Toxic Epidermal Necrolysis (TEN)
Toxic epidermal necrolysis is a life-threatening, delayed-type hypersensitivity reaction characterized by ≥30% body surface area (BSA) epidermal detachment, widespread mucosal erosions, and systemi…
Toxic epidermal necrolysis is a life-threatening, delayed-type hypersensitivity reaction characterized by ≥30% body surface area (BSA) epidermal detachment, widespread mucosal erosions, and systemic toxicity, with mortality rates of 25–50%.[1-3] It represents the most severe end of the SJS/TEN spectrum and is a true dermatologic emergency requiring immediate recognition, drug withdrawal, and transfer to a burn/ICU center.[4-5]
The following figure illustrates the clinical spectrum from SJS to TEN based on extent of epidermal detachment:
1. History
- Medication exposure within 4–28 days is the single most critical HPI element — obtain a complete drug list including new prescriptions, OTCs, and supplements[2][7]
- Prodromal phase: 1–3 days of fever, malaise, myalgias, sore throat, cough ("flu-like" symptoms) preceding skin findings[1][7]
- Skin pain often described as burning, disproportionate to visible findings early on
- Mucosal symptoms: odynophagia, dysuria, eye pain/photophobia, genital pain[7]
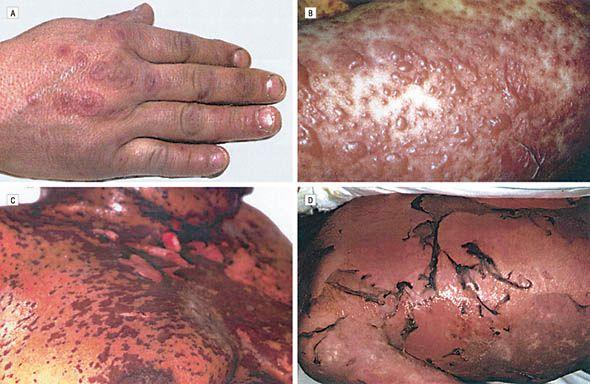
- Progression: erythematous macules → atypical targetoid lesions → confluent blisters → sheet-like epidermal sloughing[7]
- Ask about prior episodes of SJS/TEN, known drug allergies, and any recent infections (especially Mycoplasma pneumoniae)[8-9]
2. Alarm Features
- Rapidly progressive skin detachment (>10% BSA and expanding)
- Positive Nikolsky sign (epidermis sloughs with lateral pressure on erythematous skin)[2][10]
- Mucosal involvement of ≥2 sites (oral, ocular, genital)[7]
- Respiratory distress — suggests bronchial epithelial involvement or aspiration[7]
- Hemodynamic instability, high-output fluid losses
- Signs of sepsis (leading cause of death in TEN)[1][7]
- Altered mental status, oliguria, or DIC[11]
3. Medications
- High-risk culprit drugs (onset typically 4–28 days after initiation):[1][8][12]
- Anticonvulsants: carbamazepine, phenytoin, lamotrigine, phenobarbital
- Allopurinol
- Sulfonamide antibiotics: TMP-SMX
- NSAIDs (oxicam type especially)
- Antibiotics: β-lactams, fluoroquinolones, cephalosporins
- Others: nevirapine, immune checkpoint inhibitors[13]
- Contraindicated: Thalidomide — an RCT was stopped early due to increased mortality in TEN.[14] Prophylactic systemic antibiotics are not recommended without evidence of infection.[5]
Systemic therapies (controversial, no consensus)
- Cyclosporine 3–5 mg/kg/day (some evidence of mortality benefit vs. IVIG)[7][15]
- Systemic corticosteroids (pulse methylprednisolone 1–2 mg/kg/day)[7][13]
- IVIG 2 g/kg over 2–5 days[13][16]
- Etanercept (single dose 25–50 mg SC) — emerging data showing possible benefit[7][15][17]
4. Diet
- NPO initially if significant oral mucosal involvement or airway concerns
- Early enteral nutrition via NG/NJ tube if unable to tolerate PO — critical for wound healing and metabolic demands[5]
- High-calorie, high-protein diet (similar to burn nutrition protocols)[5]
- Aggressive IV fluid resuscitation — use burn-like fluid calculations but typically less than equivalent BSA burns (Parkland formula adjusted to ~2/3 of burn estimates)[5]
- Gastric ulcer prophylaxis recommended[5]
5. Review of Systems
- Skin: rash distribution, blistering, pain, peeling
- Eyes: redness, tearing, photophobia, blurred vision, discharge (ocular involvement in 40–84% of cases)[18]
- Oral: odynophagia, oral erosions, inability to eat/drink
- GU: dysuria, genital erosions, urinary retention
- Respiratory: cough, dyspnea, stridor (bronchial epithelial sloughing)
- GI: diarrhea, abdominal pain (GI mucosal involvement)
- Constitutional: fever, malaise, weight loss
- Psychiatric: anxiety, fear (PTSD develops in ~30–50% of survivors)[7][19]
6. Collateral History and Family History
- Confirm exact medication names, doses, and start dates from pharmacy records
- Prior drug allergies or adverse drug reactions — previous drug allergy is a significant risk factor (OR 5.21)[12]
- Family history of SJS/TEN or drug hypersensitivity reactions
Ethnic background — relevant for HLA-associated risk
- HLA-B15:02: carbamazepine-induced SJS/TEN (Southeast Asian/Han Chinese ancestry)[7][20]
- HLA-B58:01: allopurinol-induced SJS/TEN (higher prevalence in Black and Asian populations)[21]
- HLA-A31:01: carbamazepine-induced SCARs (Northern European, Japanese)[7][20]
- HIV status (increased SJS/TEN risk)[6]
7. Risk Factors
- New medication within past 4–28 days (most important risk factor)[2]
- HIV/AIDS (100-fold increased incidence)[3]
- Active malignancy[12][22]
- Autoimmune disease: SLE (OR 17.41), psoriasis (OR 10.28)[12]
- Prior drug allergies (OR 5.21)[12]
- Epilepsy (OR 4.92 — likely confounded by anticonvulsant use)[12]
- Diabetes mellitus, history of CVA[12]
- Genetic susceptibility (HLA alleles as above)[7]
- Slow acetylator phenotype[3]
- Concurrent radiation therapy
8. Differential Diagnosis
- Staphylococcal scalded skin syndrome (SSSS): superficial (subcorneal) cleavage plane vs. full-thickness necrosis in TEN; no mucosal involvement; more common in infants; Nikolsky sign positive but biopsy distinguishes[23-24]
- Erythema multiforme major: typical target lesions with 3 concentric rings, acral distribution, often HSV-related[6-7]
- Generalized bullous fixed drug eruption (GBFDE): well-demarcated round plaques, eosinophils on biopsy, dermal melanophages[23]
- Acute graft-versus-host disease: requires transplant history; satellite cell necrosis on biopsy[23]
- Linear IgA bullous dermatosis: positive direct immunofluorescence (linear IgA at BMZ)[7][23]
- Paraneoplastic pemphigus: positive DIF distinguishes[24]
- AGEP: subcorneal pustules, less mucosal involvement[24]
- Autoimmune blistering diseases (pemphigus vulgaris, bullous pemphigoid): DIF positive[3]
- Drug hypersensitivity syndrome/DRESS: eosinophilia, organ involvement, less epidermal detachment[10]
9. Past Medical History
- Prior SJS/TEN episodes (absolute contraindication to re-exposure to culprit drug)
- Autoimmune conditions (SLE, psoriasis)
- Malignancy (especially if on chemotherapy or immunotherapy)
- HIV/immunosuppression
- Chronic kidney disease (affects drug clearance and prognosis)
- Epilepsy and current anticonvulsant regimen
- Gout and allopurinol use
- Prior HLA testing results
10. Physical Exam
- Vital signs: Fever (often >38.5°C), tachycardia, hypotension in severe cases
Skin
- Dusky erythematous or violaceous macules, often starting on face/trunk[7]
- Atypical targetoid lesions (flat, irregular, dusky center — NOT classic EM targets)[2]
- Flaccid bullae, confluent epidermal detachment in sheets
- Nikolsky sign: positive on erythematous areas[7][10]
- Asboe-Hansen sign: lateral extension of blister with pressure
- Estimate %BSA detachment (TEN = ≥30%)[1][8]
Mucosal exam (involved in ~80% of cases)
- Oral: hemorrhagic erosions, pseudomembranes, crusted lips
- Ocular: conjunctival hyperemia, pseudomembranes, chemosis, corneal erosions[7][18]
- Genital/urethral: erosions, dysuria
- Nasal/pharyngeal: erosions
- Systemic: Lung auscultation (crackles suggest bronchial involvement), abdominal exam
11. Lab Studies
- CBC: lymphopenia is characteristic and predictive of SJS/TEN; neutrophilia may indicate secondary infection[10]
- BMP/CMP: BUN/creatinine (renal function — SCORTEN parameter), glucose >252 mg/dL (SCORTEN), bicarbonate <20 mmol/L (SCORTEN/ABCD-10)[25-26]
- LFTs: transaminases often elevated (hepatic involvement)
- Coagulation studies: PT/INR, fibrinogen, D-dimer (DIC screening)[11]
- Blood cultures: if sepsis suspected
- Lactate: sepsis workup
- Serum albumin: marker of severity and nutritional status
- Procalcitonin: may help distinguish infection from sterile inflammation
- Mycoplasma pneumoniae serology/PCR: especially in children or cases without drug trigger[8]
12. Imaging
- Chest X-ray: baseline and if respiratory symptoms present — evaluate for pneumonia, ARDS, bronchial epithelial sloughing[27]
- CT chest if concern for pulmonary complications not seen on CXR
- Imaging is NOT diagnostic for TEN — diagnosis is clinical[4]
- Imaging is primarily used to identify complications (pneumonia, effusions)
13. Special Tests
Diagnostic
- Skin biopsy: full-thickness epidermal necrosis with subepidermal cleavage; sparse dermal inflammatory infiltrate[3][7]
- Direct immunofluorescence (DIF): negative — essential to rule out autoimmune blistering diseases[7]
- Frozen section biopsy: can provide rapid confirmation in the ED/ICU setting
Scoring systems
- SCORTEN (Score of Toxic Epidermal Necrolysis): 7 parameters assessed within 24 hours of admission — predicts in-hospital mortality[8][25][28]
- Age >40, malignancy, HR >120, initial BSA detachment >10%, BUN >28 mg/dL, glucose >252 mg/dL, bicarbonate <20 mmol/L
- Score 0–1: 3.2% mortality; Score ≥5: 90% mortality[1][14]
- ABCD-10: alternative scoring (age, bicarbonate, cancer, dialysis, 10% BSA)[25-26]
- ALDEN score: algorithm to identify the most likely culprit drug when multiple drugs are involved[2]
Pharmacogenomic testing (pre-prescription screening)
- HLA-B15:02 before carbamazepine in patients of Southeast Asian descent (FDA-recommended)[20]
- HLA-B58:01 before allopurinol (ACR-recommended in high-risk populations)[21]
14. ECG
- ECG is indicated to evaluate for tachycardia (SCORTEN parameter: HR >120 bpm) and to screen for cardiac complications[22]
- Myocardial involvement is uncommon acutely but case reports describe myocardial infarction during acute TEN[11]
- SJS/TEN survivors have elevated long-term cardiovascular morbidity and mortality persisting 4–7 years post-event, attributed to sustained proinflammatory and hypermetabolic states[11]
- Monitor for DIC-related cardiac complications[11]
15. Assessment
- TEN is classified by ≥30% BSA epidermal detachment (SJS <10%, overlap 10–30%).[1][8] It is a delayed-type (Type IV) hypersensitivity reaction mediated by drug-specific cytotoxic T cells and NK cells, with granulysin as the key effector molecule causing keratinocyte apoptosis.[1][25]
- Severity stratification: SCORTEN should be calculated within 24 hours and repeated at day 3.[25][28] Mortality ranges from 3.2% (SCORTEN 0–1) to 90% (SCORTEN ≥5).[1] Recent data suggest SCORTEN may overestimate mortality in contemporary cohorts due to improvements in supportive care.[25][28]
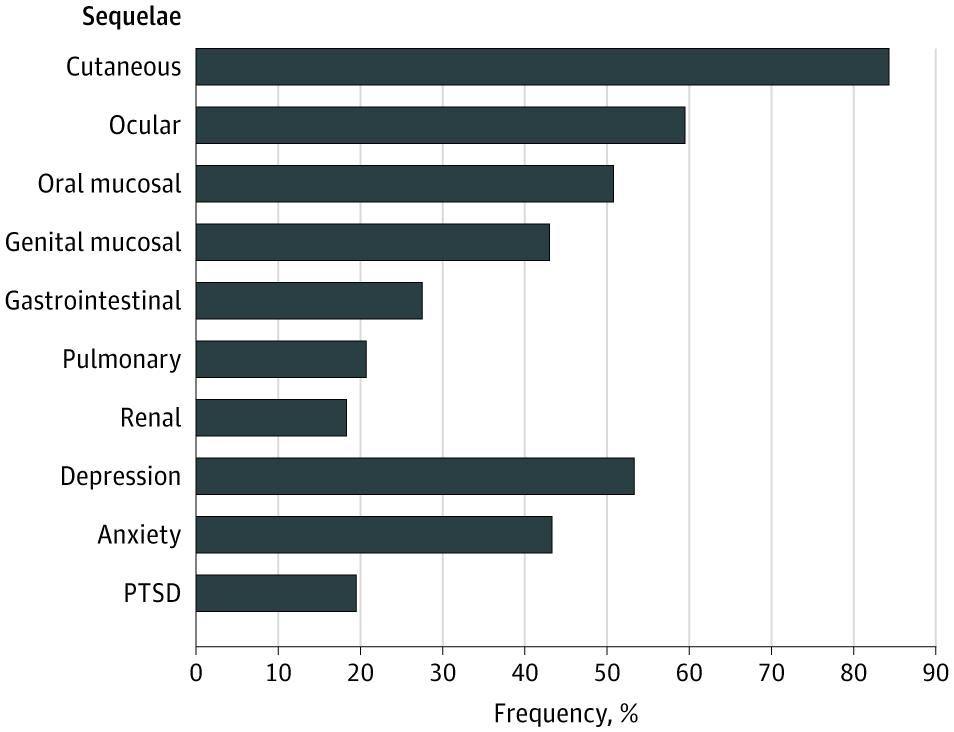
- Complications to anticipate: sepsis (leading cause of death), ARDS, acute renal failure, DIC, GI hemorrhage, electrolyte derangements, and multiorgan failure.[1][7] Long-term sequelae affect >80% of survivors — cutaneous (82%), ocular (59%), oral (48%), and psychological (depression 49%, anxiety 47%, PTSD 37%).[19]
- The following figure shows the frequency of long-term sequelae in SJS/TEN survivors:
16. Treatment Plan
Immediate stabilization (ED)
- Discontinue ALL suspected culprit drugs immediately — this is the single most impactful intervention[1][4][8]
- Airway assessment — early intubation if oropharyngeal/laryngeal involvement or respiratory distress[4]
- IV fluid resuscitation (crystalloid, burn-like protocols at ~2/3 Parkland formula)[5]
- Pain management (IV opioids often required; avoid NSAIDs if suspected culprit)
- Temperature regulation (warm environment, 28–32°C)[5]
Wound care
- Nonadherent dressings; avoid debridement of intact blisters[5]
- Gentle handling — minimize shear forces
- Topical antiseptics; silver-based dressings may be used[17]
Mucosal care
- Eyes: urgent ophthalmology consult; preservative-free lubricants, topical corticosteroid drops (0.1% betamethasone within 4 days of onset reduces sequelae), consider amniotic membrane transplantation[18][29]
- Oral: mouthwashes, topical anesthetics, soft diet
- GU: Foley catheter if urethral involvement; gynecology/urology consult[13]
- Systemic immunomodulatory therapy (no consensus; institution-dependent):[14-15]
- Cyclosporine 3–5 mg/kg/day for 7–14 days — meta-analysis suggests mortality benefit vs. IVIG (RR 0.18) Journal Der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology[15]
- Systemic corticosteroids: methylprednisolone 1–2 mg/kg/day — controversial but widely used[7][13]
- IVIG 2 g/kg over 2–5 days — evidence mixed; may be beneficial combined with corticosteroids Journal Der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology[15-16]
- Etanercept 25–50 mg SC single dose — emerging evidence of benefit (RR 0.32 vs. supportive care)[7][15][17]
- Thalidomide is contraindicated (increased mortality)[14]
- Supportive measures: DVT prophylaxis, stress ulcer prophylaxis, nutritional support, infection surveillance[5]
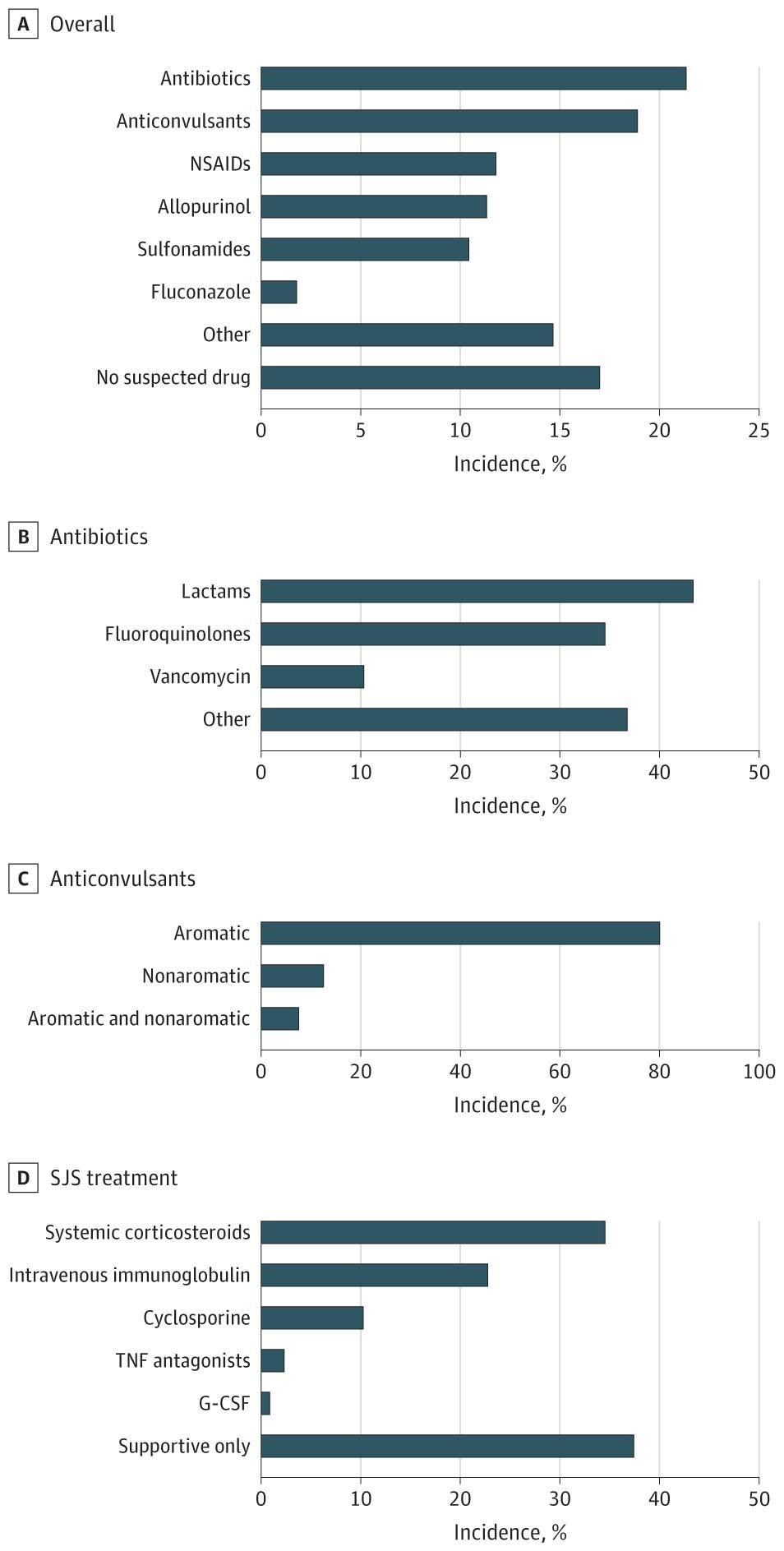
- The following figure shows the distribution of culprit drugs and treatment approaches across European centers:
- View full figure Figure 1. Distribution of General Culprit Drugs, Culprit Antibiotics, Culprit Anticonvulsants, and Treatment Modalities Assessment of Treatment Approaches and Outcomes in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Insights From a Pan-European Multicenter Study. JAMA Dermatol. September 30, 2021.
17. Disposition
- All patients with suspected TEN require admission — ideally to a burn unit or ICU with multidisciplinary access (burn surgery, dermatology, ophthalmology, critical care)[4-5]
- Transfer to a burn center if not available at presenting facility[4]
- SCORTEN ≥3 or BSA >10% detachment warrants ICU-level care[25]
- No patient with TEN should be discharged from the ED
Specialist consultations (all urgent)
- Dermatology
- Ophthalmology
- Burn surgery
- Critical care/ICU
- Urology/gynecology (if GU involvement)
- Pulmonology (if respiratory involvement)
18. Follow Up / Return Precautions
Post-discharge follow-up (multidisciplinary, prolonged)
- Dermatology: 2–4 weeks, then every 3–6 months for 1–2 years — monitor for cutaneous sequelae (dyspigmentation, scarring, nail dystrophy)
- Ophthalmology: within 1–2 weeks post-discharge and regularly for years — up to 65% develop chronic ocular complications (dry eye, symblepharon, corneal scarring, visual impairment)[7][18][31]
- Psychiatry/psychology: screen for PTSD, depression, anxiety — affects ~50% of survivors[19]
- Allergy/immunology: formal drug causality assessment (ALDEN score), documentation of culprit drug, MedicAlert bracelet[2]
Return precautions
- Fever, new rash, worsening skin pain, eye redness/vision changes, difficulty breathing, signs of infection at wound sites
- Expected re-epithelialization: begins ~1 week after disease onset, completes in 2–3 weeks[7]
Lifelong precautions
- Absolute avoidance of the culprit drug and structurally related compounds
- Pharmacogenomic testing and documentation in medical records
- Patient education regarding OTC medications (especially NSAIDs, cold medications)[32]
- Awareness of increased long-term cardiovascular risk[11]
References
1. Current Perspectives on Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. — Lerch M, Mainetti C, Terziroli Beretta-Piccoli B, Harr T. Clinical Reviews in Allergy & Immunology. 2018.
2. Worldwide Prevalence of Antibiotic-Associated Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Systematic Review and Meta-analysis. — Lee EY, Knox C, Phillips EJ. JAMA Dermatology. 2023.
3. Toxic Epidermal Necrolysis and Stevens-Johnson Syndrome. — Harr T, French LE. Orphanet Journal of Rare Diseases. 2010.
4. High Risk and Low Prevalence Diseases: Stevens Johnson Syndrome and Toxic Epidermal Necrolysis. — van Nispen C, Long B, Koyfman A. The American Journal of Emergency Medicine. 2024.
5. Multidisciplinary Treatment in Toxic Epidermal Necrolysis. — Surowiecka A, Barańska-Rybak W, Strużyna J. International Journal of Environmental Research and Public Health. 2023.
6. Correlations Between Clinical Patterns and Causes of Erythema Multiforme Majus, Stevens-Johnson Syndrome, and Toxic Epidermal Necrolysis: Results of an International Prospective Study. — Auquier-Dunant A, Mockenhaupt M, Naldi L, et al. Archives of Dermatology. 2002.
7. Severe Cutaneous Adverse Reactions to Drugs. — Duong TA, Valeyrie-Allanore L, Wolkenstein P, Chosidow O. Lancet. 2017.
8. Assessment of Treatment Approaches and Outcomes in Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Insights From a Pan-European Multicenter Study. — Kridin K, Brüggen MC, Chua SL, et al. JAMA Dermatology. 2021.
9. Infantile Stevens Johnson syndrome and toxic epidermal necrolysis: A systematic review of clinical features and outcomes in children ages 12 months and under. — Iriarte C, Karim SA, Nassim JS, Grenier PO, Massey KJ. Pediatric Dermatology. 2022.
10. Distinguishing Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis From Clinical Mimickers During Inpatient Dermatologic Consultation-a Retrospective Chart Review. — Weinkle A, Pettit C, Jani A, et al. Journal of the American Academy of Dermatology. 2019.
11. Risk of Cardiovascular Morbidity and Mortality in Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis Survivors. — Chiu HY, Chiu YM. JAMA Dermatology. 2025.
12. Culprit Medications and Risk Factors Associated With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Population-Based Nested Case-Control Study. — Gronich N, Maman D, Stein N, Saliba W. American Journal of Clinical Dermatology. 2022.
13. Management of Immune Checkpoint Inhibitor-Related Toxicities. — Updated 2025-10-23. National Comprehensive Cancer Network.
14. Systemic Interventions for Treatment of Stevens-Johnson Syndrome (SJS), Toxic Epidermal Necrolysis (TEN), and SJS/TEN Overlap Syndrome. — Jacobsen A, Olabi B, Langley A, et al. The Cochrane Database of Systematic Reviews. 2022.
15. Systemic Immunomodulating Therapies for Epidermal Necrolysis (Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis): A Systematic Review and Meta-Analysis. — Heuer R, Paulmann M, Mockenhaupt M, Nast A. Journal Der Deutschen Dermatologischen Gesellschaft = Journal of the German Society of Dermatology : JDDG. 2025.
16. Evaluation of Plasmapheresis vs Immunoglobulin as First Treatment After Ineffective Systemic Corticosteroid Therapy for Patients With Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis. — Miyamoto Y, Ohbe H, Kumazawa R, et al. JAMA Dermatology. 2023.
17. Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Review of Current Management and Innovative Therapies. — Martinez Villarreal JD, Cardenas-de la Garza JA, Ionescu MA, et al. International Journal of Dermatology. 2025.
18. Updates on the Ocular Manifestations and Treatment of SJS/TEN. — Sotozono C, Ueta M. Allergology International : Official Journal of the Japanese Society of Allergology. 2025.
19. Long-term Physical and Psychological Outcomes of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis. — Hoffman M, Chansky PB, Bashyam AR, et al. JAMA Dermatology. 2021.
20. Clinical Pharmacogenomic Testing and Reporting: A Technical Standard of the American College of Medical Genetics and Genomics (ACMG). — Tayeh MK, Gaedigk A, Goetz MP, et al. Genetics in Medicine : Official Journal of the American College of Medical Genetics. 2022.
21. HLA-B*58:01 and Risk of Allopurinol-Induced Severe Cutaneous Adverse Reactions in the US. — Campbell CN, Krantz MS, Yu A, Phillips EJ, Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis (SJS/TEN) Survivor Study Collaborators. JAMA Dermatology. 2025.
22. Predictive Value of a Severity-of-Illness Score for Toxic Epidermal Necrolysis (SCORTEN) Factors for in-Hospital Mortality in Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis. — Nikitina E, Dushkin A, Streltsov Y, et al. Frontiers in Medicine. 2025.
23. Immunohistopathological Findings of Severe Cutaneous Adverse Drug Reactions. — Orime M. Journal of Immunology Research. 2017.
24. Severe Adverse Cutaneous Reactions to Drugs. — Roujeau JC, Stern RS. The New England Journal of Medicine. 1994.
25. Improvement of Mortality Prognostication in Patients With Epidermal Necrolysis: The Role of Novel Inflammatory Markers and Proposed Revision of SCORTEN (Re-SCORTEN). — Koh HK, Fook-Chong SMC, Lee HY. JAMA Dermatology. 2022.
26. Assessment and Comparison of Performance of ABCD-10 and SCORTEN in Prognostication of Epidermal Necrolysis. — Koh HK, Fook-Chong S, Lee HY. JAMA Dermatology. 2020.
27. Drug-Induced Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Ten-Year Retrospective Study of 103 Cases. — Zhou L, Lu Y, Zou Y, et al. Clinical and Experimental Dermatology. 2025.
28. Accuracy of SCORTEN to Predict the Prognosis of Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: A Systematic Review and Meta-Analysis. — Torres-Navarro I, Briz-Redón Á, Botella-Estrada R. Journal of the European Academy of Dermatology and Venereology : JEADV. 2020.
29. Ocular Sequelae of Epidermal Necrolysis: French National Audit of Practices, Literature Review and Proposed Management. — Thorel D, Ingen-Housz-Oro S, Benaïm D, et al. Orphanet Journal of Rare Diseases. 2023.
30. Diagnosing and Managing Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis in Adults: Review of Evidence 2017-2023. — Ingen-Housz-Oro S, Matei I, Gaillet A, et al. The Journal of Investigative Dermatology. 2025.
31. Chronic Ocular Complications in Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis: Clinical Features and Surgical Management in a Brazilian Tertiary Center. — de Alcântara RJA, Wakamatsu TH, Hirai FE, et al. Cornea. 2025.
32. Severe Ocular Complications of SJS/TEN and Associations Among Pre-Onset, Acute, and Chronic Factors: A Report From the International Ophthalmology Collaborative Group. — Ueta M, Inoue C, Nakata M, et al. Frontiers in Medicine. 2023.