Traumatic Aortic Disruption
Traumatic aortic disruption (blunt traumatic aortic injury, BTAI) is the second-most common cause of death in blunt trauma patients, resulting from high-energy deceleration forces. Only 9%–14% of p…
Traumatic aortic disruption (blunt traumatic aortic injury, BTAI) is the second-most common cause of death in blunt trauma patients, resulting from high-energy deceleration forces. Only 9%–14% of patients with traumatic aortic rupture survive to reach the hospital, and untreated, approximately 30% of those admitted will die within 24 hours.[1-3] The most common injury site is the aortic isthmus (~45%), the transition point between the mobile aortic arch and the fixed descending aorta.[1][3]
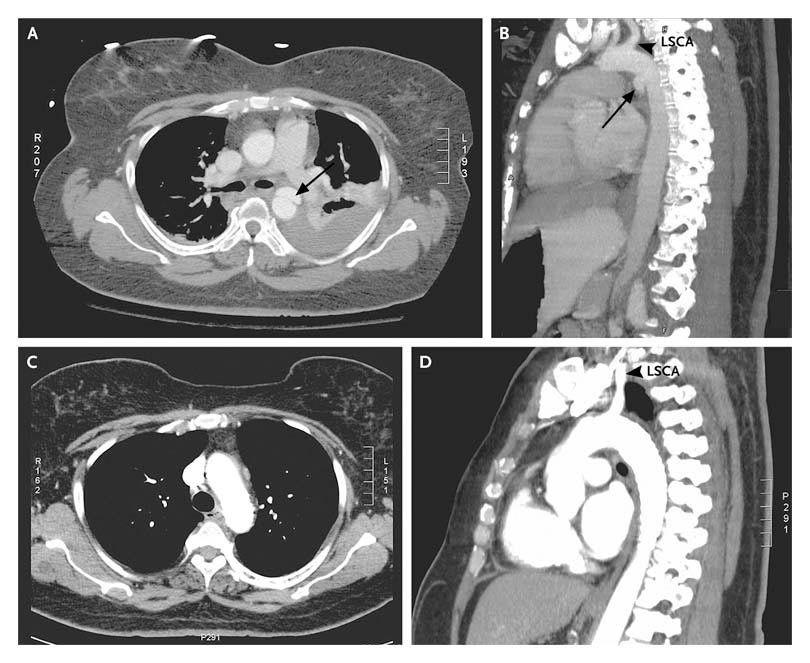
The following CT angiography images demonstrate a traumatic pseudoaneurysm at the aortic isthmus before and after endovascular repair:
View full figure Figure 3. Aortic Injury with Associated Pseudoaneurysm. Blunt Aortic Injury. N Engl J Med. October 15, 2008.
1. History
- Mechanism: High-energy deceleration — motor vehicle collisions (frontal and especially lateral impact), falls from height, motorcycle/pedestrian vs. auto, crush injuries[3-4]
- Characterize speed, restraint use, airbag deployment, ejection, steering wheel deformity, height of fall
- Patients may report severe chest or interscapular back pain, dyspnea, or may be asymptomatic depending on injury grade[4]
- Symptoms range from completely asymptomatic (low-grade intimal tears) to hemorrhagic shock (free rupture)[4]
- Ask about loss of consciousness, associated injuries (head, abdomen, pelvis, long bones)
- Important negatives: absence of chest pain does not exclude BTAI
2. Alarm Features
- Refractory hypotension/hemorrhagic shock — suggests grade IV (free rupture)[1][4]
- Expanding mediastinal hematoma
- Active external hemorrhage or pulsatile hematoma
- Absent or diminished distal pulses / limb ischemia[4]
- New-onset upper extremity hypertension with lower extremity hypotension ("pseudocoarctation")[3]
- Harsh interscapular systolic murmur[3]
- Left hemothorax
- Signs of cardiac tamponade (if ascending aorta involved)
- Any high-energy mechanism with unexplained hemodynamic instability
3. Medications
Anti-impulse therapy (cornerstone of initial management)
- IV esmolol (first-line): titratable, short-acting beta-blocker; target HR <60 bpm, SBP <100–120 mmHg[1][3-4]
- IV labetalol: combined alpha/beta blockade, useful alternative
- IV nicardipine or clevidipine: if additional BP control needed after beta-blockade achieved
- IV nitroprusside: only after adequate beta-blockade to avoid reflex tachycardia[3]
- Non-dihydropyridine calcium channel blockers (diltiazem, verapamil) if beta-blockers contraindicated[3]
Contraindicated/Cautions
- Do NOT initiate vasodilators before rate control (risk of reflex tachycardia worsening aortic wall stress)[3]
- Beta-blockers used cautiously with concurrent acute aortic regurgitation[3]
- Anticoagulation during TEVAR should be balanced against overall bleeding risk in polytrauma; no heparin vs. low-dose vs. full heparin showed no difference in outcomes in small studies[1]
4. Diet
- NPO status in the ED for all suspected BTAI (anticipate operative intervention)
- No specific dietary triggers or long-term dietary management unique to this condition
- Long-term: standard cardiovascular risk reduction diet if hypertension is a comorbidity
5. Review of Systems
- Cardiovascular: chest pain, palpitations, syncope, pulse discrepancies
- Respiratory: dyspnea, hemoptysis (rare)
- Neurologic: altered mental status, focal deficits (stroke from arch vessel involvement), paraplegia (spinal cord ischemia)
- GI/GU: abdominal pain (concomitant abdominal aortic or visceral injury)
- MSK: back pain (interscapular), extremity pain/deformity (associated fractures)
- Vascular: cool/pulseless extremities
6. Collateral History and Family History
- Collateral: EMS report is critical — mechanism details, speed, extrication time, field vitals, GCS trend
- Bystander account of the event, especially if patient is altered
- Family history: connective tissue disorders (Marfan, Loeys-Dietz, Ehlers-Danlos vascular type) increase aortic vulnerability, though BTAI is overwhelmingly mechanism-driven[3][5]
- Prior aortic surgery or known aortic aneurysm
7. Risk Factors
- High-energy deceleration mechanism — the dominant risk factor[3-4]
- MVC (especially lateral impact, unrestrained, high speed)
- Falls from significant height
- Motorcycle/bicycle crashes
- Pedestrian struck
- Side-impact crashes account for ~44% of fatal traumatic aortic ruptures[3]
- Pre-existing aortic pathology (aneurysm, connective tissue disease, bicuspid aortic valve)[3]
- Older age (less compliant aorta)
- No restraint use / no airbag deployment
8. Differential Diagnosis
- Traumatic hemothorax (from rib fractures, intercostal vessels, lung laceration) — most common cause of mediastinal widening mimic
- Cardiac contusion / myocardial rupture — ECG changes, troponin elevation, tamponade
- Traumatic diaphragmatic rupture — abnormal CXR, bowel in thorax
- Esophageal rupture — pneumomediastinum, subcutaneous emphysema
- Tracheobronchial injury — massive air leak, pneumomediastinum
- Great vessel branch injury (subclavian, innominate) — pulse deficits, expanding hematoma
- Sternal/rib fractures with mediastinal hematoma (venous bleeding, not aortic)
- Pericardial tamponade from other causes
- Cannot-miss: Free aortic rupture (grade IV) — rapidly fatal without intervention[1]
9. Past Medical History
- Prior aortic surgery or endovascular repair
- Known aortic aneurysm or dissection
- Connective tissue disorders
- Hypertension (chronic aortic wall stress)
- Prior cardiac surgery
- Anticoagulant/antiplatelet use (affects bleeding risk and surgical planning)
- Chronic kidney disease (contrast considerations for CTA)
10. Physical Exam
Vital signs
- Hypotension (present in ~17–20% on arrival)[1][6]
- Tachycardia
- Blood pressure differential between upper and lower extremities
Focused exam
- "Pseudocoarctation" signs: upper extremity hypertension with diminished femoral pulses, radial-femoral pulse delay[3]
- Harsh systolic murmur over the interscapular region[3]
- Chest wall ecchymosis, seatbelt sign, steering wheel imprint
- Absent or diminished distal pulses, limb ischemia[4]
- Pulsatile or expanding hematoma
- Signs of associated injuries: flail chest, pelvic instability, long bone deformity, abdominal tenderness
- FAST exam for hemopericardium/hemoperitoneum
11. Lab Studies
- Type and crossmatch — immediate, anticipate massive transfusion
- CBC: baseline hemoglobin/hematocrit (serial monitoring)
- BMP/CMP: renal function (pre-contrast), electrolytes
- Coagulation studies: PT/INR, PTT, fibrinogen (DIC screening in massive hemorrhage)
- Lactate: marker of tissue hypoperfusion/shock severity
- ABG/VBG: acid-base status, base deficit (correlates with hemorrhage severity)
- Troponin: rule out concurrent cardiac contusion
- TEG/ROTEM: if available, guides resuscitation in massive transfusion
- No lab test is diagnostic for BTAI — diagnosis is imaging-based.
12. Imaging
First-line / Gold standard
- CT angiography (CTA) of the chest — sensitivity approaching 100%, accuracy 99.7%, NPV 100%. This is the definitive diagnostic study.[2][7-9]
Chest X-ray
- Classic finding is mediastinal widening, but CXR is not a reliable screening tool[8]
- A prospective AAST/ATF registry study found classic CXR findings present in only 57.6% of confirmed BTAIs, and widened mediastinum in only 27.7% overall (47.4% of grade IV)[8]
- A normal CXR does NOT exclude BTAI[2][8]
- Other CXR findings (when present): loss of aorticopulmonary window, rightward tracheal deviation, left apical cap, depression of left mainstem bronchus, widened left paraspinal line, NG tube deviation[2]
- TEE: Useful bedside alternative in hemodynamically unstable patients who cannot be transported to CT[10]
- When imaging is unnecessary: If mechanism is clearly low-energy and clinical suspicion is negligible, CTA may be deferred per ATLS protocols
13. Special Tests
- Grading system (SVS/Estrera classification) — guides management:[1][4]
- Export Grade Description Management References I Intimal tear Nonoperative: anti-impulse therapy, repeat CTA 24–48h[1-3]
- II Intramural hematoma Nonoperative if no high-risk features; TEVAR if high-risk imaging features[1, 3]
- III Pseudoaneurysm TEVAR (preferred); timing may be delayed >24h in stable patients[1-2, 4]
- IV Free rupture Emergent operative repair (TEVAR or open)[1-2]
- High-risk imaging features for Grade II (favor TEVAR): posterior mediastinal hematoma >10 mm, lesion-to-normal aortic diameter ratio >1.4, mediastinal hematoma with mass effect, pseudocoarctation, left hemothorax, arch involvement[4]
- FAST: Low sensitivity for BTAI but useful for detecting hemopericardium/hemoperitoneum
- Intravascular ultrasound (IVUS): Adjunct in equivocal cases[3]
14. ECG
- ECG is part of standard trauma evaluation but is not diagnostic for BTAI
Obtain to evaluate for
- Cardiac contusion: ST changes, new arrhythmias, conduction abnormalities
- STEMI: rare complication if dissection extends to coronary ostia
- Pericardial tamponade: low voltage, electrical alternans
- Sinus tachycardia (hemorrhage, pain, sympathetic activation)
15. Assessment
- BTAI is a time-critical, life-threatening injury requiring a high index of suspicion based on mechanism alone[1][4]
- Presentation ranges from asymptomatic (grade I intimal tear) to hemorrhagic shock (grade IV free rupture)[4]
- ~80–90% die at the scene; in-hospital mortality ~19%[1][3][12]
- Concomitant injuries are the rule, not the exception — TBI in ~28–50%, solid organ injury, rib/pelvic fractures[1][11]
- Severity stratification by SVS grading system directly determines management pathway[1][4]
- Atypical presentations: completely normal exam, normal CXR, delayed presentation with chronic pseudoaneurysm
- Complications: free rupture, aortic-related death, spinal cord ischemia (from repair), stroke, renal failure, left subclavian artery coverage sequelae
16. Treatment Plan
Initial stabilization (all grades)
- ATLS primary/secondary survey
- Anti-impulse therapy: IV beta-blocker (esmolol or labetalol) targeting SBP <100–120 mmHg, HR <60–80 bpm — unless hypotensive/in shock[1][3-4]
- Massive transfusion protocol activation if hemorrhagic shock
- Adequate analgesia (reduces sympathetic drive)
Grade-specific management
- Grade I: Medical management with anti-impulse therapy; repeat CTA at 24–48 hours; 0% mortality with medical management in original series[1][6]
- Grade II without high-risk features: Nonoperative management with close surveillance[4][6]
- Grade II with high-risk features: TEVAR[4]
- Grade III: TEVAR is first-line when anatomy is suitable; delayed repair (>24h) may be preferred to allow stabilization of concomitant injuries[1][4][11]
- Grade IV: Emergent operative intervention — TEVAR if feasible, or emergent thoracotomy with aortic cross-clamping for hemorrhage control[1][4][13]
TEVAR vs. Open repair
- TEVAR has become the predominant approach (open repair decreased from 7.5% to 1.9% between 2007–2015)[1]
- Meta-analyses show TEVAR has lower 30-day mortality (7.9% vs. 20%), with similar rates of paraplegia and stroke[14]
- Long-term survival is similar once patients survive the index hospitalization[15]
- Higher 1-year reintervention rate with TEVAR (6% vs. 0%)[14]
- Concomitant TBI: Emergent TEVAR may be justified to allow earlier liberalization of blood pressure targets for cerebral perfusion[11]
17. Disposition
- All confirmed BTAI requires admission — no outpatient management
- ICU admission for all grades requiring anti-impulse therapy and hemodynamic monitoring[4]
- Transfer to a trauma center with aortic repair capability if not already at one (Class I recommendation)[1]
- Immediate OR: Grade IV with hemodynamic instability[13]
- Urgent/semi-elective OR: Grade III (and high-risk grade II) once stabilized
Consultation triggers
- Vascular surgery / cardiothoracic surgery — all confirmed BTAI
- Trauma surgery — polytrauma management
- Neurosurgery — concurrent TBI
- Interventional radiology — if hybrid OR approach considered
18. Follow-Up / Return Precautions
Post-TEVAR surveillance (per 2026 SVS focused update)
- CTA at 1, 6, and 12 months, then annually
- Monitor for endoleak, stent graft migration, device-related complications
- Injury progression occurs in ~7.6% of nonoperatively managed patients on surveillance imaging[1]
Nonoperatively managed injuries
- Grade I: May not require follow-up imaging per updated SVS guidelines[11]
- Grade II: CTA at 1 month[11]
- All nonoperatively managed patients should have repeat CTA at 24–48 hours initially[1][4]
Long-term considerations
- Lifelong blood pressure control
- Loss to follow-up is a significant problem in the trauma population[13]
- Long-term durability data for TEVAR in young trauma patients remain limited[1][16]
- Early involvement of specialized surgeons improves follow-up compliance[13]
- Return precautions (for patients discharged after nonoperative management):
- Return immediately for new or worsening chest/back pain, dyspnea, syncope, signs of limb ischemia, or hemodynamic instability
References
1. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. — Isselbacher EM, Preventza O, Hamilton Black Iii J, et al. Journal of the American College of Cardiology. 2022.
2. Blunt Aortic Injury. — Neschis DG, Scalea TM, Flinn WR, Griffith BP. The New England Journal of Medicine. 2008.
3. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease. A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology,American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons,and Society for Vascular Medicine. — Hiratzka LF, Bakris GL, Beckman JA, et al. Journal of the American College of Cardiology. 2010.
4. EACTS/STS Guidelines for Diagnosing and Treating Acute and Chronic Syndromes of the Aortic Organ. — Czerny M, Grabenwöger M, Berger T, et al. European Journal of Cardio-Thoracic Surgery : Official Journal of the European Association for Cardio-Thoracic Surgery. 2024.
5. Thoracic Aortic Aneurysm and Dissection. — Goldfinger JZ, Halperin JL, Marin ML, et al. Journal of the American College of Cardiology. 2014.
6. Outcomes and Practice Patterns of Medical Management of Blunt Thoracic Aortic Injury From the Aortic Trauma Foundation Global Registry. — Arbabi CN, DuBose J, Charlton-Ouw K, et al. Journal of Vascular Surgery. 2022.
7. Early Clinical Diagnosis and Treatment of Traumatic Aortic Injury Caused by Thoracic and Abdominal Injuries: A Series of Four Cases with Literature Review. — Wu Q, Sun S, Xie J, et al. BioMed Research International. 2021.
8. Is Chest X-Ray a Reliable Screening Tool for Blunt Thoracic Aortic Injury? Results From the American Association for the Surgery of Trauma/Aortic Trauma Foundation Prospective Blunt Thoracic Aortic Injury Registry. — Crapps JL, Efird J, DuBose JJ, et al. Journal of the American College of Surgeons. 2023.
9. Best Practices Guidelines In Imaging. — Gail T. Tominaga MD FACS, Mark Bernstein MD, Michael R. Aquino MD MHSc, et al American College of Surgeons (2018). 2018.
10. 2010 ACCF/AHA/AATS/ACR/ASA/SCA/SCAI/SIR/STS/SVM Guidelines for the Diagnosis and Management of Patients With Thoracic Aortic Disease: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. — Hiratzka LF, Bakris GL, Beckman JA, et al. Circulation. 2010.
11. The Society for Vascular Surgery Clinical Practice Guideline on the Management of Blunt Thoracic Aortic Injury: A Focused Update. — DuBose J, Kundi R, Curi MA, et al. Journal of Vascular Surgery. 2026.
12. Endovascular Repair of Blunt Aortic Trauma: A Multidisciplinary Approach and a Retrospective Multicenter Study. — Di Sario I, Franceschini E, Gatta E, Pagliariccio G. Journal of Clinical Medicine. 2025.
13. Thoracic Trauma WSES-AAST Guidelines. — Coccolini F, Cremonini C, Moore EE, et al. World Journal of Emergency Surgery : WJES. 2025.
14. A Systematic Review and Meta-Analysis of Endovascular Versus Open Surgical Repair for the Traumatic Ruptured Thoracic Aorta. — Harky A, Bleetman D, Chan JSK, et al. Journal of Vascular Surgery. 2020.
15. Long-term Outcomes of Endovascular and Open Repair for Traumatic Thoracic Aortic Injury. — Cheng YT, Cheng CT, Wang SY, et al. JAMA Network Open. 2019.
16. Thoracic Endovascular Repair (TEVAR) Versus Open Surgery for Blunt Traumatic Thoracic Aortic Injury. — Pang D, Hildebrand D, Bachoo P. The Cochrane Database of Systematic Reviews. 2019.