Transfusion-Related Acute Lung Injury (TRALI)
TRALI is a life-threatening, non-cardiogenic pulmonary edema occurring during or within 6 hours of blood product transfusion, representing a leading cause of transfusion-related mortality with an o…
TRALI is a life-threatening, non-cardiogenic pulmonary edema occurring during or within 6 hours of blood product transfusion, representing a leading cause of transfusion-related mortality with an overall mortality rate of 6–12% (exceeding 40% in critically ill patients).[1-2] It is mediated primarily through a "two-hit" model: a recipient priming event (e.g., sepsis, surgery) followed by a transfusion-related trigger (donor anti-HLA/anti-HNA antibodies or bioactive lipids).[3-4] Current consensus distinguishes TRALI type I (no pre-existing ARDS risk factor) from TRALI type II (pre-existing ARDS risk factor with stable respiratory status in the 12 hours before transfusion).[5]
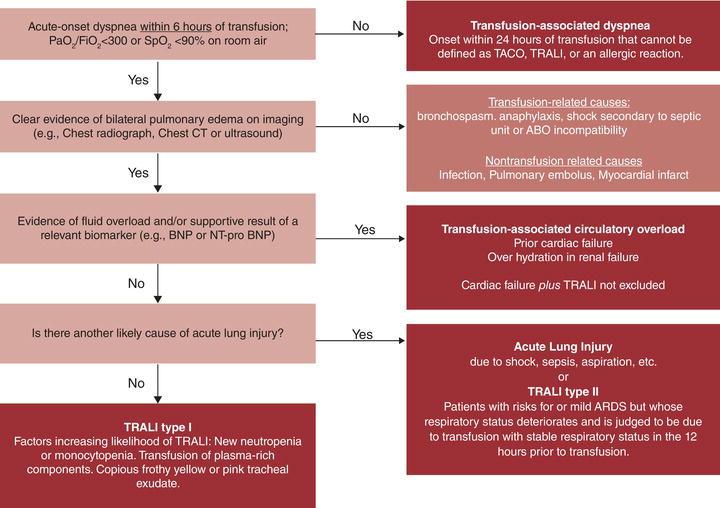
The following diagnostic algorithm illustrates the approach to acute dyspnea within 6 hours of transfusion:
1. History
- Temporal relationship: Onset of respiratory distress during or within 6 hours of any blood product transfusion (pRBCs, FFP, platelets, whole blood, cryoprecipitate)[3-4]
- Characterize dyspnea: acute onset, rapidly progressive, severity of hypoxia
- Ask about the type, volume, and number of blood products transfused and timing of symptom onset relative to transfusion
- Inquire about prior transfusion reactions or prior TRALI episodes
- Assess for pre-existing conditions that may serve as the "first hit": recent surgery (especially liver surgery), sepsis/infection, mechanical ventilation, trauma, massive transfusion[3][7]
- Important negatives: no prior heart failure symptoms, no recent volume overload, no known allergies to blood products
2. Alarm Features
- Acute hypoxemia (PaO₂/FiO₂ ≤ 300 mmHg) with rapid desaturation[4]
- Severe respiratory distress requiring intubation
- Hypotension — can progress to cardiovascular collapse
- Copious frothy pink-tinged secretions from the endotracheal tube[3]
- Fever with rigors (may mimic septic transfusion reaction)
- Transient leukopenia — a relatively specific finding that may help distinguish TRALI from TACO[3]
- Any respiratory deterioration during or shortly after transfusion should prompt immediate cessation of the transfusion
3. Medications
- No specific pharmacologic therapy is proven effective for TRALI[4][8]
- Diuretics are NOT indicated — TRALI is non-cardiogenic edema; diuresis may worsen hypotension[4][9]
- Corticosteroids: role is unproven; not routinely recommended[4][8]
- Vasopressors may be needed for refractory hypotension[9]
- Avoid further transfusions unless absolutely necessary; if transfusion is critical, use products from male-only donors or antibody-screened donors[3][7]
- Caution: if TACO is also suspected (overlap cases), diuretics may be considered, but this requires careful clinical judgment[10]
4. Diet
- Not directly applicable in the acute setting
- NPO if intubation is anticipated or the patient is hemodynamically unstable
- Fluid restriction is recommended as part of a restrictive fluid strategy consistent with ARDS management[3][8]
5. Review of Systems
- Pulmonary: dyspnea, cough, frothy sputum, chest tightness
- Cardiovascular: hypotension, tachycardia (distinguish from hypertension/JVD seen in TACO)
- Constitutional: fever, rigors, chills (present in ~30% of cases)[3]
- Skin: flushing, urticaria (if present, consider anaphylactic transfusion reaction)
- GI: nausea (nonspecific)
- Neurologic: altered mental status from hypoxia
6. Collateral History and Family History
- Donor history is critical: obtain information from the blood bank regarding donor sex, parity, and antibody status — plasma from multiparous female donors carries the highest risk due to HLA antibodies (prevalence ~24% in previously pregnant women)[4][7]
- Confirm blood product type, storage duration, and lot numbers for hemovigilance reporting
- Family history is not directly relevant to TRALI pathogenesis
- Social history: chronic alcohol abuse and current smoking are independent recipient risk factors[3][7]
7. Risk Factors
Recipient (first hit) risk factors
- Liver surgery
- Chronic alcohol abuse
- Sepsis/shock
- High peak airway pressures during mechanical ventilation
- Current smoking
- Positive fluid balance
- Elevated IL-8 levels
- ICU or perioperative setting
Transfusion (second hit) risk factors
- Plasma from female donors (especially multiparous) — OR 4.5 for TRALI
- High-volume plasma-rich components (FFP, apheresis platelets)
- Donor anti-HLA class I, class II, or anti-HNA antibodies (especially HNA-3a)
- Bioactive lipids accumulating during prolonged storage of cellular blood products
- Multiple transfusions / massive transfusion protocols
8. Differential Diagnosis
- Transfusion-associated circulatory overload (TACO) — the most important differential; characterized by hydrostatic (cardiogenic) edema, elevated BNP, hypertension, JVD, response to diuretics[11]
- Septic transfusion reaction — bacterial contamination of blood products; high fever, rigors, hypotension; blood cultures of product and patient are diagnostic
- Anaphylactic transfusion reaction — urticaria, angioedema, bronchospasm, hypotension; typically in IgA-deficient recipients
- Acute respiratory distress syndrome (ARDS) from other causes — pneumonia, aspiration, pancreatitis; distinguished by whether transfusion is the likely cause[5]
- Acute hemolytic transfusion reaction — flank pain, hemoglobinuria, DIC; ABO incompatibility
- Cardiogenic pulmonary edema — pre-existing heart failure exacerbation
- Pulmonary embolism — acute dyspnea and hypoxia but typically without bilateral infiltrates
Key distinguishing features of TRALI vs. TACO
- Export Feature TRALI TACO References Edema type Non-cardiogenic (permeability) Cardiogenic (hydrostatic)[1]
- BNP/NT-proBNP Normal or mildly elevated Significantly elevated[1-2]
- Blood pressure Often hypotensive Often hypertensive[1, 3]
- Fluid balance Variable Positive[1]
- Fever Common Uncommon[3]
- Response to diuretics No improvement Improvement[1, 4]
- Edema fluid protein High (exudative) Low (transudative)[1]
- Leukopenia May be present (transient) Absent[3]
9. Past Medical History
- Prior transfusion reactions or prior TRALI episodes (recurrence is possible if re-exposed to the same antibody)
- Chronic liver disease, cirrhosis
- Hematologic malignancies requiring frequent transfusions
- Recent surgery (especially hepatic, cardiac, or major abdominal)
- Chronic lung disease (may worsen presentation)
- Heart failure history (important to distinguish TACO)
- Renal disease (fluid management implications)
10. Physical Exam
- Vitals: Tachypnea, tachycardia, hypotension (distinguishes from TACO which tends toward hypertension), fever, hypoxemia on pulse oximetry[3]
- Pulmonary: Bilateral crackles/rales, decreased breath sounds, increased work of breathing
- Cardiovascular: Assess for JVD (absent in TRALI, present in TACO), S3 gallop (absent in TRALI), peripheral edema
- Airway: Frothy pink-tinged secretions if intubated[3]
- Skin: Cyanosis from hypoxemia; check for urticaria/angioedema (suggests allergic reaction instead)
- Abdomen: Assess for hepatomegaly (volume overload)
11. Lab Studies
- ABG: Assess PaO₂/FiO₂ ratio (≤300 mmHg consistent with acute lung injury)[4]
- CBC: Transient leukopenia is a relatively specific finding; also assess for hemolysis (hemolytic reaction)[3]
- BNP/NT-proBNP: Normal or mildly elevated in TRALI; significantly elevated in TACO — key differentiating biomarker[10-11]
- Comprehensive metabolic panel: Renal function, electrolytes
- Blood cultures (patient and implicated blood product): Rule out septic transfusion reaction
- Direct antiglobulin test (DAT): Rule out acute hemolytic transfusion reaction
- LDH, haptoglobin, bilirubin: Hemolysis workup if suspected
- Donor antibody testing: Anti-HLA class I/II and anti-HNA antibodies in donor plasma (coordinate with blood bank)[4][12]
- Recipient HLA/HNA typing: To confirm cognate antibody-antigen match
- Emerging biomarkers: IL-6 (pro-inflammatory, elevated in TRALI) and IL-10 (anti-inflammatory) may help differentiate TRALI from TACO[13]
12. Imaging
- Chest X-ray (first-line): Bilateral pulmonary infiltrates consistent with pulmonary edema, without cardiomegaly or vascular cephalization (which would suggest TACO)[3-4]
- Findings are non-specific and can be indistinguishable from ARDS or TACO on imaging alone
- CXR should improve within 96 hours in typical TRALI[9]
- CT chest: Not routinely required; may help if diagnosis is uncertain or alternative pathology is suspected (e.g., PE)
- Echocardiography: Useful to assess cardiac function and exclude cardiogenic edema; expected to show normal left ventricular function and normal filling pressures in TRALI[11]
- Lung ultrasound: Point-of-care tool to assess for B-lines (bilateral), pleural effusions, and cardiac function
13. Special Tests
- Pulmonary artery catheterization (if available): Pulmonary capillary wedge pressure (PCWP) ≤18 mmHg supports non-cardiogenic edema (TRALI); >18 mmHg suggests TACO[4][12]
- Edema fluid protein analysis (if intubated): Edema fluid-to-plasma protein ratio >0.65 indicates exudative (permeability) edema consistent with TRALI[11]
Donor antibody workup (coordinate with blood bank)
- HLA class I and class II antibody screening
- Granulocyte immunofluorescence test (GIFT) for anti-HNA antibodies
- Crossmatch of donor serum against recipient neutrophils/lymphocytes
- Hemovigilance reporting: Mandatory reporting to the blood bank and transfusion service for all suspected TRALI cases
14. ECG
- ECG is indicated to rule out acute cardiac pathology (MI, arrhythmia) as a cause of pulmonary edema
- TRALI itself does not produce specific ECG changes
- Sinus tachycardia is the most common finding
- Look for signs of right heart strain (acute cor pulmonale) in severe cases: right axis deviation, S1Q3T3, RV strain pattern
- Absence of LVH, atrial enlargement, or ischemic changes helps distinguish from cardiogenic edema
15. Assessment
TRALI is a clinical diagnosis based on
- Acute onset of hypoxemia (PaO₂/FiO₂ ≤ 300) and bilateral pulmonary edema
- Temporal association with transfusion (during or within 6 hours)
- No pre-existing acute lung injury before transfusion (TRALI type I) OR pre-existing ARDS risk factor with stable respiratory status in the prior 12 hours that acutely worsens (TRALI type II)
- Absence of circulatory overload as the primary cause
- Severity stratification: Ranges from mild (supplemental O₂ only) to severe (requiring intubation/mechanical ventilation or ECMO). Mortality is 6–12% overall but exceeds 40% in critically ill patients.[1-2] Most patients who survive recover within 48–96 hours.[9][14]
- Atypical presentations include delayed onset (up to 72 hours), isolated hypotension without significant respiratory symptoms, or overlap with TACO (TRALI/TACO overlap).[3][10][13]
16. Treatment Plan
Immediate actions
- Stop the transfusion immediately[9]
- Maintain IV access; do NOT discard the blood product — return it to the blood bank for investigation
- Notify the blood bank/transfusion service
Supportive care (mainstay of treatment)
- Supplemental oxygen: Titrate to maintain SpO₂ >92%
- Mechanical ventilation if needed: Use lung-protective ventilation (tidal volume 6 mL/kg ideal body weight, plateau pressure <30 cmH₂O, appropriate PEEP) per ARDS management protocols
- Restrictive fluid strategy: Avoid aggressive IV fluids; conservative fluid management as in ARDS[3][8]
- Vasopressors (norepinephrine preferred) for refractory hypotension[9]
- ECMO: Consider in refractory hypoxemia not responsive to conventional mechanical ventilation[9]
What NOT to do
- Do NOT give diuretics (non-cardiogenic edema; may worsen hypotension)[4]
- Do NOT give corticosteroids routinely (no proven benefit)[4][8]
Prevention for future transfusions
- Adopt a restrictive transfusion strategy — avoid unnecessary transfusions
- Use male-only donor plasma and screen female apheresis platelet donors for HLA antibodies
- If the implicated donor is identified with cognate antibodies, permanently defer that donor from donating plasma-containing products
- Consider alternatives to plasma (e.g., prothrombin complex concentrates, fibrinogen concentrate) when clinically appropriate
17. Disposition
- Admit to ICU if: intubation required, hemodynamic instability, severe hypoxemia, or ongoing clinical deterioration[8]
- Monitored bed/step-down: Mild cases with stable vitals responding to supplemental O₂ alone
- Observation: Minimum 24 hours of monitoring even for mild cases, given potential for delayed worsening
Specialist consultation triggers
- Pulmonary/critical care for ventilator management
- Transfusion medicine/hematology for donor workup and hemovigilance
- Blood bank notification is mandatory for all suspected cases
18. Follow Up / Return Precautions
- Expected recovery: Most patients improve within 48–96 hours; CXR should clear within 4 days. No permanent pulmonary sequelae are expected in survivors.[9][14]
- Hemovigilance: Ensure the case is reported to the institutional transfusion committee and national hemovigilance system (e.g., FDA in the US)[5]
- Future transfusion planning: Document the reaction in the medical record; if the patient requires future transfusions, use products from male donors or antibody-negative donors; avoid products from the implicated donor[3]
- Return precautions (if discharged): Return immediately for recurrent dyspnea, fever, chest pain, or any respiratory distress — especially if receiving further transfusions
- Follow-up: Pulmonary follow-up in 1–2 weeks to confirm radiographic resolution; repeat PFTs if symptoms persist beyond expected recovery window
References
1. Transfusion-Related Acute Lung Injury: From Mechanistic Insights to Therapeutic Strategies. — Fang X, Mo C, Zheng L, et al. Advanced Science. 2025.
2. Transfusion-Related Acute Lung Injury: Experimental Models to Study Pathogenesis and Therapeutic Strategies. — Rayatdoost F, Kapur R. Current Opinion in Immunology. 2025.
3. Transfusion Reactions: Prevention, Diagnosis, and Treatment. — Delaney M, Wendel S, Bercovitz RS, et al. Lancet. 2016.
4. Transfusion-Related Acute Lung Injury: Current Concepts for the Clinician. — Triulzi DJ. Anesthesia and Analgesia. 2009.
5. Transfusion-Related Acute Lung Injury: 36 Years of Progress (1985-2021). — Toy P, Looney MR, Popovsky M, et al. Annals of the American Thoracic Society. 2022.
6. Transfusion‐related acute lung injury and other respiratory‐related transfusion reactions. — E. Alexander Dent, H. Clifford Sullivan Rossi's Principles of Transfusion Medicine 6e. 2022.
7. Transfusion-Related Acute Lung Injury: Incidence and Risk Factors. — Toy P, Gajic O, Bacchetti P, et al. Blood. 2012.
8. State of the Art Management of Transfusion-Related Acute Lung Injury (TRALI). — Goldberg AD, Kor DJ. Current Pharmaceutical Design. 2012.
9. Transfusion related acute lung injury: A pediatric perspective. — Sanchez R, Toy P. Pediatric Blood & Cancer. 2005.
10. How I Diagnose and Treat Cardiorespiratory Complications of Transfusion. — Vlaar APJ, Zwaginga JJ, Wiersum-Osselton JC. Blood. 2025.
11. Transfusion-Associated Circulatory Overload and Transfusion-Related Acute Lung Injury. — Semple JW, Rebetz J, Kapur R. Blood. 2019.
12. Transfusion-Related Acute Lung Injury: A Review. — Looney MR, Gropper MA, Matthay MA. Chest. 2004.
13. Pulmonary Transfusion Reactions as an Immunological Spectrum Disorder. — Lowack J, Vlaar AP, Klanderman RB, Peters AL. Current Opinion in Immunology. 2025.
14. Indications for and Adverse Effects of Red-Cell Transfusion. — Carson JL, Triulzi DJ, Ness PM. The New England Journal of Medicine. 2017.