Trigeminal Neuralgia
Trigeminal neuralgia (TN) is a chronic neuropathic pain condition characterized by sudden, brief episodes of severe, electric shock–like, lancinating unilateral facial pain in one or more trigemina…
Trigeminal neuralgia (TN) is a chronic neuropathic pain condition characterized by sudden, brief episodes of severe, electric shock–like, lancinating unilateral facial pain in one or more trigeminal nerve distributions, triggered by innocuous stimuli.[1-2] It is classified as classic (neurovascular compression, ~75%), secondary (~15%, due to MS or tumor), or idiopathic (~10%).[1] Average age of onset is 50–60 years, with higher prevalence in women and increasing incidence with age.[2]
1. History
- Character of pain: Electric shock–like, shooting, stabbing, sharp — paroxysms lasting a fraction of a second to 2 minutes (usually seconds)[1][3]
- Location: Unilateral, most commonly V2 (maxillary) or V3 (mandibular); right side more common than left[1]
- Triggers: Light touch to face, talking, chewing, brushing teeth, shaving, wind/breeze across trigger zone. Trigger zones are small, discrete areas — nearly pathognomonic for TN[2][4]
- Frequency: Attacks may recur hundreds of times per day; episodes cluster over weeks to months with pain-free intervals lasting months to years[2]
- Refractory period: Some patients note a brief period after a paroxysm during which additional pain cannot be triggered[4]
- Concomitant continuous pain: A subset has mild-to-moderate background aching/throbbing between paroxysms[2-3]
- Important negatives: No numbness (suggests neuropathy), no persistent burning, no bilateral simultaneous pain, no pain outside trigeminal territory[4]
2. Alarm Features
- Bilateral pain — raises concern for MS, systemic disease, or non-neurologic cranial pathology[1]
- Sensory loss/numbness in the trigeminal distribution — suggests secondary TN (tumor, MS, neuropathy)[2-3]
- Other neurologic deficits (weakness, ataxia, visual changes) — concerning for intracranial mass or demyelinating disease[1-2]
- Young age at onset (<40 years) — higher suspicion for MS-related TN[1]
- First division (V1) involvement alone — less typical; consider alternative diagnoses[5]
- Progressive pain with no remission periods — consider malignancy or infiltrative process[1]
- Severe exacerbation with inability to eat/drink — risk of dehydration and malnutrition; may require hospitalization[3]
3. Medications
First-line
- Carbamazepine — drug of choice; start 200 mg BID, titrate by 200 mg/day every few days to max 1,200 mg/day; NNT ~2 for meaningful pain relief; ~75% initial response rate[1-2][5]
- Oxcarbazepine — alternative first-line, 300–1,800 mg/day in divided doses; potentially fewer side effects; high cross-reactivity risk if allergic to carbamazepine[1-2][6]
Second-line / adjunctive
- Lamotrigine, gabapentin, pregabalin, baclofen, botulinum toxin type A, phenytoin — used as monotherapy or add-on when first-line fails[6]
Acute exacerbation (ED)
- IV fosphenytoin or IV lidocaine — limited evidence but clinical experience supports efficacy; requires monitored setting[3][7]
- Opioids are ineffective in safe doses and should be avoided[3]
- NSAIDs are generally ineffective for neuralgic pain[7]
- Lidocaine injection into trigger zones may provide short-term relief[3]
Contraindications/cautions for carbamazepine
- Cardiac conduction abnormalities (AV block)[1]
- Hepatic porphyria[8]
- HLA-B</em>15:02 screening required before initiation in patients of Southeast Asian, South Asian, or other at-risk ancestry — risk of fatal SJS/TEN. HLA-A</em>31:01 also associated with hypersensitivity in European, Korean, and Japanese populations[9-10]
- Side effects: dizziness, diplopia, ataxia, hyponatremia, elevated transaminases, Stevens-Johnson syndrome, aplastic anemia (rare), osteoporosis with long-term use[1-2]
- Significant drug-drug interactions (CYP3A4 inducer) — affects oral contraceptives, warfarin, many other medications[1]
- Carbamazepine may have a 50% failure rate over 5–10 years[2]
4. Diet
- During severe exacerbations, eating and drinking can trigger attacks, leading to dehydration and malnutrition — a key reason for hospitalization[3]
- Soft, room-temperature foods may reduce trigger stimulation during flares
- No specific long-term dietary modifications are evidence-based for TN
- Patients on carbamazepine should be counseled about adequate hydration given hyponatremia risk[8]
5. Review of Systems
- Neurologic: Visual changes, diplopia, limb weakness/numbness, gait instability (screen for MS)[1]
- Ophthalmologic: Eye redness, tearing (autonomic phenomena can occur during flares)[2]
- Dental: Prior dental procedures, tooth pain, jaw pain (>80% of TN patients initially seek dental evaluation)[2]
- ENT: Ear pain, hearing changes, nasal congestion, sinus symptoms
- Psychiatric: Depression, anxiety, suicidal ideation — TN profoundly impacts quality of life[2][11]
- Constitutional: Weight loss from inability to eat during exacerbations
6. Collateral History and Family History
- Family history of TN: 1–2% of patients may have a familial link; rare variants in voltage-gated ion channel genes have been identified[1-2]
- History of MS in patient or family — TN prevalence is 2–5% in MS patients (20-fold increased risk vs. general population)[1][12]
- Collateral from dentist: Prior dental evaluations, procedures, or extractions for presumed dental pain (common misdiagnosis)
- Social context: Functional impairment, inability to work, social withdrawal due to fear of triggering pain
7. Risk Factors
- Age >50 years — incidence increases with age[2]
- Female sex — higher prevalence[1-2]
- Multiple sclerosis — strongest disease association (OR 8.9 in one population study)[1][13]
- Hypertension — associated with higher TN incidence[2]
- Other neurovascular compression disorders (glossopharyngeal neuralgia, hemifacial spasm)[13]
- Systemic lupus erythematosus — emerging association (OR 2.84)[13]
- Hyperlipidemia and complex diabetes — associated in population-level data[13]
8. Differential Diagnosis
- Export Diagnosis Distinguishing Features References Dental pain (caries, cracked tooth, pulpitis) Localized; related to biting or hot/cold foods; visible oral abnormalities[1-2]
- Glossopharyngeal neuralgia Pain in tongue, pharynx, or deep ear; triggered by swallowing/coughing[1-2]
- TMJ disorder Persistent aching pain near ear/jaw; bilateral possible; jaw clicking[1-2]
- Cluster headache Longer-lasting (15–180 min); orbital/supraorbital; prominent autonomic symptoms; restlessness[1-2]
- SUNCT/SUNA Periocular; prominent autonomic symptoms; no refractory period; can change sides[1-2]
- Paroxysmal hemicrania Forehead/eye pain; autonomic symptoms; responds to indomethacin[1-2]
- Postherpetic neuralgia Continuous burning pain; history of herpes zoster; often V1[1-2]
- Persistent idiopathic facial pain Dull, aching, constant; poorly localized; no trigger zones[2-3]
- Intracranial tumor Progressive; may have other neurologic signs[1, 4]
- Giant cell arteritis Persistent temporal pain; jaw claudication; age >50; elevated ESR/CRP[1, 5]
- Trigeminal neuropathy Persistent pain with sensory loss; history of trauma or autoimmune disease[1, 4]
9. Past Medical History
- Multiple sclerosis — most important associated condition[1]
- Prior dental procedures — may have caused post-traumatic trigeminal neuropathy mimicking TN[1]
- Facial trauma or maxillofacial surgery[1]
- Hypertension — associated with TN and relevant to neurovascular compression[2]
- Previous TN episodes — natural history includes remissions and relapses; prior medication trials and responses
- Autoimmune conditions (SLE, scleroderma) — can cause trigeminal neuropathy[1][13]
10. Physical Exam
- Between attacks, exam is typically normal — this is characteristic of TN[2]
- Focused cranial nerve exam: Test all three trigeminal divisions for light touch, pinprick, and temperature; test corneal reflex; assess masseter/temporalis strength
- Trigger zone testing: Light touch to perioral/perinasal area may reproduce pain (be cautious — can provoke severe paroxysm)
- Facial sensation: Any numbness or hypoesthesia is a red flag for secondary TN[2-3]
- Other cranial nerves: Assess hearing (CN VIII — relevant for cerebellopontine angle pathology), facial symmetry (CN VII)
- Fundoscopic exam if concern for intracranial pathology
- Vital signs: Generally normal; tachycardia/hypertension may be present during acute pain crisis
- Oral exam: Rule out dental pathology, mucosal lesions
11. Lab Studies
- Blood tests are not recommended to diagnose TN[2]
- Pre-carbamazepine labs: CBC (risk of aplastic anemia/agranulocytosis), CMP (hepatic function, sodium baseline), HLA-B</em>15:02 in at-risk populations[9-10]
- Monitoring on carbamazepine: Periodic CBC, hepatic function, sodium levels[8]
- If secondary TN suspected: ESR/CRP (giant cell arteritis), ANA (autoimmune), consider LP if MS suspected
- Serum drug levels of carbamazepine are not routinely needed for efficacy monitoring (unlike epilepsy)[3]
12. Imaging
- Brain MRI with and without contrast is recommended for all patients with suspected TN to rule out MS, tumor, cerebral aneurysm, and AVM[2][6]
- 3D time-of-flight MRA identifies neurovascular compression with 95% sensitivity, 77% specificity[2]
- High-resolution sequences (3D CISS, 3D FIESTA, 3D FLASH) improve visualization of neurovascular conflict; 3.0T preferred over 1.5T[3][6][16]
- MRI findings in classic TN: neurovascular contact with morphological changes (displacement, indentation, atrophy) of the trigeminal nerve root[3]
- Demonstration of neurovascular contact should NOT confirm the diagnosis — it facilitates surgical decision-making[3]
- If MRI is contraindicated: CT with contrast to rule out tumors[6]
- Imaging is unnecessary to confirm the clinical diagnosis when presentation is classic, but is needed to exclude secondary causes[6]
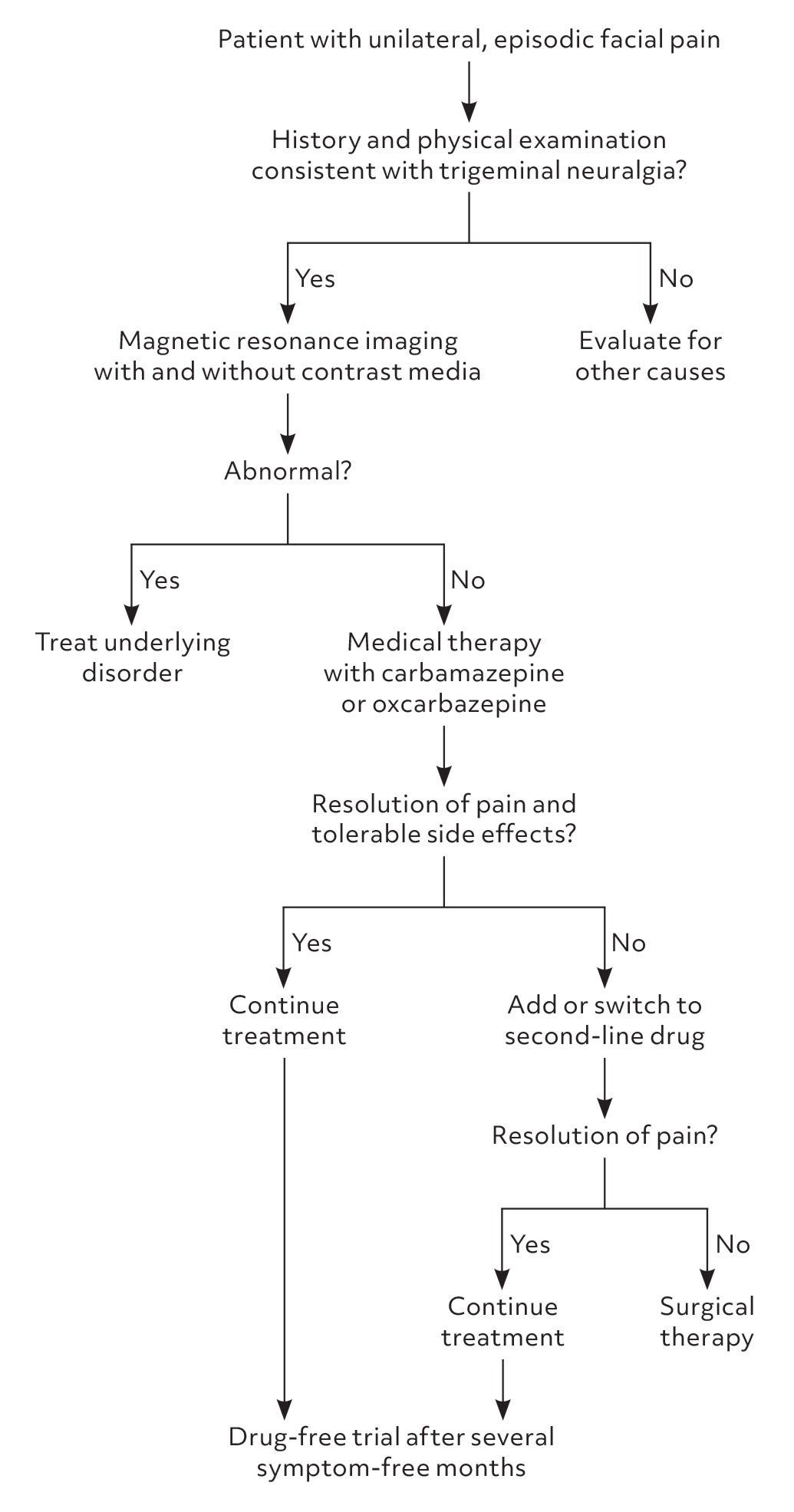
- The following figure outlines the AAFP's recommended diagnostic and treatment algorithm:
- View full figure Figure 2. Diagnosis and treatment of trigeminal neuralgia. Adapted with permission from Krafft RM. Trigeminal neuralgia. Am Fam Physician. 2008;77(9):1295. Trigeminal Neuralgia: Rapid Evidence Review. Am Fam Physician. April 30, 2025.
13. Special Tests
- Electrophysiologic trigeminal nerve reflex testing: Distinguishes classic from secondary TN with sensitivity 96%, specificity 93% (LR+ 14, LR− 0.04); useful when MRI is contraindicated or atypical features are present[2][17]
- Quantitative sensory testing (QST): Can detect subclinical sensory abnormalities; primarily a research tool[3]
- Diffusion tensor imaging (DTI): Emerging modality showing microstructural changes in the trigeminal nerve; not yet standard clinical practice[3][16]
14. ECG
- Pre-treatment ECG is recommended before starting carbamazepine — contraindicated in patients with AV block or other cardiac conduction abnormalities[1][8]
- Carbamazepine has mild anticholinergic activity and sodium-channel blocking properties that can worsen conduction defects[8]
- ECG is not part of the diagnostic workup for TN itself
15. Assessment
- Clinical summary: TN is a clinical diagnosis based on ICHD-3 criteria — recurrent unilateral paroxysmal facial pain in trigeminal distribution, lasting <2 minutes, electric shock–like quality, triggered by innocuous stimuli.[1][3] Triggered paroxysmal pain is reported by 91–99% of patients and may be pathognomonic.[1]
Classification
- Classic TN: Neurovascular compression with morphological nerve changes on MRI (~75%)
- Secondary TN: MS, tumor, AVM (~15%) — younger patients, more likely to have sensory loss and bilateral pain[1]
- Idiopathic TN: No identifiable cause (~10%)[1]
- Subclassification: Purely paroxysmal vs. with concomitant continuous pain[3]
- Complications: Depression, anxiety, weight loss, dehydration, social isolation, medication side effects, suicidality[2][11]
16. Treatment Plan
Initial stabilization (ED)
- Avoid opioids — ineffective and associated with need for additional drugs in 72% of cases[3][7]
- IV fosphenytoin achieved satisfactory relief in 64% of ED cases in one series[7]
- IV lidocaine — effective per clinical experience; requires monitored setting[3]
- Lidocaine injection into trigger zones for short-term relief[3]
- IV fluids if dehydrated from inability to eat/drink[3]
Outpatient pharmacotherapy
- Carbamazepine 200 mg BID, titrate by 200 mg/day every several days to effect (max 1,200 mg/day)[1-2]
- If intolerant: oxcarbazepine 300–1,800 mg/day[1][6]
- Patients should be encouraged to self-adjust doses based on pain severity and side effects, as remission periods occur[3][6]
- Second-line add-on: lamotrigine, gabapentin, pregabalin, baclofen, botulinum toxin type A[6]
Surgical options (for medically refractory TN)
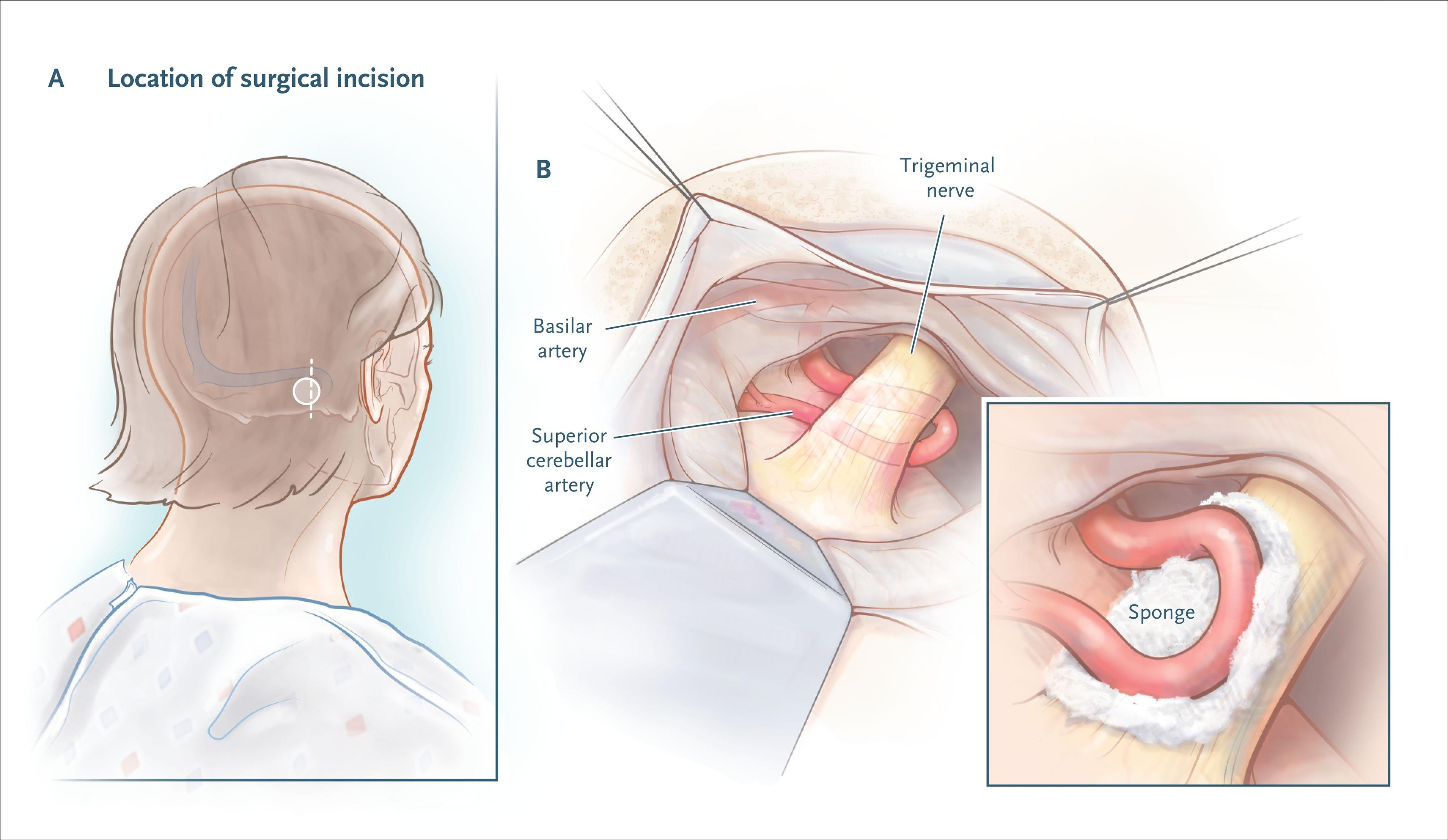
- Microvascular decompression (MVD) — first-line surgery for classic TN; 62–89% pain-free at 3–11 years; mortality 0.3%. A 5-year prospective study showed 59% of MVD patients were pain-free without medication vs. 19% with medical management alone[1][3][18]
- Percutaneous procedures (radiofrequency thermocoagulation, balloon compression, glycerol injection) — ablative; preferred when MRI shows no neurovascular contact[3]
- Gamma knife radiosurgery — non-invasive but destructive; 30–66% pain-free at 4–11 years[3]
- The following figure illustrates the microvascular decompression procedure:
17. Disposition
Admission criteria
- Severe exacerbation with inability to eat or drink (dehydration risk)[3]
- Need for IV fosphenytoin or lidocaine infusion (requires monitored setting)[3]
- Acute titration of antiepileptic drugs in refractory cases[3]
- New neurologic deficits suggesting secondary cause requiring urgent workup
Discharge criteria
- Pain adequately controlled with oral medications
- Able to tolerate oral intake
- Outpatient follow-up arranged
- MRI ordered or scheduled
Specialist consultation triggers
- Neurology: All new diagnoses (for confirmation, MRI interpretation, and classification)[6]
- Neurosurgery: Refractory to ≥2 adequate medication trials, intolerable side effects, or patient preference for surgical evaluation[3][6]
- Dentistry/oral surgery: If dental pathology cannot be excluded
- Ophthalmology: If V1 involvement with corneal reflex concerns
18. Follow Up / Return Precautions
Follow-up timing
- Within 1–2 weeks of starting carbamazepine to assess response, side effects, and check labs (CBC, CMP, sodium)[2][8]
- MRI brain with and without contrast should be obtained in all patients[2]
- After several symptom-free months, consider a gradual drug-free trial (taper slowly over days)[2][6]
- Return precautions — advise patients to seek immediate care for:
- Skin rash (risk of SJS/TEN — stop carbamazepine immediately)[9-10]
- Inability to eat or drink due to pain
- New numbness, weakness, vision changes, or other neurologic symptoms
- Dizziness, unsteadiness, or confusion (medication toxicity)
- Fever, sore throat, mouth ulcers (signs of agranulocytosis)
Patient counseling
- TN is a chronic condition with natural remissions and relapses[2-3]
- Medication doses can be self-adjusted within prescribed range based on pain severity[3][6]
- 80% of patients initially seek dental care — reassure that this is a neurologic condition[2]
- Psychological support should be offered given the significant impact on quality of life[6]
- Expected recovery: ~75% achieve initial pain control with medication; carbamazepine efficacy may wane over years, and surgical options exist for refractory cases[2]
References
1. Trigeminal Neuralgia. — Cruccu G, Di Stefano G, Truini A. The New England Journal of Medicine. 2020.
2. Trigeminal Neuralgia: Rapid Evidence Review. — Amaechi O. American Family Physician. 2025.
3. Advances in Diagnosis, Classification, Pathophysiology, and Management of Trigeminal Neuralgia. — Bendtsen L, Zakrzewska JM, Heinskou TB, et al. The Lancet. Neurology. 2020.
4. Clinical Reasoning: A Misdiagnosis of Atypical Trigeminal Neuralgia. — Duvall JR, Robertson CE. Neurology. 2019.
5. Practice Parameter: The Diagnostic Evaluation and Treatment of Trigeminal Neuralgia (An Evidence-Based Review): Report of the Quality Standards Subcommittee of the American Academy of Neurology and the European Federation of Neurological Societies. — Gronseth G, Cruccu G, Alksne J, et al. Neurology. 2008.
6. European Academy of Neurology Guideline on Trigeminal Neuralgia. — Bendtsen L, Zakrzewska JM, Abbott J, et al. European Journal of Neurology. 2019.
7. Treatment of Acute Exacerbations of Trigeminal Neuralgia in the Emergency Department: A Retrospective Case Series. — Pinto MJ, Gomes A, Pinto M, Abreu P, Costa A. Headache. 2022.
8. FDA Drug Label. — Updated date: 2025-10-23. Food and Drug Administration.
9. FDA Drug Label. — Updated date: 2025-12-09. Food and Drug Administration.
10. FDA Drug Label. — Updated date: 2025-12-16. Food and Drug Administration.
11. Trigeminal Neuralgia. — Ashina S, Robertson CE, Srikiatkhachorn A, et al. Nature Reviews. Disease Primers. 2024.
12. Trigeminal Neuralgia in Multiple Sclerosis: Prevalence and Association With Demyelination. — Laakso SM, Hekali O, Kurdo G, et al. Acta Neurologica Scandinavica. 2020.
13. Identifying Associated Comorbidities in the Development of Trigeminal Neuralgia: A Propensity-Matched Analysis of the National Inpatient Sample. — Tang M, Devarajan A, Huo L, et al. Clinical Neurology and Neurosurgery. 2025.
14. Chronic Facial Pain: Trigeminal Neuralgia, Persistent Idiopathic Facial Pain, and Myofascial Pain Syndrome-an Evidence-Based Narrative Review and Etiological Hypothesis. — Gerwin R. International Journal of Environmental Research and Public Health. 2020.
15. Differential Diagnosis of Facial Pain and Guidelines for Management. — Zakrzewska JM. British Journal of Anaesthesia. 2013.
16. Magnetic Resonance Imaging in the Diagnosis of Trigeminal Neuralgia: A Systematic Review of the Imaging Protocol and Diagnostic Accuracy. — Henssen D, van Grinsven M, Vissers K, van Goethem J. European Radiology. 2026.
17. Trigeminal Neuralgia: New Classification and Diagnostic Grading for Practice and Research. — Cruccu G, Finnerup NB, Jensen TS, et al. Neurology. 2016.
18. Five-Year Prospective Outcomes of Medical Management and Microvascular Decompression in Trigeminal Neuralgia. — Worm J, Heinskou TB, Rochat P, et al. Journal of Neurology. 2025.