Ulnar Nerve Injury (Acute)
Acute Ulnar Nerve Injury
Acute Ulnar Nerve Injury
The ulnar nerve (C8–T1) is the second most commonly injured peripheral nerve in the upper extremity, with a mean annual incidence of 24.7 per 100,000 person-years.[1] Acute injury can result from direct trauma (laceration, fracture, dislocation), compression (prolonged pressure during anesthesia/coma), traction, or crush mechanisms. The nerve is most vulnerable at the elbow (cubital tunnel/retroepicondylar groove) and the wrist (Guyon's canal) due to its superficial course.[1-3]
1. History
- Mechanism of injury: Direct blow, laceration, fracture (distal humerus, olecranon, medial epicondyle), elbow dislocation, prolonged compression (anesthesia, coma, leaning on hard surface), traction injury
- Symptom characterization: Numbness/tingling in the 5th digit and ulnar half of the 4th digit; pain at the medial elbow radiating distally; hand weakness or clumsiness[1][3-4]
- Timing: Sudden onset (laceration/fracture) vs. hours post-compression (Saturday night palsy equivalent); worsening with elbow flexion suggests cubital tunnel pathology[3]
- Functional impact: Difficulty with grip strength, key pinch, fine motor tasks (buttoning, writing, playing instruments)[3]
- Important negatives: Neck pain, shoulder/arm radiation (argues against radiculopathy), bilateral symptoms (consider polyneuropathy), preceding systemic illness
2. Alarm Features
- Open wound over the ulnar nerve course — suggests laceration/neurotmesis requiring urgent surgical exploration[5-6]
- Rapidly progressive motor weakness or complete motor/sensory loss — suggests severe axonal injury (Sunderland grade ≥3)[5]
- Associated vascular injury (absent ulnar pulse, expanding hematoma, pallor of digits)
- Compartment syndrome signs (tense forearm, pain with passive extension)
- Associated fracture-dislocation of the elbow — high risk of concurrent nerve injury[7]
- Claw hand deformity at presentation — indicates significant motor axon loss[8]
3. Medications
- Acute pain management: NSAIDs (ibuprofen 400–600 mg TID, naproxen 500 mg BID); acetaminophen as adjunct[9]
- Neuropathic pain: Gabapentin (300–900 mg TID) or pregabalin if persistent neuropathic symptoms develop
- Avoid: Opioids beyond a few days post-injury or post-surgery; corticosteroid injection at the elbow is not well-supported and carries risk of nerve damage[9]
- Caution: NSAIDs are not recommended for chronic UNE management per ACOEM guidelines — only for acute/postoperative pain[9]
4. Diet
- No specific dietary triggers or restrictions
- Adequate B-vitamin intake (B6, B12, folate) supports peripheral nerve health
- Optimize glycemic control in diabetic patients, as diabetes is a risk factor for compressive neuropathy[2]
5. Review of Systems
- Neurologic: Neck pain, shoulder/arm weakness, bilateral hand symptoms, bowel/bladder dysfunction (cervical myelopathy)
- Musculoskeletal: Elbow pain, prior fractures, joint instability, wrist pain (Guyon's canal)
- Vascular: Cold digits, color changes, pulse abnormalities
- Constitutional: Weight loss, fatigue (consider malignancy, systemic disease)
- Endocrine: Symptoms of diabetes or hypothyroidism (associated with entrapment neuropathies)[2]
6. Collateral History and Family History
- Witness account of mechanism (especially in trauma, intoxication, or post-anesthesia)
- Occupational history: manual labor, repetitive elbow flexion, vibrating tools, cycling[10]
- Family history: Hereditary neuropathy with liability to pressure palsies (HNPP) — recurrent, painless mononeuropathies in family members
- Social context: Alcohol use (risk for compression during intoxication), recreational drug use
7. Risk Factors
- Trauma: Elbow fracture/dislocation, laceration at wrist or forearm, humeral fracture[7][11]
- Compression: Prolonged anesthesia/coma, habitual elbow leaning, wheelchair use[3]
- Occupational: Construction, concrete work, floor laying, heavy tool use, cycling[10]
- Sports: Overhead throwing (baseball), weightlifting, cycling (cyclist's palsy)[12]
- Anatomic: Shallow ulnar groove, ulnar nerve subluxation/hypermobility, anconeus epitrochlearis[3][12]
- Comorbidities: Diabetes mellitus, hypothyroidism, rheumatoid arthritis, obesity[2][11]
8. Differential Diagnosis
- C8–T1 radiculopathy: Sensory loss extends to medial forearm; weakness includes non-ulnar muscles (flexor pollicis longus, extensor indicis proprius, APB); neck pain common[4][13]
- Lower trunk/medial cord brachial plexopathy: Involves both ulnar and median-innervated hand muscles (opponens, APB); Horner syndrome if preganglionic[4]
- Carpal tunnel syndrome (median neuropathy): Can coexist; different sensory distribution (thumb, index, middle finger); thenar weakness[12]
- Guyon's canal syndrome (ulnar neuropathy at wrist): Spares dorsal ulnar cutaneous sensation; spares FCU and FDP[10]
- Thoracic outlet syndrome: Positional symptoms, vascular changes, broader distribution
- Pancoast tumor: Ipsilateral Horner syndrome, shoulder/arm pain, lower trunk plexopathy
- Motor neuron disease: If pure motor presentation without sensory loss — consider ALS (fasciculations, upper motor neuron signs)
9. Past Medical History
- Prior elbow fractures, dislocations, or surgeries
- Previous episodes of ulnar neuropathy or other entrapment neuropathies
- Diabetes, thyroid disease, rheumatoid arthritis
- History of HNPP or Charcot-Marie-Tooth disease
- Prior anesthesia-related nerve injuries
10. Physical Exam
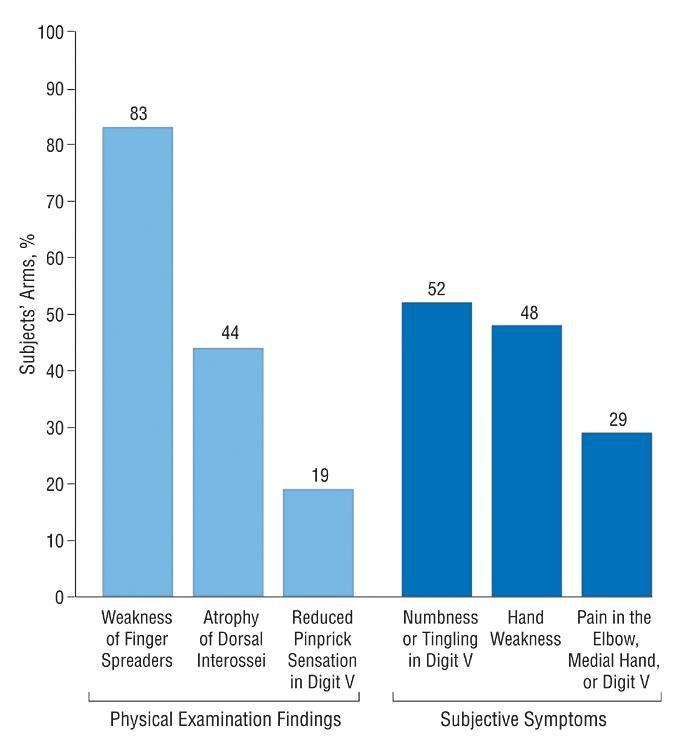
- Inspection: Ulnar claw hand deformity (hyperextension at MCP, flexion at IP joints of 4th/5th digits); hypothenar, interosseous, and first dorsal interosseous (FDI) atrophy; wound/laceration over nerve course[2][7]
- Palpation: Tenderness over cubital tunnel or Guyon's canal; assess for ulnar nerve subluxation with elbow flexion/extension[14]
Provocative tests
- Tinel sign: Percussion over cubital tunnel reproduces paresthesias in 4th/5th digits[4][14]
- Elbow flexion test: Sustained elbow flexion (>60 seconds) reproduces symptoms[3]
- Froment sign: Flexion of thumb IP joint when pinching paper (compensatory FPL activation due to adductor pollicis weakness)[2][15]
- Wartenberg sign: Involuntary abduction of the 5th digit at rest due to weak 3rd palmar interosseous[15-16]
Motor testing (MRC grading)
- Finger abduction/adduction (interossei)
- Thumb adduction (adductor pollicis)
- 5th finger abduction (abductor digiti minimi)
- Grip and pinch strength
- FDP to 4th/5th digits, FCU (if elbow-level lesion)[4]
- Sensory testing: Light touch and pinprick over 5th digit, ulnar half of 4th digit, hypothenar eminence, and dorsal ulnar hand (dorsal ulnar cutaneous nerve — spared in wrist lesions)[10]
- Vascular exam: Ulnar pulse, Allen test, capillary refill
11. Lab Studies
- Routine labs are generally not required for isolated traumatic ulnar nerve injury
Consider if systemic etiology suspected
- Fasting glucose / HbA1c (diabetes screening)
- TSH (hypothyroidism)
- CBC, ESR, CRP (inflammatory/infectious etiology)
- B12, folate (nutritional neuropathy)
- Rheumatoid factor, ANA (if autoimmune arthropathy suspected)
12. Imaging
- X-ray of the elbow: First-line for trauma — evaluate for fracture, dislocation, bony deformity, osteophytes, accessory ossicles[13][17]
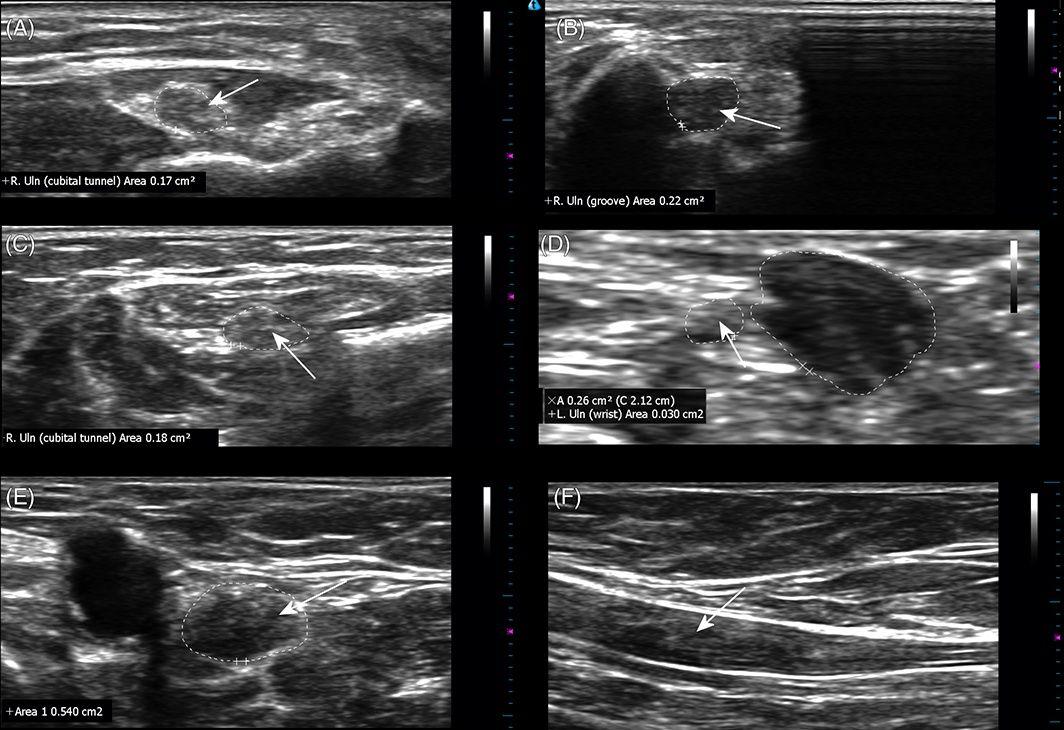
- Ultrasound: Increasingly used as adjunct; can identify nerve enlargement (CSA >8–11 mm² at elbow), subluxation/dislocation, space-occupying lesions (ganglion, lipoma); sensitivity 64–81%, specificity 60–91%[7][18]
- MRI: Gold standard for soft tissue detail; shows nerve thickening, T2 hyperintensity, denervation edema in muscles; useful for space-occupying lesions and when ultrasound is non-diagnostic[1][7]
- CT: Primarily for complex fracture characterization
- Imaging is unnecessary for mild, clearly positional compression injuries that respond to conservative measures
13. Special Tests
- Electrodiagnostic studies (NCS/EMG): Gold standard for confirming diagnosis, localizing lesion, quantifying severity, and differentiating demyelinating (neurapraxia) from axonal (axonotmesis/neurotmesis) injury[1][7][19]
- Motor NCS: Conduction velocity across elbow, recording from ADM and FDI (recording from both increases sensitivity to ~85%)[20]
- Sensory NCS: Ulnar SNAP (normal in pure demyelination, reduced/absent in axonal loss)[19]
- Inching technique: Short-segment stimulation in ~1-inch increments to precisely localize the lesion[9]
- Needle EMG: Evaluate ulnar-innervated muscles (FDI, ADM, FDP, FCU) and non-ulnar C8/T1 muscles to exclude radiculopathy/plexopathy[4][12]
- Timing: For acute traumatic injuries, NCS can be performed immediately to assess for conduction block (neurapraxia); however, Wallerian degeneration takes 7–10 days to manifest on NCS and 2–3 weeks on needle EMG, so repeat testing at 3–4 weeks provides more complete prognostic information[5]
- McGowan grading system: Clinical severity staging[11]
14. ECG
- Not routinely indicated for isolated ulnar nerve injury
- Consider if polytrauma or if the mechanism involves electrical injury
15. Assessment
- Acute ulnar nerve injury severity is classified using the Seddon and Sunderland systems:[5-6]
- Export Seddon Sunderland Pathology Prognosis References Neurapraxia Grade I Focal demyelination; axons intact Full recovery within 3 months[1-2]
- Axonotmesis Grade II Axon disruption; endoneurium intact Favorable; regrowth at 1 mm/day[1]
- Grade III Axon + endoneurium disrupted; perineurium intact Partial recovery; variable[1, 3]
- Grade IV Axon + endoneurium + perineurium disrupted Poor without surgery[1, 3]
- Neurotmesis Grade V Complete nerve transection No recovery without surgery[1-2]
Key clinical pearls
- Acute traumatic UNE tends to show more axonal features on EDx, while chronic compressive UNE is more often demyelinating[22]
- Motor symptoms may be the most clinically relevant finding on presentation, even more than pain[19]
- Surgery is less effective when delayed until significant atrophy or severe axonal degeneration has occurred[23]
16. Treatment Plan
Initial stabilization (ED)
- Wound care and hemostasis for lacerations; assess for tendon/vascular co-injury
- Splint elbow in ~45° of flexion with neutral forearm rotation for comfort and nerve protection[2][9]
- Analgesia: NSAIDs ± acetaminophen; avoid prolonged opioids[9]
Conservative management (neurapraxia, mild axonotmesis)
- Activity modification: Avoid prolonged elbow flexion (>90°), leaning on elbows[9][19]
- Night splinting in ~45° of extension to prevent nocturnal flexion[2][7][9]
- Elbow padding to reduce external compression[19]
- Physical/occupational therapy for nerve gliding exercises and strengthening
- Conservative measures succeed in approximately 62% of cases[19]
Surgical indications
- Immediate: Open laceration/transection (neurotmesis) — primary nerve repair or grafting
- Urgent: Associated fracture/dislocation with nerve compromise requiring operative fixation
- Delayed: No improvement after 3–4 months of conservative treatment; progressive weakness; moderate-to-severe axonal loss on EMG; space-occupying lesion
- Surgical options: In situ decompression vs. anterior transposition (subcutaneous or submuscular) — Cochrane review shows no significant difference in clinical outcomes between simple decompression and transposition[1]
17. Disposition
- Discharge: Most acute ulnar nerve injuries without open wound, vascular compromise, or fracture requiring operative fixation
- Observation/admission: Polytrauma, associated vascular injury, compartment syndrome concern, post-surgical monitoring
- Urgent surgical consultation: Open nerve laceration, complete motor/sensory loss with sharp mechanism, associated displaced fracture/dislocation, expanding hematoma
- Outpatient referral: Hand surgery or peripheral nerve specialist within 1–2 weeks for closed injuries with significant motor deficit; neurology/EMG referral at 3–4 weeks post-injury for prognostic EDx testing[2][6]
18. Follow Up / Return Precautions
- Follow-up timing: 1–2 weeks for wound check (if laceration); 3–4 weeks for repeat clinical exam and EDx testing; 3 months to reassess for spontaneous recovery (neurapraxia window)[5-6]
- Return immediately for: Worsening weakness, new numbness spreading beyond ulnar distribution, signs of infection (wound erythema, drainage, fever), increasing pain/swelling, vascular compromise (cold/pale digits)
Patient counseling
- Avoid resting elbow on hard surfaces; keep elbow relatively extended during sleep
- Expected recovery: Neurapraxia resolves within weeks to 3 months; axonotmesis recovery is slow (~1 mm/day from injury site to target muscle) and may take months[5][21]
- Complete transection (neurotmesis) will not recover without surgical repair[5-6]
- Expected recovery course: Sensory recovery typically precedes motor recovery; intrinsic hand muscle reinnervation may be incomplete, especially with delayed treatment or long regeneration distances[23-24]
- Relevant images 5 items
- Figure 3
- Arch Neurol January 31, 2005
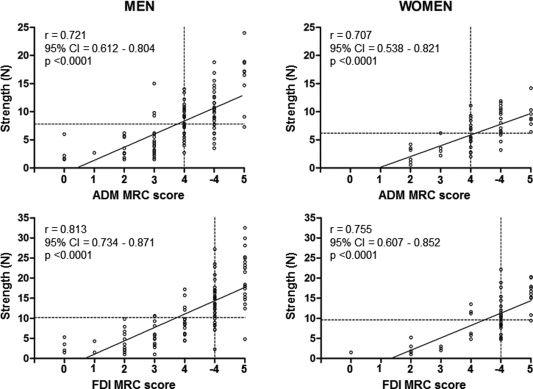
- Correlation between muscle strength tested manually using the MRC scale and measured instrumentally using the RIHM in patients with UNE.
- Muscle & Nerve May 31, 2018
- Representative scans from 4 patients.
- Muscle & Nerve October 31, 2018
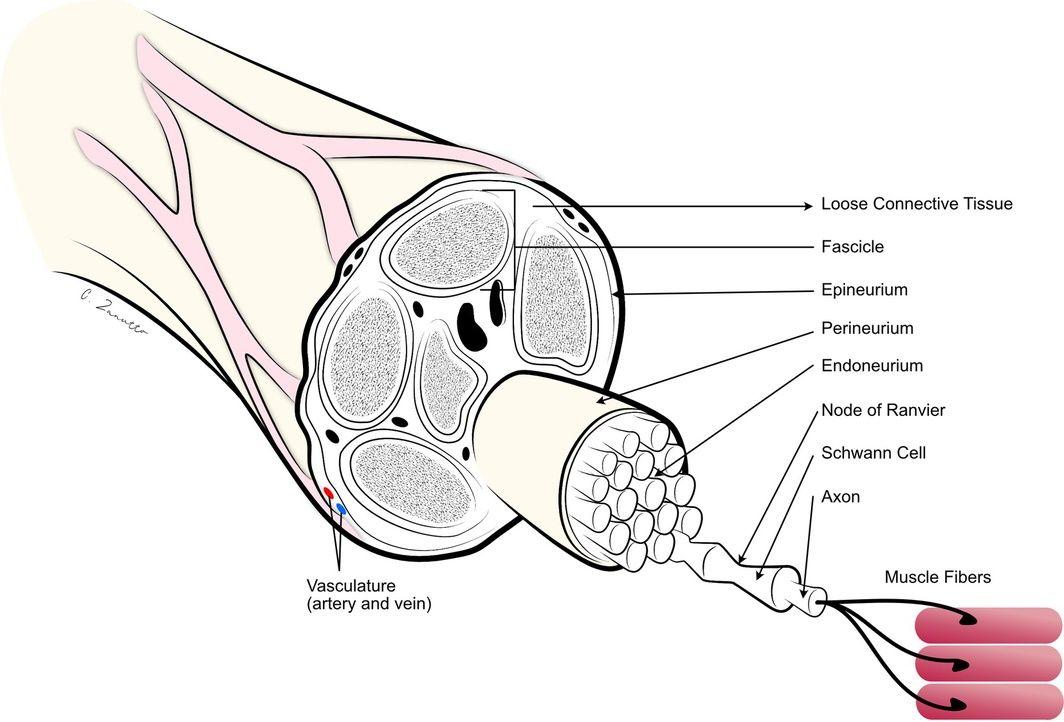
- Anatomy of a peripheral nerve.
- Muscle & Nerve April 30, 2025
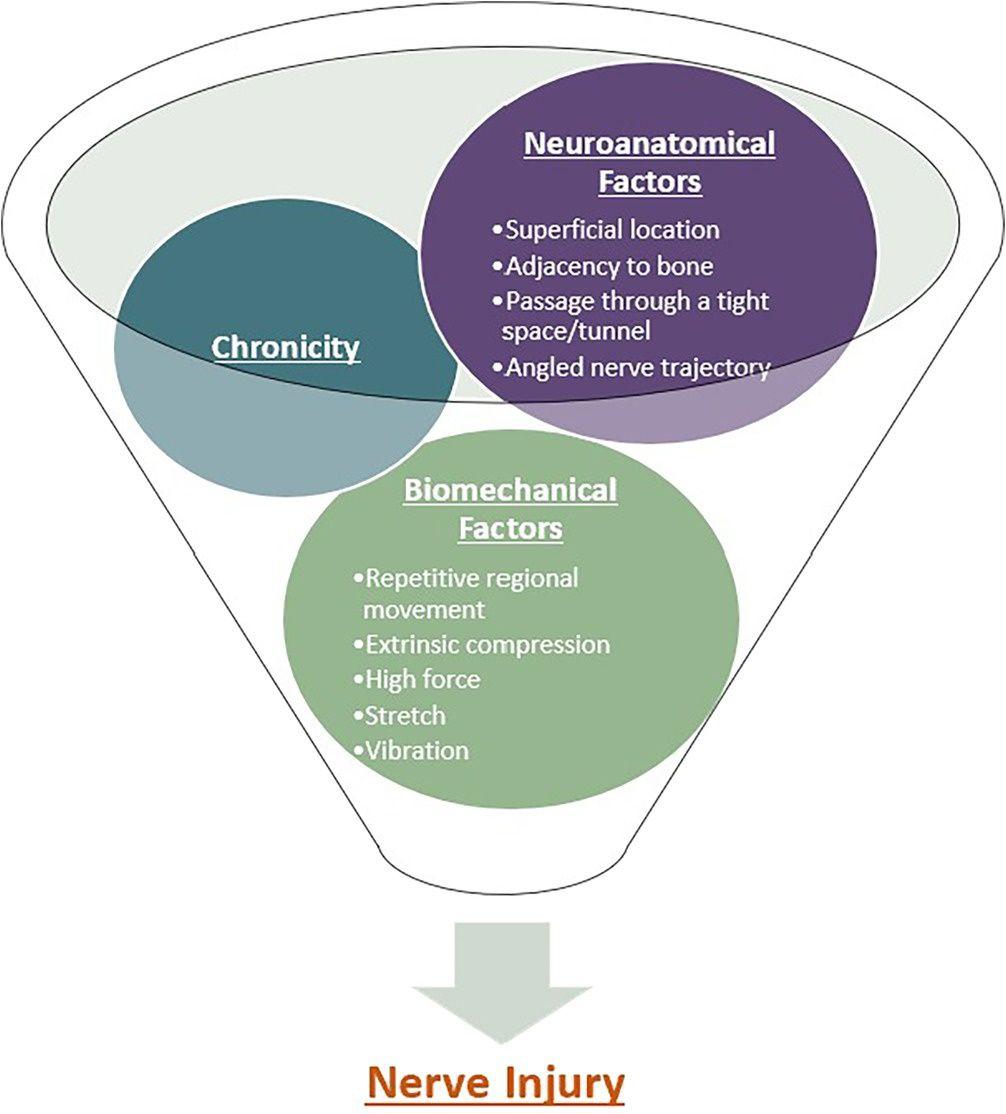
- Convergence of neuroanatomical and biomechanical factors, compounded by chronicity, in causation of nerve injury.
- Muscle & Nerve April 30, 2025
References
1. Treatment for Ulnar Neuropathy at the Elbow. — Caliandro P, La Torre G, Padua R, et al. The Cochrane Database of Systematic Reviews. 2025.
2. Peripheral Nerve Entrapment and Injury in the Upper Extremity. — Silver S, Ledford CC, Vogel KJ, Arnold JJ. American Family Physician. 2021.
3. Entrapment Neuropathies of the Upper Extremities. — Dawson DM. The New England Journal of Medicine. 1993.
4. Clinical Reasoning: A 23-Year-Old Woman With Paresthesias and Weakness. — Karam C, Khorsandi A, MacGowan DJ. Neurology. 2009.
5. Traumatic injury to peripheral nerves. — Robinson LR. Muscle & Nerve. 2022.
6. Assessment, management, and rehabilitation of traumatic peripheral nerve injuries for non‐surgeons. — Bateman EA, Pripotnev S, Larocerie-Salgado J, Ross DC, Miller TA. Muscle & Nerve. 2025.
7. Common sports‐related nerve injuries seen by the electrodiagnostic medical consultant. — Farag JI, McDougall AN, Catapano M. Muscle & Nerve. 2025.
8. Ulnar entrapment neuropathy along the medial intermuscular septum in the midarm. — Nakajima M, Ono N, Kojima T, Kusunose K. Muscle & Nerve. 2009.
9. ACOEM Practice Guidelines: Elbow Disorders. — Hegmann KT, Hoffman HE, Belcourt RM, et al. Journal of Occupational and Environmental Medicine. 2013.
10. Occupational nerve injuries. — Hearn SL, Jorgensen SP, Gabet JM, Carter GT. Muscle & Nerve. 2025.
11. Ulnar Neuropathy of the Elbow. — Norkus SA, Meyers MC. Sports Medicine. 1994.
12. Sports‐related peripheral nerve injuries of the upper limb. — Dutton RA, Norbury J, Colorado B. Muscle & Nerve. 2024.
13. Clinical Reasoning: A 27-Year-Old Man With Hand Numbness: Exploring New Horizons and Reinventing the Past. — Vijayan J, Chuen CY, Punzalan AM, Wilder-Smith E. Neurology. 2014.
14. Ulnar Neuropathy at the Elbow. — Cambon-Binder A. Orthopaedics & Traumatology, Surgery & Research : OTSR. 2021.
15. Primer on the in-Home Teleneurologic Examination: A COVID-19 Pandemic Imperative. — Boes CJ, Leep Hunderfund AN, Martinez-Thompson JM, et al. Neurology. Clinical Practice. 2021.
16. Analysis of Clinical Motor Testing for Adult Patients With Diagnosed Ulnar Neuropathy at the Elbow. — Goldman SB, Brininger TL, Schrader JW, Curtis R, Koceja DM. Archives of Physical Medicine and Rehabilitation. 2009.
17. Ulnar Nerve Neuropathy Caused by Pathologic Ossification: A Case Report. — Vojtěch K, David K, Ivan H. Surgical and Radiologic Anatomy : SRA. 2023.
18. Expert Consensus on the Combined Investigation of Ulnar Neuropathy at the Elbow Using Electrodiagnostic Tests and Nerve Ultrasound. — Pelosi L, Arányi Z, Beekman R, et al. Clinical Neurophysiology : Official Journal of the International Federation of Clinical Neurophysiology. 2021.
19. An electrodiagnostic grading system for ulnar neuropathy at the elbow. — Zeidman LA, Pandey DK. Muscle & Nerve. 2020.
20. Clinical Findings and Electrodiagnostic Testing in Ulnar Neuropathy at the Elbow and Differences According to Site and Type of Nerve Damage. — Vinciguerra C, Curti S, Aretini A, et al. American Journal of Physical Medicine & Rehabilitation. 2020.
21. Peripheral Nerve Reconstruction after Injury: A Review of Clinical and Experimental Therapies. — Grinsell D, Keating CP. BioMed Research International. 2014.
22. Comparison of electrodiagnostic findings in acute traumatic versus chronic non‐traumatic ulnar neuropathy at the elbow. — Robinson LR, Broadhurst P, Wasserman A. Muscle & Nerve. 2024.
23. In situ decompression vs conservative treatment for mild ulnar neuropathy at the elbow. — Pompe SM, Schreuder T, Teunissen LL, Visser LH, Beekman R. Muscle & Nerve. 2020.
24. How electrodiagnosis predicts clinical outcome of focal peripheral nerve lesions. — Robinson LR. Muscle & Nerve. 2015.