Tularemia (Ulceroglandular)
Ulceroglandular tularemia is the most common clinical form of tularemia, caused by the gram-negative intracellular coccobacillus Francisella tularensis. It is characterized by a cutaneous ulcer at…
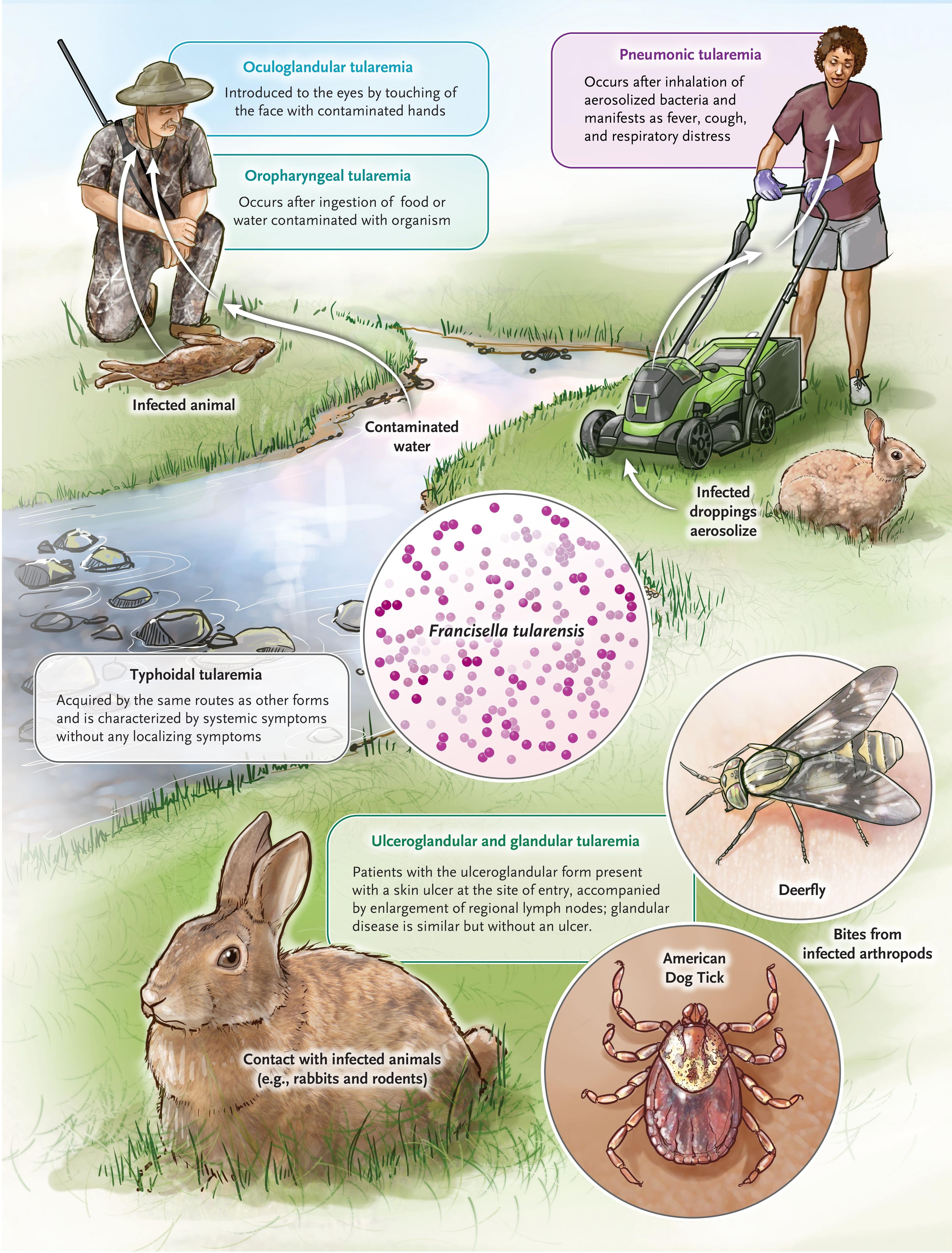
Ulceroglandular tularemia is the most common clinical form of tularemia, caused by the gram-negative intracellular coccobacillus Francisella tularensis. It is characterized by a cutaneous ulcer at the inoculation site with painful regional lymphadenopathy, typically following a tick bite or direct contact with infected animals.[1-3] It is a CDC Category A bioterrorism agent due to its extremely low infectious dose (~10 organisms) and ease of aerosolization.[4-5]
The following figure illustrates the various modes of acquisition and their corresponding clinical syndromes:
View full figure Figure 1. Tularemia — Modes of Acquisition and Manifestations. Going Down the Rabbit Hole. N Engl J Med. July 31, 2024.
1. History
- Exposure history is paramount: Ask about tick bites (most common US vector, ~69% of cases), handling rabbits/hares/rodents, skinning or butchering wild game, cat bites/scratches, deer fly bites, mowing over animal carcasses, and contaminated water exposure[2][5][7]
- Incubation period: Typically 3–5 days (range 1–21 days)[1][8-9]
- Symptom characterization: Abrupt onset of fever (38–40°C), chills, headache, malaise, myalgia, and anorexia, followed by development of a skin lesion at the inoculation site and painful swollen lymph nodes[1-2][5]
- Timing: Patients seek care after a median of 3 days of illness[7]
- Important negatives: No person-to-person transmission; no respiratory symptoms (distinguishes from pneumonic form); no pharyngitis (distinguishes from oropharyngeal form)[2][5]
2. Alarm Features
- High fever with systemic toxicity (rigors, prostration, confusion) — suggests progression to typhoidal or septic tularemia[5]
- Respiratory symptoms (cough, dyspnea, pleuritic pain) — any form can develop secondary pneumonia via hematogenous spread[5][9]
- Pulse-temperature dissociation — noted in up to 42% of patients; should raise suspicion[5][10]
- Suppurative lymphadenopathy with fluctuance — occurs in ~30% and may require surgical drainage[9][11]
- Immunocompromised patients — at risk for severe, atypical, and disseminated disease[2][12]
- Delayed treatment >2–3 weeks from onset — associated with higher treatment failure and relapse rates[11]
3. Medications
Effective treatments
Mild-moderate disease (outpatient)
- Ciprofloxacin 500–750 mg PO BID × 10–14 days[1][13-14]
- Levofloxacin 500 mg PO daily × 10–14 days[1]
- Doxycycline 100 mg PO BID × 14–21 days (higher relapse rate with shorter courses)[1][13]
Severe disease (inpatient)
- Gentamicin 5 mg/kg/day IV (or 1.5 mg/kg q8h) — first-line for severe tularemia[1][4]
- Streptomycin 15 mg/kg IM q12h (max 2 g/day) — historical gold standard[1][15]
- Step-down: Parenteral aminoglycoside until clinical improvement, then oral fluoroquinolone or doxycycline to complete 10–14 days[1]
Contraindicated/ineffective
- Beta-lactams — F. tularensis is intrinsically resistant; empiric use is a common cause of treatment failure[1][11]
- Most macrolides — generally ineffective[11]
- Anti-tuberculosis agents — ineffective[11]
Cautions
- Doxycycline and tetracyclines are bacteriostatic → higher relapse rates, especially with courses <7–10 days[1]
- Aminoglycosides require renal dose adjustment and monitoring[1]
- The 2025 CDC guidelines now designate fluoroquinolones and doxycycline as first-line for outbreaks of any size[13]
4. Diet
- No specific dietary triggers or restrictions
- Ensure adequate hydration, especially in febrile patients with systemic symptoms
- Avoid consumption of untreated water from natural sources in endemic areas (potential transmission route)[2][5]
- Ensure thorough cooking of wild game meat
5. Review of Systems
- Constitutional: Fever, chills, rigors, night sweats, weight loss, fatigue, anorexia[2][5]
- Skin: Ulcer or eschar at bite/contact site; erythema nodosum or erythema multiforme (rare)[8-9]
- Lymphatic: Painful regional lymphadenopathy (inguinal/femoral for lower extremity bites; axillary for upper extremity; cervical for head/neck)[3][10]
- Respiratory: Cough, dyspnea, pleuritic chest pain (screen for secondary pneumonia)[5]
- GI: Nausea, vomiting, diarrhea, abdominal pain[2][5]
- Musculoskeletal: Myalgia, arthralgia, low back pain[5][9]
- Neurologic: Headache; confusion/stupor in severe typhoidal forms[9]
- Ophthalmologic: Photophobia, conjunctivitis (if oculoglandular form suspected)[2]
6. Collateral History and Family History
- Occupational exposure: Hunting, trapping, butchering, farming, landscaping/mowing, veterinary work, laboratory work[5][16]
- Recreational exposure: Hiking, camping, outdoor activities in endemic areas during summer months[7][16]
- Animal contact: Recent contact with rabbits, hares, rodents, or domestic cats; dead animal sightings near home[2][5]
- Geographic context: Residence or travel to endemic areas (Arkansas, Missouri, Oklahoma, South Dakota, Montana; Scandinavia, former Soviet Union)[5][17]
- Household contacts: No person-to-person transmission, but shared environmental exposures may indicate cluster/outbreak[5]
- Family history is generally not relevant (no hereditary predisposition)
7. Risk Factors
- Tick exposure — most common US vector (~69% of cases); peak incidence in summer months[7][16]
- Direct animal contact — handling infected rabbits, hares, rodents, or their carcasses[2][5]
- Male sex — 65% of cases; reflects occupational/recreational exposure patterns[7][17]
- Age bimodal distribution — highest incidence in children aged 5–9 years and men >55 years[17]
- Rural residence in endemic states[5]
- Occupational risk: Hunters, trappers, farmers, landscapers, laboratory workers[5]
- Immunocompromised status — anti-TNF-α therapy, other immunosuppression → risk of severe/disseminated disease[12]
- Cat bites/scratches — increasingly recognized transmission route[1][18]
8. Differential Diagnosis
Cannot-miss diagnoses
- Plague (bubonic) — similar ulcer + lymphadenopathy; more rapid progression, higher mortality; exposure to rodent fleas
- Anthrax (cutaneous) — painless black eschar with surrounding edema; no significant lymphadenopathy initially
- Necrotizing soft tissue infection — rapidly progressive; systemic toxicity disproportionate to local findings
Most important alternatives
- Cat scratch disease (Bartonella henselae) — lymphadenopathy with cat exposure; typically less systemic toxicity; no ulcer at inoculation site[19]
- Sporotrichosis — nodular lymphangitis pattern; gardening/soil exposure; chronic course
- Staphylococcal/streptococcal lymphadenitis — responds to beta-lactams (tularemia does not)
- Tuberculosis — chronic lymphadenopathy with caseating granulomas; tularemia can mimic TB histologically[20]
- Lymphoma — painless lymphadenopathy; B symptoms; tularemia lymphadenopathy can mimic malignancy on PET/CT[20-21]
- Other tick-borne diseases — RMSF, ehrlichiosis, Lyme disease (different rash patterns, different lymph node involvement)[3]
- Mycobacterium marinum — if water exposure; chronic granulomatous skin lesion
- Key distinguishing feature: Failure to respond to beta-lactam antibiotics in a patient with ulcer + lymphadenopathy should raise strong suspicion for tularemia[11][22]
9. Past Medical History
- Immunosuppression — HIV, organ transplant, anti-TNF-α therapy, chemotherapy → increased risk of severe/disseminated disease[2][12]
- Prior tularemia — cellular immunity is long-lasting; reinfection tends to be localized[10]
- Chronic kidney disease — impacts aminoglycoside dosing[1]
- Prior tick-borne illness — suggests ongoing arthropod exposure risk
- Splenectomy — increased susceptibility to encapsulated and intracellular organisms
10. Physical Exam
Vital signs
- Fever 38–40°C (often high-grade)[5]
- Pulse-temperature dissociation (relative bradycardia) in up to 42%[5][10]
- Tachycardia if septic; hypotension in severe cases
Focused exam
- Skin: Tender papule → pustule → punched-out ulcer with raised borders and necrotic base (eschar) at inoculation site; typically on lower extremities (tick bite), upper extremities (animal handling), or trunk[1][3]
- Lymph nodes: Tender, enlarged regional lymphadenopathy — inguinal/femoral (lower extremity inoculation), axillary (upper extremity), cervical (head/neck); may be fluctuant if suppurated[1][3][9]
- Lungs: Usually clear in ulceroglandular form; crackles or decreased breath sounds if secondary pneumonia develops[5]
- Abdomen: Hepatosplenomegaly possible in systemic disease[10]
- Skin rashes: Erythema nodosum, erythema multiforme (uncommon complications)[8-9]
11. Lab Studies
Recommended
- Tularemia serology (microagglutination test) — preferred diagnostic method; seroconversion or 4-fold rise in paired sera is confirmatory; single titer ≥1:128 is presumptive[1][9]
- Antibodies typically detectable 1–2 weeks after symptom onset; peak at 3–4 weeks[9]
- PCR for F. tularensis — from ulcer swab, lymph node aspirate, or biopsy; rapid and highly sensitive/specific[9][12]
- Blood cultures — low yield (<10%), but should be obtained; must notify lab of tularemia suspicion (biosafety risk)[1][9][15]
- CBC — may show leukocytosis or normal WBC; nonspecific
- CMP — mild hepatitis (elevated transaminases) is common[10]
- CRP/ESR — typically elevated; nonspecific
- Key lab pearl: Routine cultures are often negative unless cysteine-supplemented media are used. Unsuspected growth of F. tularensis poses a serious laboratory-acquired infection risk — always alert the microbiology lab[1][15][19]
12. Imaging
- Ulceroglandular form: Imaging is generally not necessary for straightforward presentations
- Ultrasound of lymph nodes — useful to assess for suppuration/abscess formation requiring drainage[9]
- Chest X-ray — obtain if respiratory symptoms present; findings are nonspecific (infiltrates, hilar lymphadenopathy, pleural effusion)[15][23]
- CT chest — if pneumonic involvement suspected; may show mediastinal lymphadenopathy, pulmonary nodules, pleural effusion[21]
- PET/CT — can show intensely hypermetabolic lymph nodes mimicking lymphoma; avoid unnecessary biopsy if tularemia is in the differential[21]
13. Special Tests
- Tularemia microagglutination test — gold standard serologic method; paired sera 2–4 weeks apart[9]
- PCR (F. tularensis-specific) — from wound swab, lymph node aspirate; faster than serology[9][12]
- Immunofluorescence staining — can be performed on tissue specimens[15]
- Culture on cysteine heart agar with 9% chocolate blood or chocolate agar — growth in 24–48 hours at 37°C; requires BSL-3 precautions[9]
- Lymph node FNA or biopsy — may show necrotizing granulomatous inflammation; can mimic TB (caseating granulomas)[20]
- Point-of-care: No rapid bedside test currently available
14. ECG
- Not routinely indicated for ulceroglandular tularemia
- Cardiovascular complications are very rare but reported: myocarditis, pericarditis (usually with concomitant pneumonia), and extremely rare endocarditis[18][24-25]
- Obtain ECG if: chest pain, dyspnea out of proportion to exam, new arrhythmia, or signs of myocarditis (elevated troponin, new heart failure)
- If myocarditis suspected: look for diffuse ST changes, low voltage, new conduction abnormalities[18]
15. Assessment
- Clinical summary: Ulceroglandular tularemia presents as an acute febrile illness with a skin ulcer at the inoculation site and painful regional lymphadenopathy, typically 3–5 days after tick bite or animal contact. It is the most common form, accounting for ~37–47% of all tularemia cases in the US.[7][22]
Severity stratification
- Mild-moderate: Localized ulcer + lymphadenopathy, low-grade fever, non-toxic appearance → outpatient oral therapy
- Severe: High fever, systemic toxicity, suppurative nodes, immunocompromised host, concern for secondary pneumonia or sepsis → inpatient IV therapy
Typical vs. atypical
- Typical: Ulcer + regional adenopathy + fever after tick/animal exposure
- Atypical: Ulcer may be healed/inconspicuous at presentation ("glandular" form); granulomatous lymphadenitis mimicking TB or lymphoma[1][20]
Complications
- Lymph node suppuration (~30%)[9][11]
- Secondary pneumonia via hematogenous spread[5]
- Sepsis (rare in ulceroglandular form)
- Meningitis, brain abscess (very rare)[9]
- Myocarditis, pericarditis (very rare)[18][25]
- Erythema nodosum, erythema multiforme[8-9]
16. Treatment Plan
Initial stabilization
- IV access, fluid resuscitation, and antipyretics for febrile/toxic patients
- Obtain cultures and serology before starting antibiotics, but do not delay treatment while awaiting results
Mild-moderate ulceroglandular (outpatient)
- Ciprofloxacin 500 mg PO BID × 10–14 days, OR
- Doxycycline 100 mg PO BID × 14–21 days (longer course to reduce relapse)[1][13]
Severe disease (inpatient)
- Gentamicin 5 mg/kg/day IV divided q8h (adjust for renal function), OR
- Streptomycin 1 g IM q12h[1]
- Step down to oral fluoroquinolone or doxycycline once clinically improved; total course 10–14 days[1]
Suppurative lymph nodes
- Incision and drainage or surgical excision may be necessary, especially in patients with delayed treatment[9][11]
Special populations
- Children: Gentamicin 6 mg/kg/day IV divided q8h for severe disease; ciprofloxacin or doxycycline for mild disease[1]
- Pregnancy: Gentamicin preferred for severe disease; ciprofloxacin may be considered for mild disease (risk-benefit discussion)[13]
- Immunocompromised: Lower threshold for aminoglycoside therapy and longer treatment courses[13]
17. Disposition
Admission criteria
- Systemic toxicity, hemodynamic instability, or sepsis
- Pneumonic or typhoidal features
- Inability to tolerate oral medications
- Immunocompromised host with moderate-severe disease
- Need for IV aminoglycoside therapy
- Suppurative lymphadenopathy requiring surgical intervention
- Diagnostic uncertainty with concern for dangerous mimics (plague, anthrax)
Discharge criteria (outpatient management appropriate if)
- Non-toxic appearance, stable vitals
- Localized ulceroglandular disease without systemic complications
- Able to tolerate oral antibiotics
- Reliable follow-up available
- Immunocompetent
Observation
- Consider for borderline cases — moderate fever with early systemic symptoms, pending serology/culture results
Specialist consultation triggers
- Infectious disease — all confirmed/suspected cases (uncommon disease, complex treatment decisions)
- Surgery — suppurative lymph nodes requiring drainage
- Pulmonology — if pneumonic involvement suspected
- Public health notification — tularemia is a nationally notifiable disease; report to local/state health department[16-17]
18. Follow Up / Return Precautions
Follow-up timing
- Recheck in 48–72 hours after initiating antibiotics to assess clinical response
- Repeat serology at 2–4 weeks for paired sera confirmation[9]
- Follow-up at 2 weeks to assess ulcer healing and lymph node regression
Symptoms requiring immediate reassessment
- Worsening fever or new rigors despite 48–72 hours of appropriate antibiotics
- New respiratory symptoms (cough, dyspnea, chest pain) — concern for secondary pneumonia
- Increasing lymph node size, fluctuance, or new drainage — may need I&D
- Altered mental status, neck stiffness — concern for meningitis
- Rash progression (erythema nodosum, erythema multiforme)
Patient counseling
- No person-to-person transmission — standard precautions are sufficient[5][15]
- Ulcer healing may take weeks to months; lymphadenopathy can persist for months[9]
- Relapse is possible, especially with bacteriostatic agents (doxycycline) or short courses — complete the full antibiotic course[1][11]
- Tick prevention: DEET-based repellents, permethrin-treated clothing, daily tick checks, prompt tick removal[2]
- Avoid handling sick/dead wild animals without gloves[5]
Expected recovery
- With appropriate antibiotics, clinical improvement typically occurs within 48–72 hours[7]
- Overall mortality for ulceroglandular form is low (<2% with treatment)[8][14]
- Untreated fatality rate for all forms can reach up to 60%, though ulceroglandular carries the best prognosis among tularemia subtypes[4][10]
References
1. Practice Guidelines for the Diagnosis and Management of Skin and Soft Tissue Infections: 2014 Update by the Infectious Diseases Society of America. — Stevens DL, Bisno AL, Chambers HF, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2014.
2. Tickborne Diseases of the United States: A Reference Manual for Healthcare Providers Sixth Edition. — Nancy Shadick MD MPH, Nancy Maher MPH, Dennis Hoak MD United States Centers for Disease Control and Prevention (2022). 2022.
3. Tick-Borne Diseases in the United States. — Spach DH, Liles WC, Campbell GL, et al. The New England Journal of Medicine. 1993.
4. Tularemia for Clinicians: An Up-to-Date Review on Epidemiology, Diagnosis, Prevention and Treatment. — Antonello RM, Giacomelli A, Riccardi N. European Journal of Internal Medicine. 2025.
5. Tularemia as a Biological Weapon: Medical and Public Health Management. — Dennis DT, Inglesby TV, Henderson DA, et al. The Journal of the American Medical Association. 2001.
6. Going Down the Rabbit Hole. — Burdick KJ, Ealick W, Vargas Acevedo H, Sectish TC, Sandora TJ. The New England Journal of Medicine. 2024.
7. Clinical Recognition and Management of Tularemia in Missouri: A Retrospective Records Review of 121 Cases. — Weber IB, Turabelidze G, Patrick S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2012.
8. Tularemia‐induced erythema multiforme minor in an 11‐year‐old girl. — Coates SJ, Briggs B, Cordoro KM. Pediatric Dermatology. 2018.
9. Tularaemia: Clinical Aspects in Europe. — Maurin M, Gyuranecz M. The Lancet. Infectious Diseases. 2016.
10. Tularemia: A 30-Year Experience With 88 Cases. — Evans ME, Gregory DW, Schaffner W, McGee ZA. Medicine. 1985.
11. Tularemia Treatment: Experimental and Clinical Data. — Maurin M, Pondérand L, Hennebique A, et al. Frontiers in Microbiology. 2023.
12. Pulmonary tularaemia in a female adolescent with inflammatory bowel disease receiving infliximab: Do not miss the diagnosis. — Schwarzová V, Schwarz J, Mitrová K, et al. Pediatric Pulmonology. 2023.
13. Tularemia Antimicrobial Treatment and Prophylaxis: CDC Recommendations for Naturally Acquired Infections and Bioterrorism Response - United States, 2025. — Nelson CA, Meaney-Delman D, Fleck-Derderian S, Winberg J, Mead PS. MMWR. Recommendations and Reports : Morbidity and Mortality Weekly Report. Recommendations and Reports. 2025.
14. Tularemia Clinical Manifestations, Antimicrobial Treatment, and Outcomes: An Analysis of US Surveillance Data, 2006-2021. — Wu HJ, Bostic TD, Horiuchi K, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
15. Clinical Management of Potential Bioterrorism-Related Conditions. — Adalja AA, Toner E, Inglesby TV. The New England Journal of Medicine. 2015.
16. Tularemia - Missouri, 2000-2007. — MMWR. Morbidity and Mortality Weekly Report. 2009.
17. Tularemia - United States, 2001-2010. — MMWR. Morbidity and Mortality Weekly Report. 2013.
18. Tularemia: An Experience of 13 Cases Including a Rare Myocarditis in a Referral Center in Eastern Switzerland (Central Europe) and a Review of the Literature. — Frischknecht M, Meier A, Mani B, et al. Infection. 2019.
19. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
20. A Clinical Pitfall in Caseating Necrotizing Granulomatous Lymphadenitis: Tularemia. — Özan Köse S, Erdem H, Köse ÖC, Yılmaz Ertürk F. Diagnostic Microbiology and Infectious Disease. 2025.
21. Pulmonary Tularemia: A Diagnosis Not to Overlook. — Zaghdoudi A, Robin F, Moulinie J, et al. International Journal of Infectious Diseases : IJID : Official Publication of the International Society for Infectious Diseases. 2026.
22. Tularemia in Pediatric Patients: A Case Series and Review of the Literature. — Kossadoum RF, Baron A, Parizot M, et al. The Pediatric Infectious Disease Journal. 2025.
23. Tularaemia. — Tärnvik A, Berglund L. The European Respiratory Journal. 2003.
24. ACCF/AHA/CDC Conference Report on Emerging Infectious Diseases and Biological Terrorism Threats. Task Force III: Prevention and Control of Cardiovascular Complications of Emerging Infectious Diseases and Potential Biological Terrorism Agents and Diseases. — Cooper LT, Mensah GA, Baddour LM, et al. Journal of the American College of Cardiology. 2007.
25. ACCF/AHA/CDC Conference Report on Emerging Infectious Diseases and Biological Terrorism Threats. Task Force I: Direct Cardiovascular Implications of Emerging Infectious Diseases and Biological Terrorism Threats. — Baddour LM, Zheng ZJ, Labarthe DR, O'Connor S. Journal of the American College of Cardiology. 2007.