Upper GI Bleed (PUD)
Peptic ulcer disease is the most common cause of upper GI bleeding, accounting for 40–60% of all UGIB cases, with a hospitalization rate of ~67 per 100,000 in the US and in-hospital mortality of 2–…
Peptic ulcer disease is the most common cause of upper GI bleeding, accounting for 40–60% of all UGIB cases, with a hospitalization rate of ~67 per 100,000 in the US and in-hospital mortality of 2–10%.[1-2] The following is a comprehensive EM/primary care–focused clinical summary.
1. History
- Hematemesis (bright red blood or coffee-ground emesis) and/or melena (black, tarry stools); hematochezia if brisk bleeding[3-4]
- Epigastric pain (present in ~81% of PUD patients), burning quality, may improve with food (duodenal) or worsen postprandially (gastric)[5]
- Nocturnal pain/awakening (41%), nausea/vomiting (25%), belching (43%)[3]
- Timing: acute onset vs. chronic/relapsing symptoms; prior episodes of GI bleeding
- Quantify blood loss: number of episodes of hematemesis/melena, volume, duration
- Symptoms of hypovolemia: lightheadedness, dizziness, syncope, dyspnea on exertion, chest pain
- Important negatives: no retching/vomiting before hematemesis (argues against Mallory-Weiss), no liver disease/alcohol use (argues against variceal bleed), no weight loss/dysphagia (argues against malignancy)
- Nearly half of patients with bleeding PUD have no preceding warning symptoms[6]
2. Alarm Features
- Hemodynamic instability: tachycardia, hypotension, orthostatic changes
- Large-volume hematemesis or bright red blood per rectum
- Syncope or altered mental status
- Signs of peritonitis (sudden severe abdominal pain, rigidity) → suspect perforation[3]
- Recurrent vomiting with inability to tolerate PO → suspect gastric outlet obstruction
- Unintentional weight loss, dysphagia, palpable mass → concern for malignancy
- Hemoglobin drop >2 g/dL, need for ongoing transfusion
- Ongoing bleeding despite initial resuscitation
3. Medications
Contributors to bleeding risk (ask about all)
- NSAIDs (4× increased risk of PUD complications; IRR 4.3 for UGIB)
- Low-dose aspirin (2–4× increased risk)
- Dual antiplatelet therapy (DAPT: aspirin + P2Y12 inhibitor) — 2–3× risk vs. aspirin alone
- Anticoagulants (warfarin, DOACs) — adjusted OR 2.34 for PUB
- Corticosteroids (especially with concurrent NSAIDs; IRR up to 12.8 combined)
- SSRIs (impair platelet function; OR 1.75 for UGIB when combined with NSAIDs)[9-10]
- Aldosterone antagonists (IRR 11.0 when combined with nsNSAIDs)[8]
Acute treatment medications
- PPI: IV bolus 80 mg pantoprazole/esomeprazole, then 8 mg/hr continuous infusion OR 40 mg IV q8–12h for 72 hours post-endoscopy[4][11]
- Erythromycin 250 mg IV 30–90 min pre-endoscopy (prokinetic to improve visualization); metoclopramide if erythromycin unavailable[12]
- Tranexamic acid is NOT recommended in UGIB[11]
Contraindicated/caution
- Avoid NSAIDs in active bleeding
- H2-receptor antagonists are inferior to PPIs and should not be substituted[7]
4. Diet
- NPO initially until hemodynamic stability and endoscopic assessment
- Early refeeding within 24 hours after endoscopic hemostasis decreases hospital length of stay[3]
- Long-term: avoid alcohol, smoking, spicy foods, caffeine (may exacerbate symptoms though not proven to cause ulcers)
- Adequate hydration during recovery
5. Review of Systems
- GI: hematemesis, melena, hematochezia, abdominal pain, nausea/vomiting, early satiety, weight loss, dysphagia
- Cardiovascular: chest pain, palpitations, dyspnea (anemia/hypovolemia symptoms)
- Neurologic: dizziness, lightheadedness, syncope, altered mental status
- Constitutional: fatigue, weakness, pallor
- Hepatic: jaundice, ascites, spider angiomata (to evaluate for variceal etiology)
6. Collateral History and Family History
- Confirm medication list with pharmacy/family — especially OTC NSAIDs, aspirin, supplements (iron, bismuth can mimic melena)
- Prior endoscopy results, prior H. pylori treatment and eradication confirmation
- Alcohol use history (quantity, duration) — cirrhosis/variceal risk
- Family history of PUD, GI malignancy, bleeding disorders
- Social context: functional status, ability to recognize return precautions, reliable follow-up
7. Risk Factors
- H. pylori infection (present in 20–50% of bleeding PUD patients)[13]
- NSAID/aspirin use — most important modifiable risk factor
- Age >60–65 years (highest attributable risk at 25%)[14]
- Prior history of PUD or GI bleeding
- Concurrent use of multiple ulcerogenic medications
- Smoking, heavy alcohol use
- Severe comorbidities (cardiovascular disease, renal failure, hepatic disease)
- Physiologic stress (ICU patients, major surgery, burns, sepsis)
- Zollinger-Ellison syndrome — rare; suspect with recurrent/refractory multiple ulcers[5]
8. Differential Diagnosis
- Export Diagnosis Distinguishing Features References Esophageal/gastric varices Cirrhosis, portal hypertension, large-volume hematemesis, stigmata of liver disease[1-2]
- Mallory-Weiss tear Preceded by forceful retching/vomiting, linear tear at GEJ, often self-limited[1]
- Erosive esophagitis/gastritis GERD symptoms, NSAID use, typically less severe bleeding[1]
- GI malignancy Weight loss, dysphagia, anorexia, older age, iron deficiency anemia[1, 3]
- Dieulafoy lesion Intermittent massive bleeding, normal surrounding mucosa, difficult to diagnose[1]
- Aortoenteric fistula History of aortic graft, "herald bleed" followed by massive hemorrhage — cannot miss[1, 3]
- Gastric antral vascular ectasia (GAVE) "Watermelon stomach," chronic occult blood loss, associated with cirrhosis/autoimmune disease[4]
- Hemobilia/hemosuccus pancreaticus Post-procedural, hepatobiliary/pancreatic pathology[3]
9. Past Medical History
- Prior PUD, prior GI bleeding episodes, prior endoscopic interventions
- H. pylori infection status and prior eradication attempts
- Liver disease/cirrhosis (changes management entirely — variceal protocol)
- Cardiovascular disease (affects transfusion thresholds and antithrombotic decisions)
- Chronic kidney disease (uremic platelet dysfunction)
- Coagulopathies, thrombocytopenia
- Prior abdominal/aortic surgery (aortoenteric fistula risk)
10. Physical Exam
- Vitals: HR, BP (orthostatics), RR, SpO2 — assess for shock (tachycardia, hypotension)
- General: pallor, diaphoresis, altered mental status
- Abdomen: epigastric tenderness (common in PUD); peritoneal signs (rigidity, rebound) → perforation; distension, succussion splash → gastric outlet obstruction
- Rectal exam: melena, hematochezia, stool color
- Skin: pallor, petechiae/purpura (coagulopathy), spider angiomata, palmar erythema, caput medusae (liver disease)
- Stigmata of chronic liver disease: jaundice, ascites, gynecomastia, splenomegaly
11. Lab Studies
- CBC (hemoglobin — note initial Hgb may not reflect true blood loss for 24–72 hours)
- BMP (BUN:Cr ratio >20:1 suggests upper GI source; assess renal function)
- Coagulation studies: PT/INR, aPTT (especially if on anticoagulants)
- Type and screen/crossmatch — order early
- Liver function tests (evaluate for underlying liver disease)
- Lactate (tissue hypoperfusion marker in severe bleeding)
- H. pylori testing: biopsy at endoscopy; if negative, repeat non-invasive testing (UBT or stool antigen) ≥2 weeks after stopping PPI and ≥4 weeks after antibiotics to avoid false negatives (25–55% false-negative rate during acute bleeding)[3]
Transfusion thresholds
- Hgb <7 g/dL → transfuse (restrictive strategy reduces mortality)
- Hgb <8 g/dL → transfuse if active cardiovascular disease
- Hemodynamically unstable with active bleeding → transfuse regardless of Hgb level[18]
12. Imaging
- Imaging is generally NOT first-line — endoscopy is the gold standard for both diagnosis and treatment[5-6]
- CT angiography (CTA): indicated when endoscopy fails to identify or control bleeding source, or when interventional radiology (TAE) is being considered[16]
- CT abdomen/pelvis with contrast: if perforation suspected (free air under diaphragm)[3]
- Conventional angiography: therapeutic (transcatheter arterial embolization) when endoscopic hemostasis fails[12]
- Imaging is unnecessary in straightforward presentations managed with endoscopy
13. Special Tests
Risk Stratification Scores
- The Glasgow-Blatchford Score (GBS) is the recommended pre-endoscopic risk stratification tool:[4][7][19]
- GBS ≤1: very low risk — safe for outpatient management and discharge from ED[3]
- GBS ≥7: predicts need for endoscopic therapy (sensitivity 80%, specificity 57%)[19]
- <calculator slug="glasgow-blatchford-bleeding-score"/>
- The AIMS65 score (Albumin <3, INR >1.5, Altered mental status, SBP ≤90, Age ≥65) is superior for predicting in-hospital mortality.[7][19]
- The Forrest Classification (post-endoscopy) guides endoscopic therapy and predicts rebleeding risk:[1][3]
- Ia (active spurting), Ib (oozing) → highest rebleeding risk → endoscopic therapy required
- IIa (visible vessel) → endoscopic therapy required
- IIb (adherent clot) → endoscopic therapy may be individualized[12]
- IIc (flat spot), III (clean base) → low risk, no endoscopic therapy needed
Other
- Nasogastric tube lavage is NOT recommended for diagnosis based on current evidence[18]
14. ECG
- Obtain ECG in all patients with significant bleeding, especially those with:
- Known cardiovascular disease
- Tachycardia, hypotension, chest pain, dyspnea
- Elderly patients
- Look for: ST changes, T-wave inversions (demand ischemia from anemia/hypovolemia), arrhythmias (atrial fibrillation — relevant to anticoagulation decisions)
- ECG findings may influence transfusion threshold (Hgb <8 g/dL if myocardial ischemia)[18]
15. Assessment
- UGIB from PUD is the most common cause of nonvariceal UGIB, accounting for ~50% of cases[2][20]
- Bleeding occurs without warning symptoms in nearly half of patients[6]
- Mortality remains 2–10% depending on setting and comorbidities; in-hospital bleeding carries 3–4× higher mortality than primary admission for UGIB[2]
- Severity stratification should be based on GBS (pre-endoscopy) and Forrest classification (post-endoscopy)
- Atypical presentations: elderly patients may be asymptomatic; hematochezia can occur with brisk upper GI bleeding; patients on anticoagulants may bleed from previously silent ulcers
- Complications: rebleeding (highest risk in first 72 hours), perforation, gastric outlet obstruction, death
16. Treatment Plan
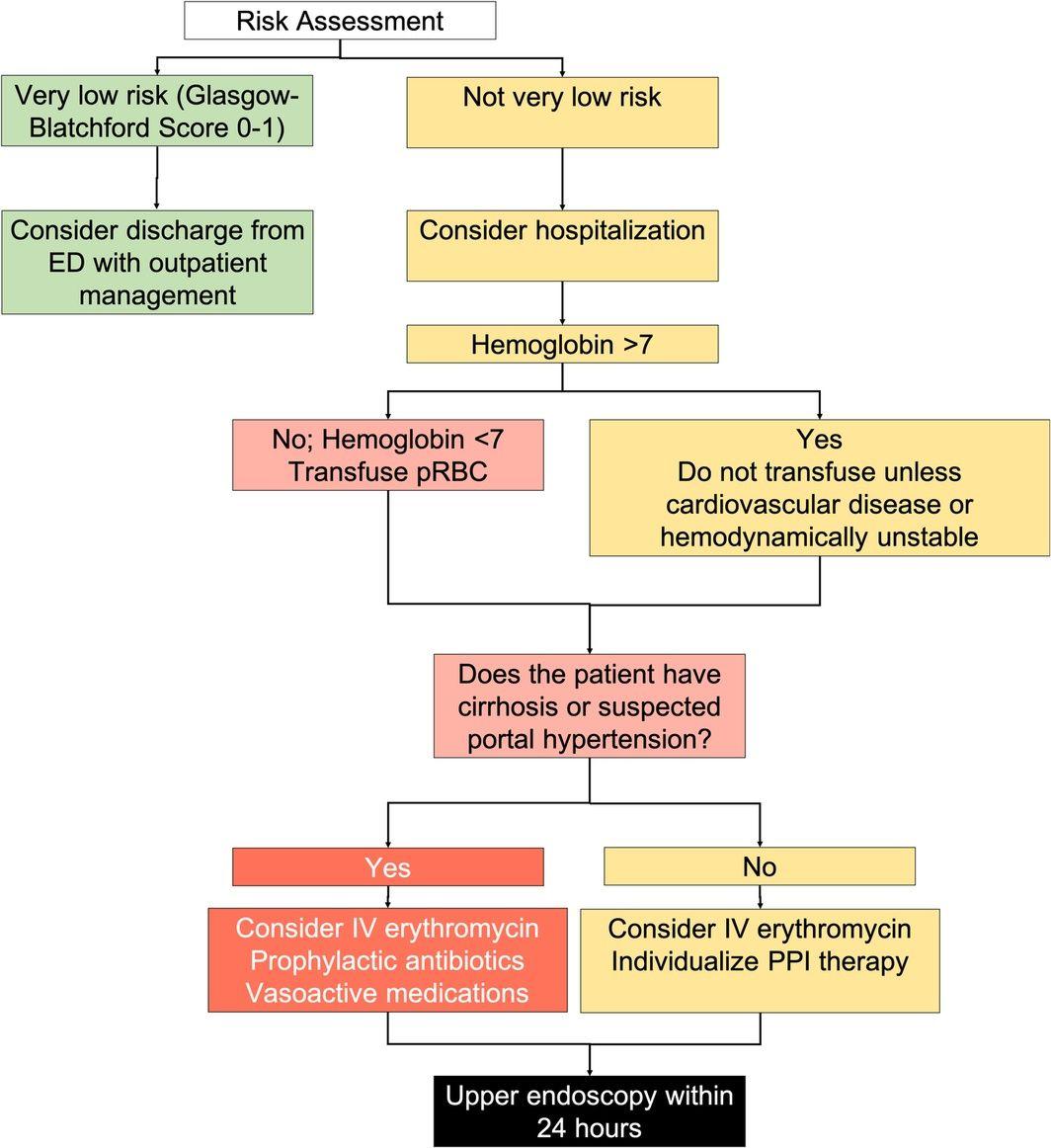
- The following figure summarizes the pre-endoscopic management algorithm:
- View full figure Figure 1. Pre‐endoscopic management for patients with acute upper gastrointestinal bleeding. Review article: Upper gastrointestinal bleeding – review of current evidence and implications for management. Aliment Pharmacol Ther. April 30, 2024.
Initial stabilization
- 2 large-bore IVs, crystalloid resuscitation to restore end-organ perfusion[3]
- Restrictive transfusion strategy as above
- Continuous monitoring, NPO
Pharmacotherapy
- PPI: IV bolus 80 mg → continuous infusion 8 mg/hr OR intermittent 40 mg IV q8–12h — both strategies are acceptable per ACG guidelines[4][11]
- Pre-endoscopy PPI reduces high-risk stigmata and need for endoscopic therapy but does not improve mortality[7][20]
- Erythromycin 250 mg IV 30–90 min before endoscopy in selected patients with clinically severe/ongoing bleeding[12]
Endoscopy (within 24 hours of presentation)
- Urgent endoscopy (<6–12 hours) is NOT recommended before adequate resuscitation, even in high-risk patients — a large RCT showed no benefit of urgent vs. early endoscopy[4][21]
- Endoscopic therapy for Forrest Ia, Ib, IIa lesions; combination therapy preferred (e.g., epinephrine injection + thermal/clips); epinephrine alone is insufficient[11]
- Over-the-scope clips (OTSC) may be used as monotherapy as an alternative to combination therapy for high-risk stigmata[12]
- Post-endoscopy PPI (for high-risk stigmata treated endoscopically):[2][4]
- 80 mg IV bolus → 8 mg/hr infusion (or 40 mg 2–4× daily) for 72 hours
- Then twice-daily oral PPI for 2 weeks, followed by once-daily PPI
- Duration of PPI depends on etiology: 4–8 weeks for H. pylori–negative ulcers; through completion of eradication therapy if H. pylori–positive[2]
H. pylori management
- Test ALL patients with bleeding PUD
- If positive → eradication therapy (14-day course preferred); first-line: bismuth quadruple therapy or concomitant quadruple therapy depending on local resistance patterns[3][6]
- Confirm eradication ≥4 weeks after antibiotics and ≥2 weeks off PPI
- Rebleeding rate drops to 1.3% with confirmed eradication vs. 26% without treatment[2]
Rebleeding
- If clinical evidence of rebleeding → repeat endoscopy with OTSC consideration
- If second endoscopy fails → transcatheter arterial embolization (TAE)
- Surgery if TAE unavailable or unsuccessful
Antithrombotic resumption
- Aspirin for secondary prevention: resume within 1–3 days after hemostasis (RCT showed 30-day mortality 1% with aspirin vs. 9% with placebo)[2][22]
- Aspirin for primary prevention: risk of rebleeding likely outweighs benefit — consider discontinuation[2]
- Anticoagulants: resume when clinically indicated based on thromboembolic risk; general guidance suggests within 7–15 days post-bleed, with PPI co-therapy[12][23]
- DAPT: do not stop aspirin in high thrombotic risk patients; resume second agent as soon as hemostasis is achieved[7]
17. Disposition
- Discharge from ED: GBS ≤1 with outpatient endoscopy arranged[3][19]
- Admit to floor: hemodynamically stable, GBS 2–6, no active comorbidities
- Admit to ICU/monitored bed: hemodynamic instability, active hematemesis, GBS ≥7, significant comorbidities, need for urgent endoscopy
- Observation: borderline cases, elderly with low GBS but significant comorbidities
- Typical hospital stay: 3 days post-endoscopy if no rebleeding and no other medical issues[2]
- Specialist consultation triggers: GI for endoscopy (all admitted patients); interventional radiology if endoscopic hemostasis fails; surgery if TAE unavailable/unsuccessful; cardiology if antithrombotic management is complex
18. Follow Up / Return Precautions
Follow-up timing
- Outpatient GI follow-up within 1–2 weeks post-discharge
- Repeat endoscopy for gastric ulcers at 8–12 weeks to confirm healing and exclude malignancy (biopsy if not done)[5]
- H. pylori eradication confirmation testing at ≥4 weeks post-antibiotics
- Return precautions — instruct patients to return immediately for:
- Recurrent hematemesis or coffee-ground emesis
- Melena or bloody stools
- Lightheadedness, dizziness, syncope
- Severe abdominal pain
- Chest pain or shortness of breath
Patient counseling
- Avoid NSAIDs/aspirin unless specifically directed by physician
- Take PPI as prescribed; do not stop early
- Avoid alcohol and smoking
- Iron supplementation should be initiated prior to discharge if iron deficiency/anemia present[12]
- Expected recovery: most patients recover without rebleeding; among those with rebleeding, 44% occurs after day 3 and 24% after day 7[2]
- Patients should be informed about symptoms of recurrent upper gastrointestinal bleeding and the need to return to the emergency department if any occur.
- — Loren Laine, M.D., Yale School of Medicine and other institutions
- Upper Gastrointestinal Bleeding Due to a Peptic Ulcer. N Engl J Med. June 15, 2016.
References
1. Prophylactic Transarterial Embolization in Patients With Bleeding Peptic Ulcers Following Endoscopic Control of Bleeding. — Zetner D, Roost I, Rosenberg J, Andresen K. The Cochrane Database of Systematic Reviews. 2025.
2. Upper Gastrointestinal Bleeding Due to a Peptic Ulcer. — Laine L. The New England Journal of Medicine. 2016.
3. Peptic Ulcer Disease. — Almadi MA, Lu Y, Alali AA, Barkun AN. Lancet. 2024.
4. ACG Clinical Guideline: Upper Gastrointestinal and Ulcer Bleeding. — Laine L, Barkun AN, Saltzman JR, Martel M, Leontiadis GI. The American Journal of Gastroenterology. 2021.
5. Peptic Ulcer Disease: A Review. — Vakil N. The Journal of the American Medical Association. 2024.
6. Peptic Ulcer Disease. — Lanas A, Chan FKL. Lancet. 2017.
7. Gastrointestinal Surgical Emergencies Textbook. — Ashley E. Aaron, Andrea Amabile, Ciro Andolfi, et al American College of Surgeons (2021). 2021.
8. Risk of Upper Gastrointestinal Bleeding From Different Drug Combinations. — Masclee GM, Valkhoff VE, Coloma PM, et al. Gastroenterology. 2014.
9. Selective Serotonin Reuptake Inhibitors Increase Risk of Upper Gastrointestinal Bleeding When Used With NSAIDs: A Systemic Review and Meta-Analysis. — Alam SM, Qasswal M, Ahsan MJ, Walters RW, Chandra S. Scientific Reports. 2022.
10. Risk of Gastrointestinal Bleeding With Concurrent Use of NSAID and SSRI: A Systematic Review and Network Meta-Analysis. — Haghbin H, Zakirkhodjaev N, Husain FF, Lee-Smith W, Aziz M. Digestive Diseases and Sciences. 2023.
11. Review article: Upper gastrointestinal bleeding – review of current evidence and implications for management. — Shung DL, Laine L. Alimentary Pharmacology & Therapeutics. 2024.
12. Endoscopic Diagnosis and Management of Peptic Ulcer Bleeding: European Society of Gastrointestinal Endoscopy (ESGE) Guideline - Update 2026. — Gralnek IM, Morris J, Laursen SB, et al. Endoscopy. 2026.
13. Perforated and Bleeding Peptic Ulcer: WSES Guidelines. — Tarasconi A, Coccolini F, Biffl WL, et al. World Journal of Emergency Surgery : WJES. 2020.
14. Contribution of Helicobacter pylori infection to the risk of peptic ulcer bleeding in patients on nonsteroidal anti‐inflammatory drugs, antiplatelet agents, anticoagulants, corticosteroids and selective serotonin reuptake inhibitors. — Venerito M, Schneider C, Costanzo R, et al. Alimentary Pharmacology & Therapeutics. 2018.
15. Characteristics of Peptic Ulcer Bleeding in Cirrhotic Patients With Esophageal and Gastric Varices. — Lu Z, Sun X, Han J, et al. Scientific Reports. 2020.
16. ACR Appropriateness Criteria® Nonvariceal Upper Gastrointestinal Bleeding: 2024 Update. — Nagpal P, Dane B, Aghayev A, et al. Journal of the American College of Radiology : JACR. 2024.
17. Endoscopic diagnosis and treatment of nonvariceal upper gastrointestinal hemorrhage. — Andrew W. Yen, Joseph W. Leung Yamada's Textbook of Gastroenterology 7e. 2022.
18. Emergency Medicine Updates: Upper Gastrointestinal Bleeding. — Long B, Gottlieb M. The American Journal of Emergency Medicine. 2024.
19. Comparison of Risk Scoring Systems for Patients Presenting With Upper Gastrointestinal Bleeding: International Multicentre Prospective Study. — Stanley AJ, Laine L, Dalton HR, et al. BMJ. 2017.
20. Proton Pump Inhibitor Treatment Initiated Prior to Endoscopic Diagnosis in Upper Gastrointestinal Bleeding. — Kanno T, Yuan Y, Tse F, et al. The Cochrane Database of Systematic Reviews. 2022.
21. Timing of Endoscopy for Acute Upper Gastrointestinal Bleeding. — Lau JYW, Yu Y, Tang RSY, et al. The New England Journal of Medicine. 2020.
22. American College of Gastroenterology-Canadian Association of Gastroenterology Clinical Practice Guideline: Management of Anticoagulants and Antiplatelets During Acute Gastrointestinal Bleeding and the Periendoscopic Period. — Abraham NS, Barkun AN, Sauer BG, et al. The American Journal of Gastroenterology. 2022.
23. Re-Starting Anticoagulation and Antiplatelets After Gastrointestinal Bleeding: A Systematic Review. — Slouha E, Jensen H, Fozo H, et al. F1000Research. 2023.