 2025 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Wigginton JG, Agarwal S, Bartos JA, et al. Circulation. 2025.
2. Pharmacological Treatment of Acquired QT Prolongation and Torsades De Pointes. — Thomas SH, Behr ER. British Journal of Clinical Pharmacology. 2016.
3. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Journal of the American College of Cardiology. 2018.
4. Ventricular Arrhythmias. — Elias Hanna Practical Cardiovascular Medicine 2e. 2022.
5. Multidisciplinary Critical Care Management of Electrical Storm: JACC State-of-the-Art Review. — Jentzer JC, Noseworthy PA, Kashou AH, et al. Journal of the American College of Cardiology. 2023.
6. Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association. — Tisdale JE, Chung MK, Campbell KB, et al. Circulation. 2020.
7. Prevention of Torsade De Pointes in Hospital Settings: A Scientific Statement From the American Heart Association and the American College of Cardiology Foundation. — Drew BJ, Ackerman MJ, Funk M, et al. Circulation. 2010.
8. Ventricular Tachycardia Due to Triggered Activity: Role of Early and Delayed Afterdepolarizations. — Lerman BB, Markowitz SM, Cheung JW, Thomas G, Ip JE. JACC. Clinical Electrophysiology. 2024.
9. Update on long QT syndrome. — Neira V, Enriquez A, Simpson C, Baranchuk A. Journal of Cardiovascular Electrophysiology. 2019.
10. Drugs That May Cause or Exacerbate Heart Failure: A Scientific Statement From the American Heart Association. — Page RL, O'Bryant CL, Cheng D, et al. Circulation. 2016.
11. Part 3: Adult Basic and Advanced Life Support: 2020 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. — Panchal AR, Bartos JA, Cabañas JG, et al. Circulation. 2020.
12. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. — Al-Khatib SM, Stevenson WG, Ackerman MJ, et al. Heart Rhythm. 2018.
13. ACC/AHA/ESC 2006 Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Association Task Force and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Develop Guidelines for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death). — European Heart Rhythm Association, Heart Rhythm Society, Zipes DP, et al. Journal of the American College of Cardiology. 2006.
14. Polymorphic Ventricular Tachycardia, Ischaemic Ventricular Fibrillation, and Torsade De Pointes: Importance of the QT and the Coupling Interval in the Differential Diagnosis. — Rosso R, Hochstadt A, Viskin D, et al. European Heart Journal. 2021.
15. Predicting the Unpredictable: Drug-Induced QT Prolongation and Torsades De Pointes. — Schwartz PJ, Woosley RL. Journal of the American College of Cardiology. 2016.
16. The Electrocardiogram in the Poisoned Patient. — Steven H. Mitchell, Christopher P. Holstege, William J. Brady The Electrocardiagram in Emergency and Acute Care. 2023.
17. Acute Management of Ventricular Arrhythmia In Patients With Suspected Inherited Heart Rhythm Disorders. — Laksman Z, Barichello S, Roston TM, Deyell MW, Krahn AD. JACC. Clinical Electrophysiology. 2019.