Transfusion-Associated Circulatory Overload (TACO)
TACO is the leading cause of transfusion-related morbidity and mortality worldwide, characterized by hydrostatic (cardiogenic) pulmonary edema occurring during or within 6–12 hours of blood transfu…
TACO is the leading cause of transfusion-related morbidity and mortality worldwide, characterized by hydrostatic (cardiogenic) pulmonary edema occurring during or within 6–12 hours of blood transfusion.[1-2] It affects approximately 1–12% of at-risk transfused patients and is widely underrecognized.[2-3] Up to 50% of cases occur after transfusion of a single unit, suggesting factors beyond volume alone contribute to pathophysiology.[4]
1. History
- Temporal relationship: Onset of symptoms during or within 6–12 hours of transfusion completion[5]
- Acute dyspnea, orthopnea, cough (may be frothy/pink sputum)
- Ask about volume and rate of transfusion, number of units given
- Pre-transfusion respiratory baseline — was the patient already dyspneic?
- Prior episodes of TACO or known CHF exacerbations
- Fluid balance over the preceding 24 hours (IV fluids, oral intake, urine output)
- Important negatives: fever (typically absent in TACO, present in TRALI), rigors, urticaria, flank pain[6-7]
2. Alarm Features
- Acute respiratory distress with hypoxemia requiring supplemental O₂ or intubation
- Severe hypertension with widened pulse pressure[5]
- Rapid desaturation (SpO₂ < 90%) during or immediately after transfusion
- Signs of frank pulmonary edema (pink frothy sputum, diffuse crackles)
- Hemodynamic instability or need for vasopressors (consider overlap with TRALI or septic transfusion reaction)
- Mortality in TACO cases is approximately 21% vs 11% in matched controls[8]
3. Medications
Treatment
- IV loop diuretics (furosemide 20–40 mg IV) — both diagnostic and therapeutic; clinical improvement with diuresis supports TACO[3][5]
- Supplemental oxygen; NIV (BiPAP/CPAP) as needed
- Nitrates for afterload reduction if hypertensive
Prevention
- Pre-transfusion diuretics in high-risk patients (logical but not rigorously studied)[3][9]
- Slow transfusion rate: maximum 4 hours per unit[10]
- Medications that increase risk: Large-volume IV fluid resuscitation concurrent with transfusion
- Caution: Diuretics are contraindicated if TRALI is the primary diagnosis (noncardiogenic edema; diuretics may worsen hypotension)[1]
4. Diet
- Sodium restriction in patients with known CHF or renal failure receiving transfusions
- Strict fluid restriction in at-risk patients during transfusion periods
- Accurate I&O monitoring including oral intake
- Long-term: dietary sodium management for patients with recurrent TACO or underlying heart failure
5. Review of Systems
- Respiratory: Dyspnea, orthopnea, paroxysmal nocturnal dyspnea, cough, sputum production
- Cardiovascular: Chest pain/pressure, palpitations, lower extremity edema, weight gain
- Renal: Urine output (oliguria/anuria), recent dialysis schedule
- General: Fever (absent in TACO; if present, consider TRALI, septic reaction, or hemolytic reaction)[7]
- Neurologic: Altered mental status (may indicate severe hypoxemia)
6. Collateral History and Family History
- Prior transfusion reactions — history of TACO is a strong predictor of recurrence[9]
- Baseline cardiac function (recent echocardiogram, known EF)
- Dialysis schedule and dry weight for ESRD patients
- Nursing documentation of transfusion rate, volume infused, and concurrent IV fluids
- Family history is generally not contributory, though familial cardiomyopathy or renal disease may increase baseline risk
7. Risk Factors
- Multivariable analyses have identified the following independent predictors:[3][5][8]
- Age > 70 years
- Congestive heart failure or cardiac dysfunction (reduced EF)
- Renal failure — especially patients on dialysis or with acute kidney injury
- Positive fluid balance prior to transfusion
- Rapid transfusion rate or large volume of blood products
- Plasma transfusion (especially in females)[8]
- Deep/severe anemia (pre-transfusion Hb very low)
- Emergency surgery
- Pre-transfusion diuretic use (marker of at-risk patients, not causative)[8]
- Small body habitus / low body weight
8. Differential Diagnosis
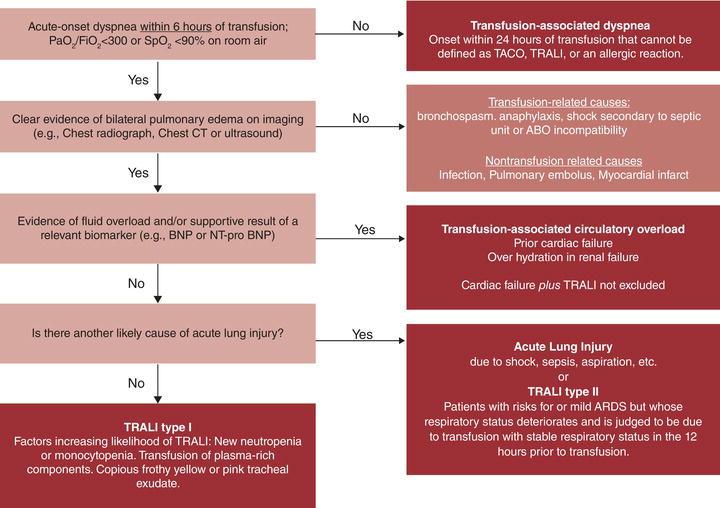
- The following diagnostic algorithm helps differentiate respiratory transfusion reactions:
- Transfusion-Related Acute Lung Injury (TRALI) — the most critical mimic. Noncardiogenic permeability edema; associated with fever, hypotension (vs. hypertension in TACO), normal BNP, bilateral infiltrates, no response to diuretics[1][12]
- Acute decompensated heart failure — may be indistinguishable; temporal relationship to transfusion is key
- Septic transfusion reaction — fever, rigors, hypotension, positive blood cultures
- Acute hemolytic transfusion reaction — fever, flank pain, dark urine, hemoglobinemia
- Anaphylactic transfusion reaction — urticaria, angioedema, bronchospasm, hypotension
- Aspiration pneumonitis — witnessed aspiration event, focal infiltrate
- Pulmonary embolism — pleuritic chest pain, unilateral leg swelling, risk factors for VTE
- TACO/TRALI overlap — increasingly recognized; both mechanisms may coexist[13-14]
- Export Feature TACO TRALI Ref Mechanism Hydrostatic (cardiogenic) edema Permeability (noncardiogenic) edema[1]
- Blood pressure Hypertension, widened pulse pressure Hypotension[2-3]
- Fever Absent Often present[4]
- BNP/NT-proBNP Elevated (ratio > 1.5) Normal or low[5]
- Fluid balance Positive Variable[6]
- Response to diuretics Yes (diagnostic + therapeutic) No (may worsen)[1, 6]
- Onset During or ≤12 h post-transfusion ≤6 h post-transfusion[1-2]
9. Past Medical History
- CHF (most important predisposing condition)
- Chronic kidney disease / ESRD / dialysis dependence
- Coronary artery disease, valvular heart disease
- Prior TACO episodes
- Chronic transfusion dependence (e.g., MDS, thalassemia, sickle cell disease)
- Recent surgery (especially emergency surgery)[8]
- Chronic lung disease (reduced pulmonary reserve)
10. Physical Exam
- Vitals: Hypertension, tachycardia, tachypnea, hypoxemia (SpO₂ < 94%), widened pulse pressure[5]
- Respiratory: Bilateral crackles/rales, decreased breath sounds at bases, use of accessory muscles, orthopnea
- Cardiovascular: S3 gallop, elevated JVP, peripheral edema
- General: Diaphoresis, cyanosis, respiratory distress
- Concerning findings: Severe hypoxemia requiring intubation, hemodynamic collapse (consider TRALI or septic reaction if hypotensive)
11. Lab Studies
BNP or NT-proBNP — the primary diagnostic biomarker
- Post/pre-transfusion NT-proBNP ratio > 1.5 supports TACO
- Post-transfusion BNP < 300 pg/mL or NT-proBNP < 2000 pg/mL makes TACO unlikely
- Specificity is poor in critically ill patients[15]
- ABG: Hypoxemia, may show respiratory alkalosis or mixed acid-base disorder
- CBC: Verify hemoglobin response to transfusion
- BMP/CMP: Assess renal function, electrolytes
- Troponin: If concern for ACS as precipitant
- Lactate: If hemodynamic compromise
- Blood cultures: If fever present (rule out septic transfusion reaction)
- DAT (Coombs test): If hemolytic reaction suspected
- Pulmonary edema fluid protein/serum protein ratio: < 0.65 supports hydrostatic edema (TACO); > 0.75 supports permeability edema (TRALI) — rarely performed but can be definitive[12]
12. Imaging
Chest X-ray (first-line)
- Bilateral pulmonary edema / vascular congestion
- Pleural effusions
- Enlarged cardiac silhouette (cardiomegaly)
- Kerley B lines
- Findings may be indistinguishable from TRALI on CXR alone[12]
Echocardiography
- Assess LV function, wall motion abnormalities, valvular disease
- Elevated filling pressures support TACO over TRALI
- Can be performed at bedside (point-of-care)
- Lung ultrasound: B-lines (pulmonary edema), pleural effusions — rapid bedside assessment
- CT chest: Generally unnecessary unless PE or other pathology suspected
13. Special Tests
- Pre- and post-transfusion BNP/NT-proBNP — the most useful biomarker strategy; obtain baseline before transfusion in high-risk patients[15]
- Echocardiography (TTE) — bedside assessment of cardiac function and filling pressures
- Pulmonary artery catheterization — rarely needed; PCWP > 18 mmHg supports TACO[12]
- Edema fluid sampling — protein ratio analysis if intubated (research/academic settings)
- TRALI workup (if suspected): Donor antibody screening, recipient HLA/HNA antibody testing[12]
14. ECG
- Obtain ECG to rule out acute coronary syndrome as precipitant
- May show: sinus tachycardia, LVH, atrial fibrillation (pre-existing), ST-T wave changes
- Dangerous patterns: ST elevation/depression suggesting ACS, new-onset atrial fibrillation with rapid ventricular response, wide-complex tachycardia
- ECG is not diagnostic for TACO but helps identify cardiac comorbidities contributing to volume intolerance
15. Assessment
- TACO is a clinical diagnosis based on the temporal relationship between transfusion and development of signs/symptoms of hydrostatic pulmonary edema. The NHSN definition requires new onset or exacerbation of ≥3 of the following within 6 hours of transfusion:[3]
- Respiratory distress
- Elevated BNP/NT-proBNP
- Increased CVP
- Left heart failure
- Positive fluid balance
- Pulmonary edema on imaging
Severity stratification: Ranges from mild (supplemental O₂ only, rapid diuretic response) to severe (requiring intubation/mechanical ventilation). TACO cases requiring mechanical ventilation occur in up to 71% of cases in ICU populations.[8] The pathophysiology follows a two-hit model: first hit = patient comorbidity rendering volume noncompliance; second hit = the transfusion itself, which contributes volume, colloid osmotic effects, pro-inflammatory mediators, and storage lesion byproducts.[4]
16. Treatment Plan
Immediate management
- Stop the transfusion immediately[3]
- Sit the patient upright
- Supplemental oxygen — nasal cannula, high-flow, or NIV (BiPAP/CPAP) as needed
- IV furosemide 20–40 mg (or equivalent loop diuretic) — both diagnostic and therapeutic[3][10]
- Continuous pulse oximetry and cardiac monitoring
- Strict I&O with Foley catheter if needed
If severe / refractory
- Intubation and mechanical ventilation if worsening hypoxemia despite NIV
- IV nitroglycerin for afterload reduction if hypertensive
- Consider ICU admission
Prevention strategies for future transfusions
- Identify at-risk patients before transfusion
- Transfuse one unit at a time (single-unit transfusion strategy)
- Slow infusion rate: 3–4 hours per unit (max 4 hours per component)
- Pre-transfusion diuretics (e.g., furosemide 20 mg IV) in high-risk patients
- Minimize concurrent IV fluids
- Use restrictive transfusion thresholds (Hb 7 g/dL in most patients)
- Reassess clinical need after each unit before ordering additional units
17. Disposition
Admit (or escalate to higher level of care) if
- Requiring supplemental O₂ beyond baseline
- Hemodynamic instability
- Need for mechanical ventilation (ICU)
- Ongoing hypoxemia despite diuresis
- Uncertain diagnosis (TACO vs. TRALI — management differs significantly)
- Observation appropriate for mild cases with rapid response to diuretics and O₂
- Discharge only after complete symptom resolution, return to baseline oxygenation, and stable hemodynamics
- Consult transfusion medicine/blood bank — mandatory for hemovigilance reporting and to guide future transfusion planning[16-17]
- Pulmonology or cardiology consultation if diagnostic uncertainty or severe presentation
18. Follow Up / Return Precautions
- Report to blood bank/transfusion medicine for hemovigilance documentation[16-17]
- Flag the patient's chart for TACO history — future transfusions require modified protocols (slow rate, pre-diuretics, single-unit strategy)[9]
- Follow-up echocardiography if new cardiac dysfunction identified
- Reassess transfusion indication — consider alternatives (e.g., EPO, iron therapy) to reduce transfusion burden
- Return precautions: Instruct patient/family to seek immediate care for recurrent dyspnea, chest tightness, cough, or swelling after any future transfusion
- Expected course: Most patients improve within hours of diuresis and cessation of transfusion; full resolution typically within 24–48 hours[10]
- If recurrent TACO, consider cardiology and nephrology co-management for optimization before future transfusions
References
1. Transfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung Injury. — Semple JW, Rebetz J, Kapur R. Blood. 2019.
2. Transfusion-Associated Circulatory Overload: A Clinical Perspective. — Bosboom JJ, Klanderman RB, Migdady Y, et al. Transfusion Medicine Reviews. 2019.
3. Transfusion Reactions: Prevention, Diagnosis, and Treatment. — Delaney M, Wendel S, Bercovitz RS, et al. Lancet. 2016.
4. The Recipe for TACO: A Narrative Review on the Pathophysiology and Potential Mitigation Strategies of Transfusion-Associated Circulatory Overload. — Bulle EB, Klanderman RB, Pendergrast J, et al. Blood Reviews. 2022.
5. Revised International Surveillance Case Definition of Transfusion-Associated Circulatory Overload: A Classification Agreement Validation Study. — Wiersum-Osselton JC, Whitaker B, Grey S, et al. The Lancet. Haematology. 2019.
6. Loop Diuretics for Patients Receiving Blood Transfusions. — Sarai M, Tejani AM. The Cochrane Database of Systematic Reviews. 2015.
7. Evaluation of pulmonary abnormalities in recipients of hematopoietic cell transplants and cellular therapies. — Thomas L, Boatman J. Transplant Infectious Disease : An Official Journal of the Transplantation Society. 2023.
8. Contemporary Risk Factors and Outcomes of Transfusion-Associated Circulatory Overload. — Roubinian NH, Hendrickson JE, Triulzi DJ, et al. Critical Care Medicine. 2018.
9. The Prevention of Transfusion-Associated Circulatory Overload. — Alam A, Lin Y, Lima A, Hansen M, Callum JL. Transfusion Medicine Reviews. 2013.
10. Indications for and Adverse Effects of Red-Cell Transfusion. — Carson JL, Triulzi DJ, Ness PM. The New England Journal of Medicine. 2017.
11. Transfusion‐related acute lung injury and other respiratory‐related transfusion reactions. — E. Alexander Dent, H. Clifford Sullivan Rossi's Principles of Transfusion Medicine 6e. 2022.
12. Pulmonary Edema After Transfusion: How to Differentiate Transfusion-Associated Circulatory Overload From Transfusion-Related Acute Lung Injury. — Gajic O, Gropper MA, Hubmayr RD. Critical Care Medicine. 2006.
13. Pulmonary Transfusion Reactions as an Immunological Spectrum Disorder. — Lowack J, Vlaar AP, Klanderman RB, Peters AL. Current Opinion in Immunology. 2025.
14. Transfusion-Related Pulmonary Complications in Paediatric Acute Myeloid Leukaemia: A Case Report of Transfusion-Associated Circulatory Overload (TACO) and Transfusion-Related Acute Lung Injury (TRALI). — Guariento M, Echecopar C, Galán-Gómez V, et al. Transfusion Medicine. 2026.
15. Transfusion-Associated Circulatory Overload-a Systematic Review of Diagnostic Biomarkers. — Klanderman RB, Bosboom JJ, Migdady Y, et al. Transfusion. 2019.
16. How I Diagnose and Treat Cardiorespiratory Complications of Transfusion. — Vlaar APJ, Zwaginga JJ, Wiersum-Osselton JC. Blood. 2025.
17. Noninfectious Transfusion-Associated Adverse Events and Their Mitigation Strategies. — Goel R, Tobian AAR, Shaz BH. Blood. 2019.