Tularemia (Pneumonic)
Pneumonic tularemia is a rare but potentially life-threatening form of tularemia caused by Francisella tularensis, typically acquired through inhalation of contaminated aerosols or secondary to hem…
Pneumonic tularemia is a rare but potentially life-threatening form of tularemia caused by Francisella tularensis, typically acquired through inhalation of contaminated aerosols or secondary to hematogenous spread.[1-2] This form has the highest mortality rate (up to 60% if untreated) and requires prompt recognition and treatment.[2]
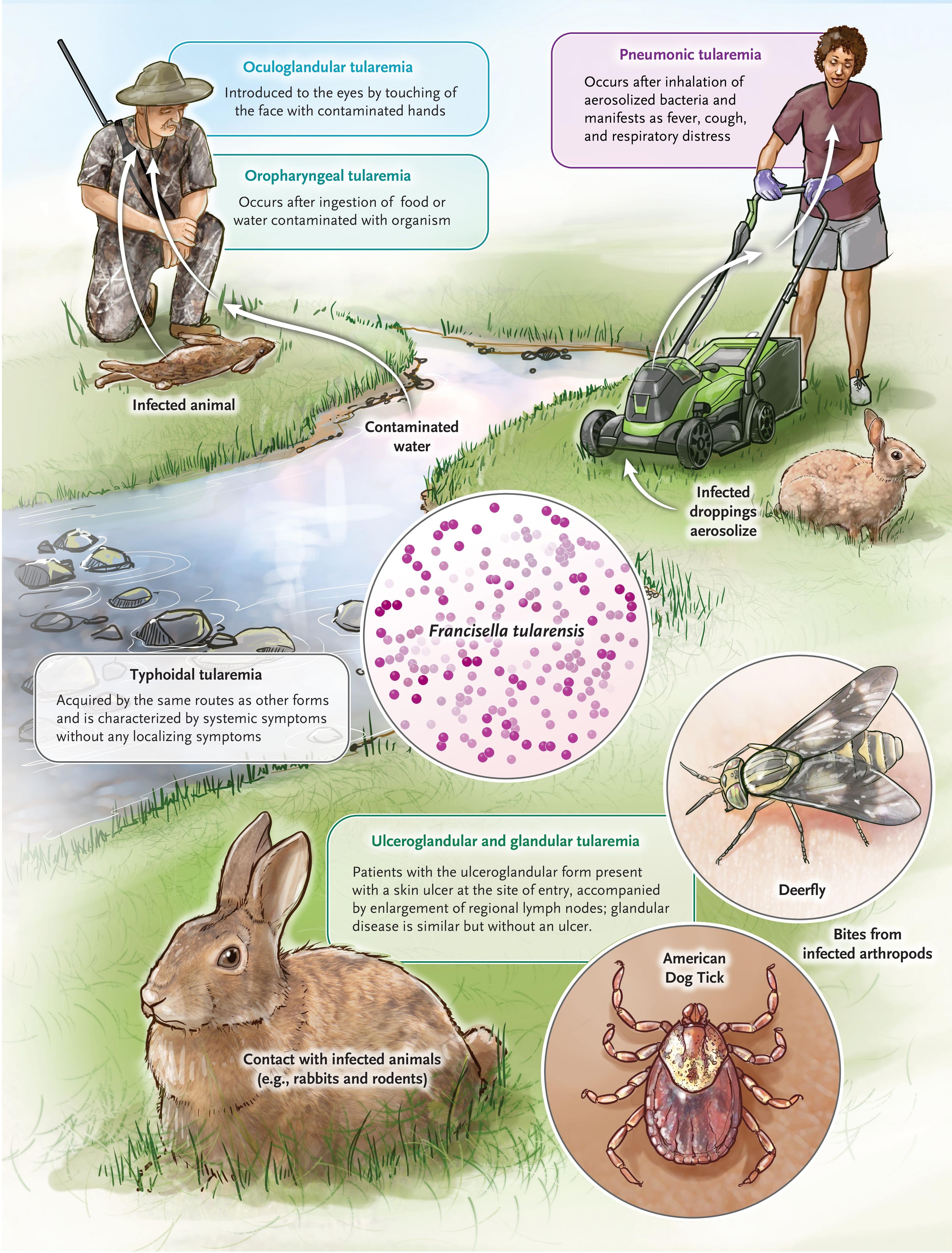
The following figure illustrates the various transmission routes and clinical manifestations of tularemia:
View full figure Figure 1. Tularemia — Modes of Acquisition and Manifestations. Going Down the Rabbit Hole. N Engl J Med. July 31, 2024.
1. History
Key HPI questions
- • Onset and duration of symptoms (typically 3-5 days incubation, range 1-14 days)[4]
- • Fever pattern and severity (38.0-41.5°C)[4]
- • Respiratory symptoms: cough (often with scant sputum), chest pain, dyspnea[1][5]
- • Constitutional symptoms: fatigue, headache, myalgias, malaise[1][4]
Symptom characterization
- • Fever is typically high-grade and acute in onset[4]
- • Cough is usually nonproductive or with minimal sputum[6]
- • Chest pain may be pleuritic[5]
Timing, triggers, severity, progression
- • Symptoms develop 1-14 days after exposure (average 3-5 days)[4]
- • Can progress rapidly to severe pneumonia and respiratory failure[7]
- • May present initially as systemic illness without prominent respiratory signs[7]
Associated symptoms
- • Headache, myalgias, malaise, chills[4]
- • Abdominal pain, nausea, vomiting (especially in typhoidal form)[7]
- • Pharyngitis may be present[4]
Important negatives
- • Absence of skin ulcers or lymphadenopathy (distinguishes from ulceroglandular form)[7]
- • No conjunctival involvement[7]
2. Alarm Features
Red flag symptoms/signs
- • High fever with rapid clinical deterioration[2]
- • Respiratory distress or failure[7]
- • Septic shock presentation[4]
- • Altered mental status[7]
Features suggesting life-threatening pathology
- • Pneumonic and typhoidal forms have highest mortality[2]
- • Rapid progression to severe pneumonia[7]
- • Signs of sepsis or multi-organ failure[7]
Indications for urgent escalation
- • Respiratory distress requiring oxygen support
- • Hemodynamic instability
- • Suspected bioterrorism exposure (requires immediate public health notification)[8]
3. Medications
Relevant medication contributors
- • Beta-lactam antibiotics are ineffective and should be avoided[9-10]
- • Anti-TNF agents increase risk of severe infection[6]
- • Immunosuppressive medications increase severity risk[6]
Common treatments
- • First-line for severe disease: Gentamicin 1.5 mg/kg IV q8h or streptomycin 15 mg/kg IM q12h[11]
- • First-line for mild-moderate disease: Ciprofloxacin 750 mg PO BID or levofloxacin 500 mg PO daily[8][11]
- • Alternative: Doxycycline 100 mg PO BID[11]
Contraindicated medications
- • Beta-lactam antibiotics (penicillins, cephalosporins)[9-10]
- • Most macrolides (except azithromycin in specific European strains)[10]
Medication interactions or cautions
- • Fluoroquinolones: avoid in pregnancy and young children due to musculoskeletal concerns[10]
- • Aminoglycosides: monitor renal function and hearing[11]
4. Diet
Dietary triggers or recommendations
- • No specific dietary restrictions during acute illness
- • Maintain adequate nutrition during prolonged illness
Hydration considerations
- • Ensure adequate hydration, especially with fever
- • Monitor fluid balance in severe cases
5. Review of Systems
Important ROS questions
- • Respiratory: cough, dyspnea, chest pain, hemoptysis
- • Constitutional: fever, chills, night sweats, weight loss
- • GI: abdominal pain, nausea, vomiting, diarrhea
- • Neurologic: headache, altered mental status
- • Skin: rash, ulcers, lymphadenopathy
High-yield associated systems
6. Collateral History and Family History
Important collateral information
- • Recent outdoor activities in endemic areas[1][5]
- • Animal exposure (rabbits, rodents, cats)[13]
- • Tick bites or arthropod exposure[5]
- • Travel to rural areas[1][5]
- • Occupational exposure (veterinarians, hunters, laboratory workers)
Relevant hereditary conditions
- • Immunodeficiency syndromes
- • Family history of unusual infections
Social context
- • Rural residence or activities[1][5]
- • Hunting, trapping, or animal handling[13]
- • Laboratory work with potential F. tularensis exposure
7. Risk Factors
Major epidemiologic risk factors
- • Rural residence or outdoor activities[1][5]
- • Contact with rabbits, rodents, or other small mammals[13]
- • Tick or deerfly bites[5]
- • Drinking untreated water[3]
- • Laboratory exposure[8]
Lifestyle contributors
- • Hunting, trapping, skinning animals[13]
- • Gardening, lawn mowing in endemic areas[3]
- • Camping in endemic areas
Comorbidities increasing risk
- • Immunosuppression (including anti-TNF therapy)[6]
- • Advanced age[12]
- • Chronic medical conditions[12]
8. Differential Diagnosis
Most important alternative diagnoses
- • Community-acquired pneumonia (bacterial, viral, atypical)
- • Tuberculosis[10]
- • Lung cancer or lymphoma[1]
- • Sarcoidosis[6]
- • Histoplasmosis or other endemic mycoses
Dangerous cannot-miss diagnoses
- • Pneumonic plague
- • Anthrax (inhalational)
- • Severe acute respiratory syndrome
- • Pneumonic tularemia in bioterrorism context[8]
Mimics and distinguishing features
- • vs. Tuberculosis: Tularemia has more acute onset, less cavitation[10]
- • vs. Lung cancer: Tularemia has fever, acute onset, exposure history[1]
- • vs. CAP: Tularemia often has mediastinal lymphadenopathy[1][12]
9. Past Medical History
Relevant prior conditions
- • Previous tularemia infection (provides some immunity)
- • Immunocompromising conditions
- • Chronic lung disease
Previous episodes
- • Prior tick-borne illnesses
- • Previous pneumonias
Surgical history
- • Thoracic procedures
- • Immunosuppressive procedures
Chronic illnesses impacting management
- • Renal disease (affects antibiotic dosing)[11]
- • Liver disease
- • Heart failure
10. Physical Exam
Key exam findings
- • Fever (often high-grade 38-41.5°C)[4]
- • Tachypnea, tachycardia
- • Pulmonary findings may be minimal early in disease[7]
Vital sign abnormalities
Focused exam maneuvers
- • Complete pulmonary examination
- • Lymph node examination (cervical, axillary, inguinal)
- • Skin examination for ulcers or rashes
- • Oropharyngeal examination
Expected vs concerning findings
- • Expected: Fever, mild respiratory findings initially[7]
- • Concerning: Respiratory distress, altered mental status, hypotension[7]
11. Lab Studies
Recommended labs
- • Complete blood count (usually normal or slightly elevated WBC)[4]
- • Comprehensive metabolic panel
- • Liver function tests (often elevated transaminases)[4]
- • Blood cultures (low sensitivity ~10%)[6]
- • Respiratory cultures if productive sputum
Expected abnormalities
- • Normal or slightly elevated WBC with normal differential[4]
- • Elevated hepatic transaminases[4]
- • Elevated inflammatory markers (ESR, CRP)
Labs used to rule out dangerous conditions
- • Blood cultures to rule out other bacterial pneumonia
- • Sputum cultures and stains
- • Procalcitonin may be elevated
Monitoring parameters
- • Renal function (if using aminoglycosides)[11]
- • Liver function
- • Complete blood count
12. Imaging
First-line imaging
Gold standard imaging
- • Chest CT: consistently shows mediastinal lymphadenopathy and pulmonary nodules[1]
- • May show subpleural micronodules or pleural effusion[1]
- • Subpleural round consolidations are characteristic[12]
Important imaging findings
- • Mediastinal lymphadenopathy (very common)[1][12]
- • Pulmonary nodules or consolidations[1]
- • Pleural effusions[1][12]
- • May mimic malignancy on PET scan[1]
When imaging is unnecessary
- • Chest imaging is essential for suspected pneumonic tularemia
13. Special Tests
Diagnostic scoring systems
- • No specific scoring systems available
Point-of-care tests
- • None available
Procedures or specialty tests
- • Bronchoscopy with EBUS-TBNA may be performed[5]
- • CT-guided biopsy (shows necrotizing granulomatous inflammation)[1][5]
14. ECG
ECG findings
- • Generally not specific for tularemia
- • May show sinus tachycardia
Indications for ECG
- • Severe illness with hemodynamic compromise
- • Elderly patients or those with cardiac risk factors
15. Assessment
Clinical summary
- • Pneumonic tularemia is a rare but serious form of tularemia with high mortality if untreated[2]
- • Often presents with nonspecific symptoms initially[1]
- • Imaging typically shows mediastinal lymphadenopathy and pulmonary nodules[1][12]
Severity stratification
- • Mild-moderate: Stable vital signs, minimal respiratory distress
- • Severe: Respiratory distress, hemodynamic instability, sepsis[2]
Typical vs atypical presentations
- • Typical: Acute febrile illness with respiratory symptoms and exposure history
- • Atypical: May present as systemic illness without prominent respiratory signs[7]
Complications to consider
16. Treatment Plan
Initial stabilization
- • Supportive care for respiratory distress
- • Fluid resuscitation if hypotensive
- • Oxygen support as needed
Medications and dosing
- • Severe disease: Gentamicin 1.5 mg/kg IV q8h or streptomycin 15 mg/kg IM q12h[11]
- • Mild-moderate disease: Ciprofloxacin 750 mg PO BID or levofloxacin 500 mg PO daily[8][11]
- • Alternative: Doxycycline 100 mg PO BID[11]
- • Duration: 10-14 days for severe cases, 14-21 days for mild-moderate[9][11]
Outpatient vs inpatient treatment
- • Inpatient: Severe disease, respiratory distress, hemodynamic instability
- • Outpatient: Mild disease with reliable follow-up
Follow-up management
- • Monitor for treatment response
- • Watch for complications or relapse[9]
17. Disposition
Admission criteria
- • Severe pneumonia or respiratory distress
- • Hemodynamic instability
- • Inability to tolerate oral medications
- • Concern for complications
Discharge criteria
- • Stable vital signs
- • Tolerating oral medications
- • Reliable follow-up available
- • No signs of complications
Observation indications
- • Borderline cases with mild respiratory symptoms
- • Elderly patients or those with comorbidities
Specialist consultation triggers
- • Infectious disease consultation for severe cases
- • Pulmonology if respiratory failure
- • ICU consultation for septic shock
18. Follow Up / Return Precautions
Follow-up timing
- • 48-72 hours for outpatients to assess response
- • Weekly follow-up until resolution
Symptoms requiring immediate reassessment
- • Worsening respiratory distress
- • High fever despite treatment
- • Signs of sepsis or shock
- • Inability to tolerate medications
Patient counseling points
- • Complete full antibiotic course[9]
- • Expect gradual improvement over days to weeks
- • Avoid beta-lactam antibiotics[9-10]
- • Report worsening symptoms immediately
Expected recovery course
- • Fever typically resolves within 24-115 hours depending on severity[12]
- • Complete recovery may take weeks
- • Relapse rates 5-15% depending on antibiotic choice[10]
References
1. Pulmonary Tularemia: A Diagnosis Not to Overlook. — Zaghdoudi A, Robin F, Moulinie J, et al. International Journal of Infectious Diseases : IJID : Official Publication of the International Society for Infectious Diseases. 2026.
2. Tularemia for Clinicians: An Up-to-Date Review on Epidemiology, Diagnosis, Prevention and Treatment. — Antonello RM, Giacomelli A, Riccardi N. European Journal of Internal Medicine. 2025.
3. Going Down the Rabbit Hole. — Burdick KJ, Ealick W, Vargas Acevedo H, Sectish TC, Sandora TJ. The New England Journal of Medicine. 2024.
4. Tick-Borne Diseases in the United States. — Spach DH, Liles WC, Campbell GL, et al. The New England Journal of Medicine. 1993.
5. Thoracic Manifestations of Tularaemia: A Case Series. — Vacca M, Wilhelms B, Zange S, et al. Infection. 2024.
6. Pulmonary tularaemia in a female adolescent with inflammatory bowel disease receiving infliximab: Do not miss the diagnosis. — Schwarzová V, Schwarz J, Mitrová K, et al. Pediatric Pulmonology. 2023.
7. Tularemia as a Biological Weapon: Medical and Public Health Management. — Dennis DT, Inglesby TV, Henderson DA, et al. The Journal of the American Medical Association. 2001.
8. Tularemia Antimicrobial Treatment and Prophylaxis: CDC Recommendations for Naturally Acquired Infections and Bioterrorism Response - United States, 2025. — Nelson CA, Meaney-Delman D, Fleck-Derderian S, Winberg J, Mead PS. MMWR. Recommendations and Reports : Morbidity and Mortality Weekly Report. Recommendations and Reports. 2025.
9. Tularemia Treatment: Experimental and Clinical Data. — Maurin M, Pondérand L, Hennebique A, et al. Frontiers in Microbiology. 2023.
10. Tularaemia: Clinical Aspects in Europe. — Maurin M, Gyuranecz M. The Lancet. Infectious Diseases. 2016.
11. Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. — Stevens DL, Bisno AL, Chambers HF, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2014.
12. Treatment Outcome of Severe Respiratory Type B Tularemia Using Fluoroquinolones. — Widerström M, Mörtberg S, Magnusson M, Fjällström P, Johansson AF. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
13. Hunting for Tularaemia - A Review of Cases in North Carolina. — Rimawi RH, Shah KB, Chowdhary RA, Cook PP. Zoonoses and Public Health. 2015.