Tracheal Stenosis
Tracheal stenosis is a pathological narrowing of the tracheal lumen caused by neoplastic or nonneoplastic processes, most commonly iatrogenic (post-intubation/post-tracheostomy), but also arising f…
Tracheal stenosis is a pathological narrowing of the tracheal lumen caused by neoplastic or nonneoplastic processes, most commonly iatrogenic (post-intubation/post-tracheostomy), but also arising from autoimmune, inflammatory, infectious, or idiopathic etiologies.[1-2] It is frequently misdiagnosed as asthma or COPD due to overlapping symptoms, with a median diagnostic delay of 12 months in inflammatory cases.[3]
1. History
- Onset and progression: Insidious vs. acute; post-intubation stenosis typically presents 4–6 weeks after extubation with delayed dyspnea[4]
- Symptom characterization: Exertional dyspnea (most common), inspiratory stridor, biphasic stridor, wheezing, chronic cough, hoarseness, exercise intolerance[1][5]
- Timing/triggers: Symptoms worsen with exertion, URI, or cold air; may be positional
- Severity: Quantify dyspnea (at rest vs. exertion), ability to perform ADLs, sleep-disordered breathing[6]
- Prior airway instrumentation: Duration of intubation, tracheostomy history, number of intubation attempts, cuff pressures used[7]
- Important negatives: Lack of response to bronchodilators or inhaled corticosteroids (distinguishes from asthma); absence of diffuse wheezing on auscultation[8]
2. Alarm Features
- Stridor at rest — indicates >50% luminal narrowing; critical stenosis typically at >70% obstruction[9-10]
- Acute respiratory distress, cyanosis, inability to lie flat
- Inability to pass suction catheter through tracheostomy[11]
- Rapid progression of dyspnea over hours to days
- Hemoptysis — raises concern for malignant etiology or erosion[5]
- Failed response to bronchodilators/steroids in a patient labeled as asthma — should prompt airway evaluation[8]
3. Medications
- Contributing medications: No specific medications directly cause tracheal stenosis, but prolonged corticosteroid use may impair wound healing; diabetes medications should be optimized as diabetes is a risk factor for stenosis[7]
Treatments
- Intralesional triamcinolone acetonide injection at time of dilation reduces recurrence (37% vs. 54.5% without)[12]
- Topical mitomycin C application — 75% success rate at 4 months vs. 15% for dilation alone[13]
- Post-procedural inhaled budesonide as recurrence prophylaxis[12]
- PPIs (e.g., omeprazole 80 mg/day) for GERD-associated stenosis[4][14]
- Systemic immunosuppression (glucocorticoids ± methotrexate) for GPA- or RP-related stenosis[3]
- Contraindicated: Avoid heat-based ablative therapies with FiO₂ >0.4 (airway fire risk)[13]
4. Diet
- GERD management: GERD is a recognized risk factor and potential contributor to tracheal stenosis recurrence. Anti-reflux dietary modifications (avoid late meals, acidic/spicy foods, caffeine, alcohol) are recommended as adjunctive therapy[1][4]
- Hydration: Adequate hydration to maintain airway secretion clearance, especially in stented patients
- Weight management: Obesity is associated with iatrogenic tracheal stenosis and may complicate airway management[4][7]
5. Review of Systems
- Pulmonary: Dyspnea, stridor, wheezing, cough, hemoptysis, exercise intolerance
- ENT: Hoarseness, voice changes, dysphagia, globus sensation, nasal crusting/epistaxis (GPA)
- GI: Heartburn, regurgitation, chronic throat clearing (GERD/LPR)
- Rheumatologic: Joint pain, skin rashes, ear/nose cartilage pain (relapsing polychondritis), sinusitis, renal symptoms (GPA)[3]
- Constitutional: Fevers, weight loss, night sweats (malignancy, vasculitis, TB)
6. Collateral History and Family History
- Collateral: ICU records — duration of intubation, cuff pressures, number of reintubations, tracheostomy details, ventilator settings[7]
- Family history: Generally not hereditary; however, congenital tracheal stenosis exists in pediatric populations[15]
- Social context: Occupational exposures (chemical/thermal inhalation), smoking history (predictor of need for resection), illicit drug use (inhalational injuries)[16]
7. Risk Factors
- Iatrogenic (most common, >80% of acquired cases): Prolonged intubation, tracheostomy, prior airway surgery[7][17]
- Duration of intubation and mechanical ventilation[7]
- Diabetes mellitus — independent risk factor for stenosis development and decannulation failure[4][7]
- Respiratory tract infection during intubation[7]
- High tracheostomy incision[7]
- Cuff-to-trachea diameter ratio (C/T) >150%[7]
- GERD/laryngopharyngeal reflux[1][4]
- Autoimmune diseases: GPA (41%), relapsing polychondritis (26%) among inflammatory causes[3]
- Idiopathic subglottic stenosis: Almost exclusively middle-aged white females[4][18]
- Obesity, vascular disease[4]
- Radiation therapy, infections (TB), sarcoidosis, amyloidosis[1][19]
8. Differential Diagnosis
- Asthma/reactive airway disease — most common misdiagnosis; distinguished by lack of bronchodilator response and fixed obstruction on PFTs[8][20]
- COPD — diffuse lower airway obstruction; coexisting COPD may mask tracheal stenosis on PFTs[5]
- Vocal cord dysfunction (VCD)/paradoxical vocal fold motion — episodic, inspiratory stridor, normal between episodes
- Tracheal/endobronchial malignancy — adenoid cystic carcinoma, squamous cell carcinoma, carcinoid[5][21]
- Tracheobronchomalacia — dynamic collapse rather than fixed stenosis; diagnosed on dynamic expiratory CT[13]
- Extrinsic compression — thyroid goiter, mediastinal mass, vascular ring
- Foreign body aspiration
- Angioedema — acute onset, associated urticaria
- Epiglottitis/croup — infectious, acute presentation
9. Past Medical History
- Prior intubation/tracheostomy (duration, number of episodes)
- Previous airway dilations or surgeries (number and type — critical for treatment planning)[16][22]
- Autoimmune conditions (GPA, relapsing polychondritis, sarcoidosis, Crohn's disease)[3]
- GERD history[4]
- Diabetes mellitus[7]
- Prior radiation therapy to head/neck/chest
- History of inhalational injury or external neck trauma
- Smoking history[16]
10. Physical Exam
- Vital signs: Tachypnea, hypoxia (late finding), use of accessory muscles
- Inspection: Stridor (inspiratory = extrathoracic; biphasic = fixed; expiratory = intrathoracic), tracheal tug, suprasternal/intercostal retractions[15]
- Auscultation: Monophonic wheeze or stridor loudest over the neck/central airways (vs. diffuse polyphonic wheezing in asthma); diminished air entry in severe stenosis
- Neck exam: Tracheostomy site/scar, tracheal deviation, thyroid enlargement, cervical lymphadenopathy
- ENT findings: Saddle nose deformity, nasal crusting (GPA); auricular chondritis, ear/nose tenderness (relapsing polychondritis)[3]
- Concerning findings: Stridor at rest, cyanosis, inability to speak in full sentences, tripod positioning
11. Lab Studies
- Baseline: CBC, BMP, coagulation studies (preoperative)
Autoimmune workup (when inflammatory etiology suspected)
- ANCA (c-ANCA/PR3 for GPA)[3][23]
- ESR, CRP
- ANA, anti-dsDNA (if lupus suspected)
- Infectious: AFB cultures, fungal cultures (if TB or fungal etiology suspected)
- GERD evaluation: Consider 24-hour pH monitoring or impedance testing[4][14]
- Biopsy at bronchoscopy: Histopathology to distinguish granulomatous, fibrotic, or malignant processes[1][24]
12. Imaging
- First-line: CT chest (with or without IV contrast) — the ACR Appropriateness Criteria rates CT as the initial imaging modality of choice for suspected tracheal stenosis. CT with IV contrast is preferred when malignancy or mediastinal pathology is suspected[21]
- Multiplanar reconstructions (MPR) and virtual bronchoscopy are helpful adjuncts for preprocedural planning[21]
- 3D volume rendering accurately predicts stenosis location, length, and severity[21]
- Dynamic expiratory CT: Useful to evaluate for concurrent tracheomalacia[21]
- Chest X-ray: May show tracheal narrowing; the "inverted steeple sign" has been described for lower tracheal stenosis; generally insufficient for definitive diagnosis[15]
- MRI: Limited role; a meta-analysis found critically low specificity (6–46%) for grading stenosis. May be useful for GPA-related SGS monitoring without radiation[25-26]
- Imaging unnecessary: Stable, known mild stenosis under surveillance with PFTs and clinical assessment
13. Special Tests
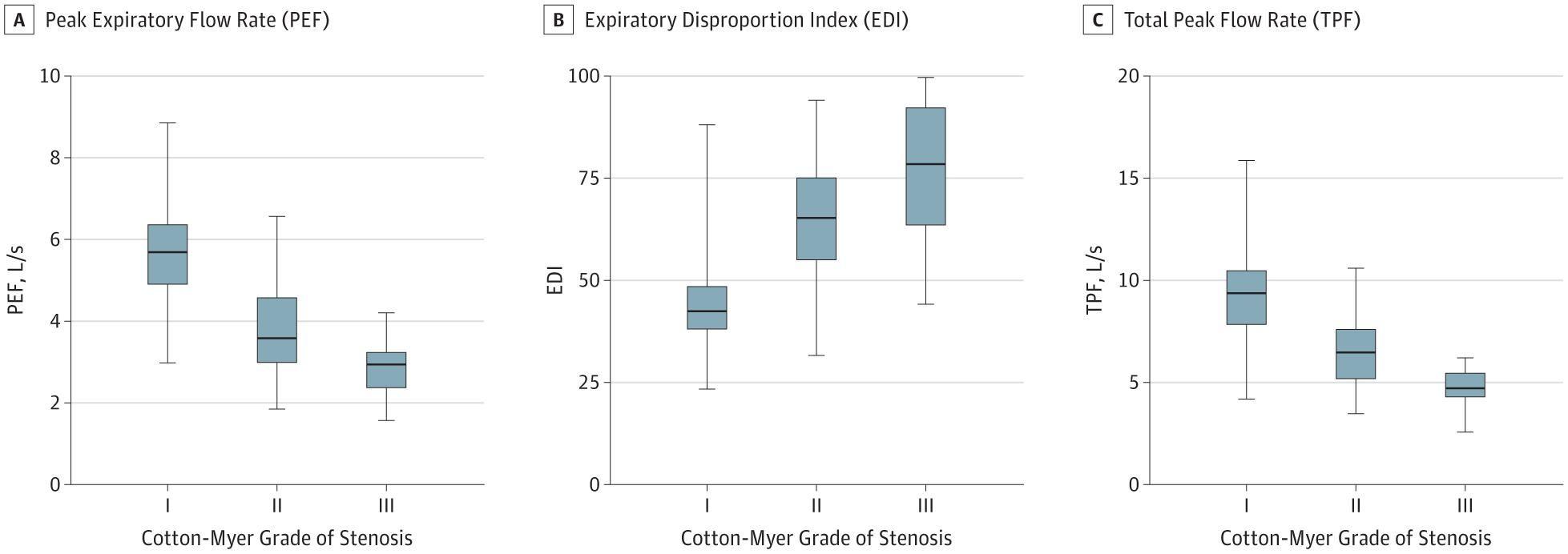
Myer-Cotton grading system
- Grade I: ≤50% obstruction
- Grade II: 51–70% obstruction
- Grade III: 71–99% obstruction
- Grade IV: No detectable lumen
- Higher grades (and pre-operative tracheostomy) are independent predictors of need for surgical resection[16]
Pulmonary function tests / Flow-volume loops
- Fixed obstruction: Plateau on both inspiratory and expiratory limbs (rectangular loop)
- Variable extrathoracic: Plateau on inspiratory limb with preserved expiratory flow
- Variable intrathoracic: Plateau on expiratory limb with preserved inspiratory flow
- FEV₁/PEF ratio >8 mL·L⁻¹·min⁻¹ suggests central/upper airway obstruction[28]
- Expiratory Disproportion Index (EDI): Highest sensitivity (88%) for predicting need for intervention[30]
- PEF, PIF, and EDI all significantly improve after stenosis is relieved[30]
- Bronchoscopy: Diagnostic gold standard — allows direct visualization, grading, biopsy, and simultaneous therapeutic intervention[1][5][24]
14. ECG
- ECG is not a primary diagnostic tool for tracheal stenosis
- Obtain ECG as part of preoperative assessment before bronchoscopy or surgical intervention
- Chronic hypoxia from severe stenosis may show signs of right heart strain (right axis deviation, P pulmonale, RV hypertrophy) in advanced cases
- Rule out cardiac causes of dyspnea in the differential
15. Assessment
- Clinical summary: Tracheal stenosis presents insidiously with progressive dyspnea, stridor, and exercise intolerance. Symptoms typically do not manifest until >50% luminal narrowing, and work of breathing increases rapidly beyond 70% obstruction[9-10]
- Severity stratification: Based on Myer-Cotton grade, PFT findings, and symptom burden[18][27]
- Typical presentation: Post-intubation — delayed onset 4–6 weeks after extubation; idiopathic SGS — middle-aged white female with progressive dyspnea misdiagnosed as asthma[4][18]
- Atypical presentations: Inflammatory stenosis may present as the first manifestation of systemic disease in 66% of cases[3]
- Complications: Respiratory failure, recurrent pneumonia, mucus plugging (especially with stents), airway fire during procedures, restenosis (76% relapse rate in inflammatory causes)[3][31]
16. Treatment Plan
Initial stabilization (ED)
- Secure airway — heliox (70:30 or 80:20) as temporizing measure to reduce work of breathing
- Humidified oxygen, upright positioning
- Racemic epinephrine nebulization for acute mucosal edema
- Dexamethasone IV for edema reduction
- If critical obstruction: emergent rigid bronchoscopy for debulking/dilation; if unavailable, endotracheal intubation with a smaller tube past the stenosis or emergent tracheostomy/cricothyrotomy[5][11]
Definitive management
- The ACCP 2025 guidelines recommend a comprehensive evaluation including CT chest and appropriate labs, followed by either therapeutic bronchoscopy or surgical resection for symptomatic stenosis:[13]
- Surgical resection with primary anastomosis: Preferred definitive treatment for focal benign stenosis in operable patients. Three-year recurrence rate of only 1.2% vs. 28% for dilation and 12.4% for endoscopic resection with medical therapy. Resection-anastomosis showed adjusted HR 2.0 for clinical resolution compared to stenting[13][32]
- Endoscopic interventions (for non-surgical candidates or as bridge to surgery):
- Balloon or rigid dilation ± adjunctive therapies[13]
- Laser (CO₂, Nd:YAG) or electrocautery ablation of scar tissue[13]
- Intralesional triamcinolone injection[12]
- Topical mitomycin C application[13]
- Airway stent placement — reserved for failed bronchoscopic/systemic treatments[13]
- Rigid bronchoscopy preferred over flexible for therapeutic interventions, under general anesthesia[13]
- Systemic therapy: Glucocorticoids + methotrexate for GPA/RP-related stenosis; anti-GERD therapy for reflux-associated stenosis[3][14]
17. Disposition
- Admission criteria: Stridor at rest, respiratory distress, hypoxia, need for emergent airway intervention, new diagnosis with significant obstruction (Myer-Cotton grade III–IV)
- ICU admission: Impending respiratory failure, post-emergent airway intervention, hemodynamic instability
- Observation: Post-dilation monitoring (typically 4–6 hours minimum), new stent placement
- Discharge criteria: Stable airway, no stridor at rest, adequate oxygenation, able to tolerate oral intake, reliable follow-up arranged
- Specialist consultation triggers: Interventional pulmonology, thoracic surgery, and otolaryngology — a multidisciplinary team approach is essential. Rheumatology for suspected autoimmune etiology[1][3][13]
18. Follow Up / Return Precautions
- Follow-up timing: Post-dilation — 4–6 weeks for reassessment; PFTs at regular intervals for surveillance (PEF is a simple, reliable monitoring parameter)[18][30]
- Symptoms requiring immediate reassessment: Worsening dyspnea, new or worsening stridor, inability to clear secretions, fever (if stented — concern for granulation tissue/infection), hemoptysis
Patient counseling
- Recurrence is common — 76% relapse rate in inflammatory causes; >85% of idiopathic SGS patients require repeat intervention within 5 years[3][18]
- Compliance with anti-reflux therapy if GERD is identified[14]
- Smoking cessation (smoking history predicts need for resection)[16]
- Diabetes optimization[7]
- Expected recovery: Post-dilation — immediate symptom improvement but high recurrence risk; post-surgical resection — excellent long-term outcomes with low recurrence in appropriately selected patients[13][32]
References
1. The Role of Bronchoscopy in the Multidisciplinary Approach to Benign Tracheal Stenosis. — Ravikumar N, Ho E, Wagh A, Murgu S. Journal of Thoracic Disease. 2023.
2. Tracheobronchial Stenosis: Causes and Advances in Management. — Puchalski J, Musani AI. Clinics in Chest Medicine. 2013.
3. Presentation, Diagnosis, and Management of Subglottic and Tracheal Stenosis During Systemic Inflammatory Diseases. — Catano J, Uzunhan Y, Paule R, et al. Chest. 2022.
4. Laryngotracheal stenosis: Mechanistic review. — Carpenter DJ, Hamdi OA, Finberg AM, Daniero JJ. Head & Neck. 2022.
5. Interventional Pulmonology. — Seijo LM, Sterman DH. The New England Journal of Medicine. 2001.
6. Acquired Tracheal Stenosis: Cervical Slide Tracheoplasty. — Li C, Rutter MJ. Seminars in Pediatric Surgery. 2021.
7. Risk Factors for Patients With Tracheal Stenosis: A Systematic Review and Meta-Analysis. — Hong S, Wu X, Feng H, et al. The Journal of International Medical Research. 2024.
8. Management of Postintubation Tracheal Stenosis in a Neurosurgical Patient With Tracheomalacia and Scarring Tendency: A Case Report. — Zhan Y, Zhang S, Chen M, Pu H. Medicine. 2026.
9. Subglottic Stenosis Position Affects Work of Breathing. — Yang MM, Higano NS, Gunatilaka CC, et al. The Laryngoscope. 2021.
10. Relationship Between Degree of Obstruction and Airflow Limitation in Subglottic Stenosis. — Lin EL, Bock JM, Zdanski CJ, Kimbell JS, Garcia GJM. The Laryngoscope. 2018.
11. Successful Rescue Using Tracheal Intubation Cannula for Severe Central Airway Stenosis After Tracheotomy: A CARE Compliant Case Report. — Li HF, Xing BP, Song LS, Wang W, Liu BH. Medicine. 2020.
12. Endoscopic Treatment of Benign Tracheal Stenosis: A Single-Centre Study. — Kather D, Steinack C, Franzen DP. Swiss Medical Weekly. 2024.
13. Management of Central Airway Obstruction: An American College of Chest Physicians Clinical Practice Guideline. — Mahmood K, Frazer-Green L, Gonzalez AV, et al. Chest. 2025.
14. Idiopathic Tracheal Stenosis: Successful Outcome With Antigastroesophageal Reflux Disease Therapy. — Terra RM, de Medeiros IL, Minamoto H, et al. The Annals of Thoracic Surgery. 2008.
15. The Inverted Steeple Sign, Tracheal Tug, and Biphasic Stridor: A Triad for Diagnosing Congenital Tracheal Stenosis. — Rajvanshi N, Ks A, Kumar TVV. Pediatric Pulmonology. 2025.
16. Management of Benign Airway Stenosis-Predictors of Tracheal Resection. — Patel AJ, Budacan AM, Kumar S, et al. Journal of Thoracic Disease. 2024.
17. Staged Laryngotracheoplasty in Adult Laryngotracheal Stenosis: Predictors of Long-term Decannulation. — Liu IY, Mendelsohn AH, Ching H, et al. JAMA Otolaryngology-- Head & Neck Surgery. 2015.
18. Utility of Routine Spirometry Measures for Surveillance of Idiopathic Subglottic Stenosis. — Carpenter DJ, Ferrante S, Bakos SR, et al. JAMA Otolaryngology-- Head & Neck Surgery. 2019.
19. Nonneoplastic Tracheal and Bronchial Stenoses. — Grenier PA, Beigelman-Aubry C, Brillet PY. Radiologic Clinics of North America. 2009.
20. Flow Volume Loops in the Evaluation of Upper Airway Obstruction. — Lunn WW, Sheller JR. Otolaryngologic Clinics of North America. 1995.
21. ACR Appropriateness Criteria® Tracheobronchial Disease. — Expert Panel on Thoracic Imaging, Little BP, Walker CM, et al. Journal of the American College of Radiology : JACR. 2024.
22. Predictors of Response to Endoscopic Management of Subglottic/Tracheal Stenosis in Patients Without Tracheostomy. — Ahmadian D, Gleadhill CM, Wehbi N, Bixby BA, Yip HT. American Journal of Otolaryngology. 2023.
23. Clinical Manifestations and Treatment of Idiopathic and Wegener Granulomatosis–Associated Subglottic Stenosis. — Taylor SC, Clayburgh DR, Rosenbaum JT, Schindler JS. JAMA Otolaryngology-- Head & Neck Surgery. 2013.
24. A Review on Diagnostic Assessments of Tracheal Stenosis. — Monjezi M, Rismanian M, Jamaati H. Biomedical Engineering Online. 2025.
25. Diagnostic Accuracy of Non-Invasive Modalities for Laryngotracheal Stenosis: A Systematic Review and Meta-Analysis. — Klopper GJ, Adeniyi OV. European Archives of Oto-Rhino-Laryngology : Official Journal of the European Federation of Oto-Rhino-Laryngological Societies : Affiliated With the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2026.
26. Accuracy of Magnetic Resonance Imaging for Grading of Subglottic Stenosis in Patients With Granulomatosis With Polyangiitis: Correlation With Pulmonary Function Tests and Laryngoscopy. — Henes FO, Laudien M, Linsenhoff L, et al. Arthritis Care & Research. 2018.
27. Endoscopic Management of Subglottic Stenosis. — Feinstein AJ, Goel A, Raghavan G, et al. JAMA Otolaryngology-- Head & Neck Surgery. 2017.
28. ERS/ATS Technical Standard on Interpretive Strategies for Routine Lung Function Tests. — Stanojevic S, Kaminsky DA, Miller MR, et al. The European Respiratory Journal. 2022.
29. Evaluation of Major Airway Lesions Using the Flow-Volume Loop. — Hyatt RE. The Annals of Otology, Rhinology, and Laryngology. 1975.
30. Spirometry in Laryngotracheal Stenosis: A Systematic Review and Meta-Analysis. — Alshareef W, Almutairi N, Sindi A, et al. European Archives of Oto-Rhino-Laryngology : Official Journal of the European Federation of Oto-Rhino-Laryngological Societies : Affiliated With the German Society for Oto-Rhino-Laryngology - Head and Neck Surgery. 2023.
31. Treatment of Benign Tracheal Stenosis Using Endoluminal Spray Cryotherapy. — Bhora FY, Ayub A, Forleiter CM, et al. JAMA Otolaryngology-- Head & Neck Surgery. 2016.
32. Stent and Resection Anastomosis in Patients With Complex Tracheal Stenosis: The Stars Retrospective Multicenter Trial. — Marchioni A, Moretti A, Tonelli R, et al. Interdisciplinary Cardiovascular and Thoracic Surgery. 2025.