Ulcerative Colitis Flare
An ulcerative colitis (UC) flare is a relapse of mucosal inflammation presenting with bloody diarrhea, urgency, and abdominal cramping in a patient with known UC. Severity ranges from mild (managea…
An ulcerative colitis (UC) flare is a relapse of mucosal inflammation presenting with bloody diarrhea, urgency, and abdominal cramping in a patient with known UC. Severity ranges from mild (manageable outpatient) to acute severe UC (ASUC), which is life-threatening (approximately 1% mortality) and requires hospitalization.[1-2] The 2025 ACG Guideline Update and 2026 AGA Clinical Practice Update provide the most current evidence-based framework for management.[3-4]
1. History
- Stool frequency: number of bowel movements per day, including nocturnal stools (a marker of severity)[3]
- Rectal bleeding: proportion of stools mixed with visible blood, volume, and color
- Urgency and tenesmus: degree of fecal urgency, incontinence episodes
- Abdominal pain: location, severity, cramping vs. constant (constant pain raises concern for complications)
- Duration and progression: onset of worsening, rapidity of symptom escalation
- Triggers: recent NSAID use, smoking cessation, recent antibiotic use, enteric infections, medication nonadherence (common and associated with relapse)[3]
- Weight loss and oral intake: nutritional status, ability to tolerate PO
- Extraintestinal symptoms: joint pain/swelling, skin lesions (erythema nodosum, pyoderma gangrenosum), eye redness/pain, oral ulcers[3][5]
- Current UC medications: adherence, recent changes, prior biologic/immunomodulator exposure and response history
2. Alarm Features
- ≥6 bloody stools/day plus any of: HR >90, temp >37.8°C, Hgb <10.5 g/dL, ESR >30 mm/h → meets Truelove and Witts criteria for ASUC — requires hospitalization[6-7]
- Abdominal distension with tympany → concern for toxic megacolon (transverse colon >5.5 cm on imaging)[3][8]
- Peritoneal signs (rebound, guarding) → perforation until proven otherwise
- Massive hemorrhage requiring transfusion
- Hemodynamic instability or sepsis physiology
- Failure to improve on IV corticosteroids by day 3 (Oxford criteria: >8 stools/day, or 3–8 stools/day with CRP >45 mg/L → 85% colectomy rate)[1][3]
- Hypoalbuminemia and colonic dilation predict failure of medical therapy[3]
3. Medications
Medications that contribute to flares
- NSAIDs — associated with IBD-related hospitalizations and relapses in up to one-third of patients; must be avoided[3]
- Opioids and anticholinergics — may precipitate colonic dilation and toxic megacolon; associated with poor outcomes including infections and mortality[3][8]
- 5-ASA hypersensitivity — paradoxical worsening in patients recently started on mesalamine; should be stopped if suspected[3]
Common treatments by severity
- Mild–moderate flare: optimize oral/topical 5-ASA (mesalamine ≥2 g/day, up to 4.8 g/day); add budesonide MMX 9 mg daily if inadequate response[1]
- Moderate–severe flare (outpatient): oral prednisone 40–60 mg/day, tapered over 2–3 months; initiate steroid-sparing agent (biologic or small molecule)[1-2]
- ASUC (inpatient): IV methylprednisolone 60 mg/day (or hydrocortisone 100 mg TID–QID)[2-3]
- Rescue therapy (IVCS nonresponders by day 3): infliximab 5 mg/kg IV or cyclosporine 2 mg/kg/day IV[1][3]
- Tofacitinib has observational data as salvage in anti-TNF–exposed patients (90-day colectomy-free survival ~86%)[1]
- Contraindicated in ASUC: NSAIDs, opioids, anticholinergics, routine broad-spectrum antibiotics (no benefit for colectomy reduction)[3][6]
4. Diet
- No bowel rest required — the 2025 ACG guideline recommends against TPN for the purpose of bowel rest in ASUC[3]
- Maintain adequate oral intake when tolerated; enteral nutrition is preferred over parenteral
- Avoid high-fiber, raw, or spicy foods during acute flare (empiric, comfort-based)
- Correct dehydration aggressively with IV fluids; replete electrolytes (potassium, magnesium)[2]
- Long-term: no single diet proven to prevent flares, though Mediterranean-style diets are commonly recommended in remission
5. Review of Systems
- GI: stool frequency, blood, mucus, urgency, tenesmus, nocturnal stools, abdominal pain, nausea/vomiting
- Constitutional: fever, weight loss, fatigue, malaise
- MSK: joint pain/swelling (peripheral arthritis is the most common extraintestinal manifestation)[5]
- Dermatologic: new skin lesions (erythema nodosum, pyoderma gangrenosum)
- Ophthalmologic: eye redness, pain, photophobia (uveitis, episcleritis)
- Oral: mouth sores, angular cheilitis[3]
- Hepatobiliary: jaundice, pruritus (primary sclerosing cholangitis)[3]
- Thromboembolic: leg swelling, dyspnea (UC carries elevated VTE risk, especially during flares)[4]
6. Collateral History and Family History
- Family history of IBD — first-degree relatives have significantly increased risk[9]
- Family history of colorectal cancer — impacts surveillance strategy
- Medication adherence — nonadherence is common and a leading cause of relapse; collateral from family/pharmacy records is valuable[3]
- Social context: functional status, ability to manage outpatient care, access to follow-up, psychosocial stressors (UC is associated with reduced quality of life)[1]
- Travel history and sexual history — relevant for infectious mimics[2]
7. Risk Factors
For developing a flare
- Medication nonadherence[3]
- NSAID use[3]
- Recent smoking cessation[3]
- Enteric infections, particularly C. difficile[3]
- Psychosocial stress
Predictors of aggressive course / colectomy
- Young age at diagnosis (<40 years)[6]
- Extensive disease (pancolitis)[6]
- Severe endoscopic activity (deep ulcers, UCEIS ≥7)[3]
- Extraintestinal manifestations[6]
- Early need for corticosteroids[6]
- Elevated inflammatory markers, hypoalbuminemia[3]
8. Differential Diagnosis
- The differential is critical at every flare — infection must be excluded before escalating immunosuppression:[1-2]
- **C. difficile colitis — prevalence 5–47% in relapsing IBD; worsens outcomes dramatically; test at every flare[3][8]
- CMV colitis/reactivation — especially in immunosuppressed patients; biopsy with immunohistochemistry on sigmoidoscopy[3]
- Bacterial enterocolitis — Salmonella, Shigella, Campylobacter, E. coli O157:H7[3]
- Crohn disease — patchy/segmental inflammation, granulomas, perianal disease, small bowel involvement[1]
- Ischemic colitis — especially in elderly; watershed distribution, acute onset[10]
- Drug-induced colitis — checkpoint inhibitors, NSAIDs[1]
- Colorectal cancer — especially in longstanding UC[1]
- STI proctitis — Chlamydia, Gonorrhea, HSV, syphilis (in patients with proctitis and relevant sexual history)[2]
- Segmental colitis associated with diverticulosis — in older patients[1]
9. Past Medical History
- UC disease history: date of diagnosis, disease extent (proctitis, left-sided, pancolitis), prior flare frequency and severity
- Prior hospitalizations and surgeries: previous ASUC episodes, prior colectomy discussions
- Medication history: all prior biologics, immunomodulators, and responses/failures (critical for rescue therapy selection)[8]
- Steroid dependence: number of steroid courses, cumulative exposure
- Comorbidities: VTE history, osteoporosis (steroid-related), PSC, diabetes, cardiovascular disease (relevant for JAK inhibitor risk)[11]
- Vaccination status: hepatitis B, influenza, pneumococcal, varicella zoster (important before immunosuppression)[7]
10. Physical Exam
- Vitals: tachycardia (>90 bpm), fever (>37.8°C), hypotension — markers of systemic toxicity[6-7]
- Abdominal exam: tenderness (location and severity), distension, tympany (suggests dilation), rebound/guarding (perforation), absent bowel sounds (ileus)[3]
- Rectal exam: blood on exam, perianal disease (fistulae/tags suggest Crohn), rectal tenderness
- Volume status: mucous membranes, skin turgor, capillary refill
- Skin: erythema nodosum (tender nodules on shins), pyoderma gangrenosum (ulcerating lesions)
- Eyes: conjunctival injection, scleral injection
- Joints: swelling, tenderness (peripheral arthropathy)
- Nutritional status: muscle wasting, BMI, pallor (anemia)
11. Lab Studies
Initial workup
- CBC: anemia (Hgb <10.5 g/dL is a Truelove and Witts criterion), leukocytosis, thrombocytosis[3][6]
- CRP and ESR: markers of systemic inflammation; CRP >45 mg/L on day 3 of IVCS is prognostic for colectomy[3]
- Albumin: hypoalbuminemia predicts failure of medical therapy, higher risk of hospitalization and surgery[3]
- BMP: electrolytes (hypokalemia, hypomagnesemia common), renal function
- LFTs: baseline and to assess for PSC
- Stool C. difficile toxin (PCR or ELISA): mandatory at every flare[3]
- Stool cultures: bacterial pathogens[3]
- Fecal calprotectin: >150 μg/g reliably suggests moderate-to-severe endoscopic inflammation in symptomatic patients[12]
If rescue therapy anticipated
- Hepatitis B serologies (HBsAg, HBsAb, HBcAb), TB screening (QuantiFERON), HIV, CMV/EBV serologies, TPMT (if thiopurines considered), lipid panel and magnesium (if cyclosporine considered)[7]
12. Imaging
- Plain abdominal radiograph (KUB): first-line in ASUC to assess for toxic megacolon (transverse colon diameter >5.5 cm), mucosal islands, loss of haustrations, and dilated small bowel loops (≥3 dilated loops predict nonresponse to medical therapy)[3]
- CT abdomen/pelvis: reserved for suspected perforation, extraluminal complications, or diagnostic uncertainty between UC and Crohn disease; not routine[3][7]
- Intestinal ultrasound (IUS): emerging noninvasive modality; can detect response to therapy as early as 2 weeks; role in ASUC not yet fully defined[3]
- Imaging is unnecessary in mild flares managed outpatient with clinical and biomarker assessment
13. Special Tests
- Flexible sigmoidoscopy: recommended within 72 hours (preferably within 24 hours) of admission for ASUC — assesses endoscopic severity and obtains biopsies for CMV (immunohistochemistry); full colonoscopy is avoided due to perforation risk[3][8]
- UCEIS score: correlates with need for rescue therapy and colectomy; score ≥7 has high positive predictive value for colectomy[3]
- Mayo Endoscopic Score: widely used; score of 3 (spontaneous bleeding, ulceration) indicates severe disease[1]
- Oxford Index (Day 3 of IVCS): >8 stools/day or 3–8 stools/day + CRP >45 mg/L → 85% predicted colectomy rate[3]
- Fecal calprotectin: useful for monitoring; <50 μg/g in asymptomatic patients correlates with endoscopic remission (false-negative rate <5%)[1]
- The Mayo Score / Disease Activity Index can be used to quantify flare severity:
14. ECG
- Obtain ECG in patients with tachycardia, electrolyte abnormalities, or before initiating cyclosporine (arrhythmia risk with hypomagnesemia)
- Tofacitinib/upadacitinib: baseline ECG reasonable given cardiovascular risk warnings (FDA boxed warning for JAK inhibitors regarding MACE and VTE)[11]
- Etrasimod/ozanimod (S1P receptor modulators): require cardiac evaluation before initiation due to risk of bradycardia and AV block; first-dose monitoring may be needed[11]
- Rule out QTc prolongation before starting medications that may interact with electrolyte derangements
15. Assessment
- Severity stratification is the cornerstone of management and follows the Truelove and Witts criteria:[6-7]
- Mild: <4 stools/day, minimal blood, no systemic toxicity, normal inflammatory markers
- Moderate: 4–6 stools/day, moderate blood, minimal systemic signs
- Severe (ASUC): ≥6 bloody stools/day + ≥1 of: HR >90, temp >37.8°C, Hgb <10.5, ESR >30
- Up to 25% of UC patients will develop ASUC requiring hospitalization, and 40% of those may require colectomy.[8] ASUC carries approximately 1% mortality, higher in elderly patients and those with comorbidities.[1-2] Complications include toxic megacolon (<5% of ASUC), perforation, massive hemorrhage, and VTE.[1][3] Delayed surgery is associated with poor outcomes and must be avoided.[3]
16. Treatment Plan
Mild–moderate flare (outpatient)
- Optimize oral mesalamine (≥2 g/day, up to 4.8 g/day) ± topical mesalamine (rectal suppository or enema)[1]
- If inadequate: budesonide MMX 9 mg daily × 8 weeks[1]
- If still refractory: oral prednisone 40–60 mg/day, taper by 10 mg/week to 20 mg, then 5 mg/week[2]
- Initiate steroid-sparing therapy if steroid-dependent (>1 course/year or unable to taper)
- Moderate–severe flare (outpatient, steroid-refractory/dependent):
- Start advanced therapy per AGA 2024 Living Guideline: in biologic-naïve patients, higher-efficacy agents preferred — infliximab, vedolizumab, upadacitinib, ozanimod, etrasimod, risankizumab, or guselkumab[13]
ASUC (inpatient)
- IV methylprednisolone 60 mg/day (or hydrocortisone 100 mg TID–QID)[3-4]
- IV fluids, electrolyte repletion, correct anemia[2]
- DVT prophylaxis with LMWH (mandatory)[3-4]
- Stop NSAIDs, opioids, anticholinergics[3][8]
- C. difficile testing, stool cultures[3]
- Flexible sigmoidoscopy within 24–72 hours with CMV biopsies[8]
- Daily KUB to monitor for toxic megacolon[8]
- Assess response by day 3 using Oxford criteria[3]
- If nonresponder: initiate rescue therapy — infliximab 5 mg/kg IV (most commonly used) or cyclosporine 2 mg/kg/day IV[1][3]
- Surgical consultation early for all patients failing IVCS; do not delay colectomy beyond 4–7 days of failed medical therapy[3][5]
17. Disposition
Admission criteria
- Meets Truelove and Witts criteria for ASUC[6-7]
- Severe dehydration, inability to tolerate PO, hemodynamic instability
- Suspected complications: toxic megacolon, perforation, massive hemorrhage[8]
- Failure of outpatient therapy with worsening symptoms
- Significant nutritional risk or failure to thrive[4]
Discharge criteria (per RAND Appropriateness Panel)
- Rectal bleeding resolved (Mayo rectal bleeding subscore 0–1)
- Stool frequency returned to baseline (Mayo stool frequency subscore 0–1)
- Observe for 24 hours on oral prednisone (typically 40 mg) to ensure stability before discharge[14]
- Stability of treatment response achieved with clear discharge transition plan[4]
Observation indications
- Moderate flare with borderline vitals, uncertain trajectory, or social barriers to close outpatient follow-up
Specialist consultation triggers
- GI consultation: all admitted UC patients; all patients failing outpatient therapy
- Surgical consultation: all patients failing IVCS by day 3, toxic megacolon, perforation, massive hemorrhage[3][8]
- Colorectal surgery: early involvement recommended in ASUC — all patients should be counseled on potential need for colectomy[4]
18. Follow-Up / Return Precautions
Follow-up timing
- Within 2 weeks of discharge for clinical reassessment[14]
- Lower endoscopy within 4–6 months post-discharge to assess mucosal healing[14]
- Ensure steroid-sparing therapy is initiated or planned before or shortly after discharge if not already started[14]
Symptoms requiring immediate reassessment
- Increasing bloody stool frequency (>6/day)
- Fever, tachycardia, or worsening abdominal pain
- Abdominal distension or inability to pass gas
- Inability to tolerate oral medications or fluids
- Lightheadedness, syncope, or signs of significant bleeding
Patient counseling points
- Medication adherence is critical — nonadherence is the most common modifiable cause of relapse[3]
- Avoid NSAIDs (use acetaminophen for pain)[3]
- Approximately 65–70% of ASUC patients respond to IV corticosteroids; those who do not may need rescue therapy or surgery[5][7]
- VTE risk is elevated during and after flares — early mobilization encouraged
- Expected recovery: mild–moderate flares typically improve within 1–2 weeks of appropriate therapy; ASUC response should be evident by day 3 of IVCS[3]
- Relevant images 4 items
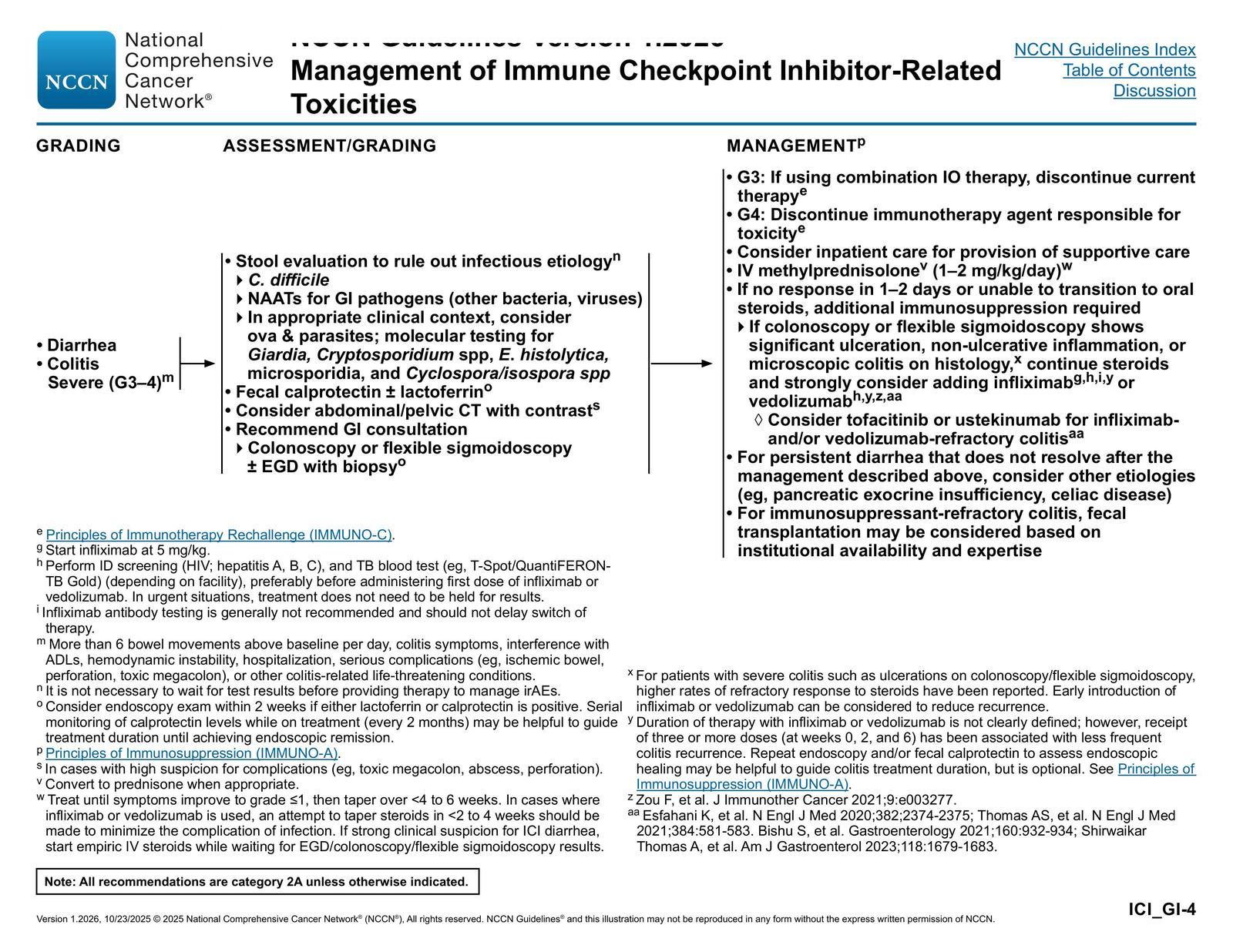
- Management of Diarrhea/Colitis: Severe (G3–4) — NCCN Guidelines® — Management of Immune Checkpoint Inhibitor-Related Toxicities p. 42 (v1.2026)
- NCCN October 22, 2025
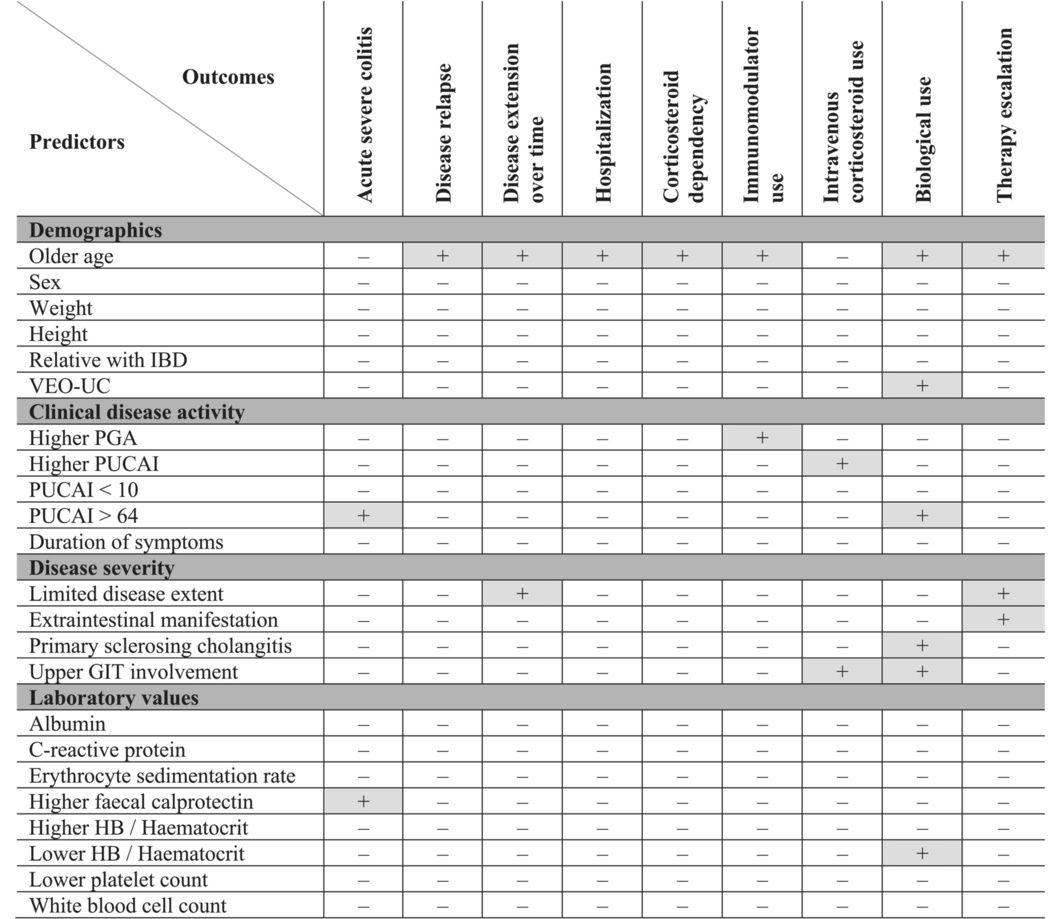
- Overview of disease outcomes and their predictors.
- Alimentary Pharmacology & Therapeutics October 31, 2024
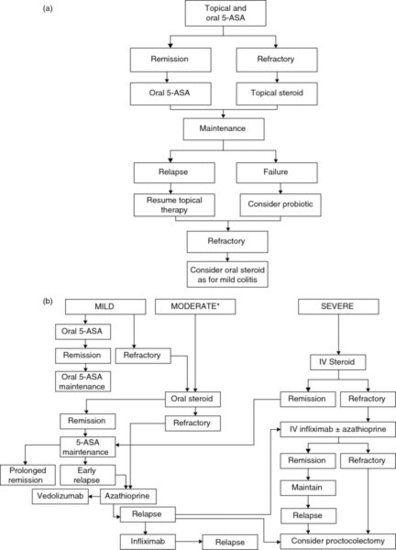
- (a) Algorithm for management of distal ulcerative colitis. (b) Algorithm for management of more extensive ulcerative colitis.
- Evidence‐based Gastroenterology and Hepatology 4e December 31, 2018
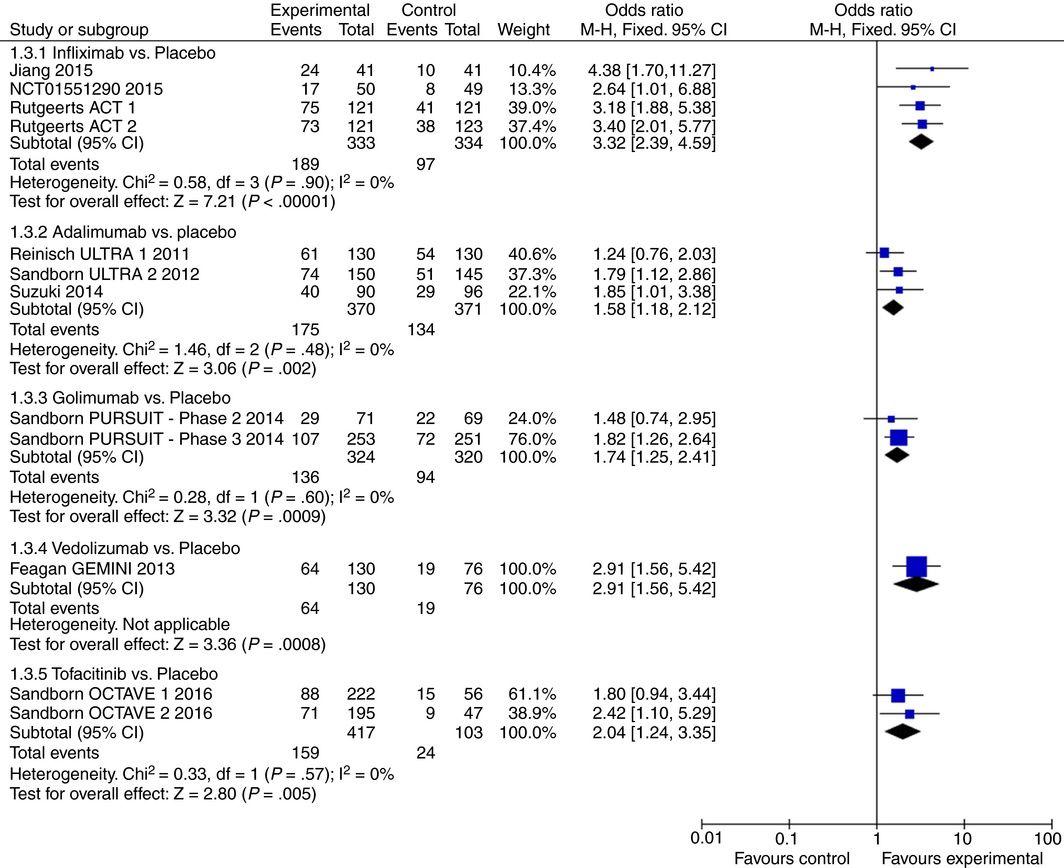
- Efficacy of pharmacological agents in biologic‐naïve patients with moderate‐severe ulcerative colitis for induction of mucosal healing
- Alimentary Pharmacology & Therapeutics December 31, 2017
References
1. Ulcerative Colitis in Adults: A Review. — Gros B, Kaplan GG. The Journal of the American Medical Association. 2023.
2. Ulcerative Colitis. — Le Berre C, Honap S, Peyrin-Biroulet L. Lancet. 2023.
3. ACG Clinical Guideline Update: Ulcerative Colitis in Adults. — Rubin DT, Ananthakrishnan AN, Siegel CA, Barnes EL, Long MD. The American Journal of Gastroenterology. 2025.
4. AGA Clinical Practice Update on Inpatient Management of Adults With Inflammatory Bowel Disease: Expert Review. — Cohen-Mekelburg S, Hashash JG, Loftus EV, Rubin DT. Gastroenterology. 2026.
5. Ulcerative Colitis. — Ungaro R, Mehandru S, Allen PB, Peyrin-Biroulet L, Colombel JF. Lancet. 2017.
6. AGA Clinical Practice Guidelines on the Management of Moderate to Severe Ulcerative Colitis. — Feuerstein JD, Isaacs KL, Schneider Y, et al. Gastroenterology. 2020.
7. Review article: acute severe ulcerative colitis – evidence‐based consensus statements. — Chen JH, Andrews JM, Kariyawasam V, et al. Alimentary Pharmacology & Therapeutics. 2016.
8. ACG Clinical Guideline: Ulcerative Colitis in Adults. — Rubin DT, Ananthakrishnan AN, Siegel CA, Sauer BG, Long MD. The American Journal of Gastroenterology. 2019.
9. Ulcerative Colitis: Rapid Evidence Review. — Adams SM, Close ED, Shreenath AP. American Family Physician. 2022.
10. AGA Clinical Practice Update on Management of Inflammatory Bowel Disease in Elderly Patients: Expert Review. — Ananthakrishnan AN, Nguyen GC, Bernstein CN. Gastroenterology. 2021.
11. FDA Orange Book. — FDA Orange Book. 2026.
12. AGA Clinical Practice Guideline on the Role of Biomarkers for the Management of Ulcerative Colitis. — Singh S, Ananthakrishnan AN, Nguyen NH, et al. Gastroenterology. 2023.
13. AGA Living Clinical Practice Guideline on Pharmacological Management of Moderate-to-Severe Ulcerative Colitis. — Singh S, Loftus EV, Limketkai BN, et al. Gastroenterology. 2024.
14. Recommendations on the Appropriate Management of Steroids and Discharge Planning During and After Hospital Admission for Moderate-Severe Ulcerative Colitis: Results of a RAND Appropriateness Panel. — Dulai PS, Rai V, Raffals LE, et al. The American Journal of Gastroenterology. 2022.