Upper GI Bleed (Variceal)
Acute variceal hemorrhage (AVH) is a life-threatening complication of portal hypertension, most commonly from esophageal or gastric varices in cirrhotic patients. Even with modern therapy, 6-week m…
Acute variceal hemorrhage (AVH) is a life-threatening complication of portal hypertension, most commonly from esophageal or gastric varices in cirrhotic patients. Even with modern therapy, 6-week mortality remains 10–20%, with most deaths occurring in Child-Pugh class C patients.[1-2] The following is a structured clinical summary for emergency medicine and primary care management.
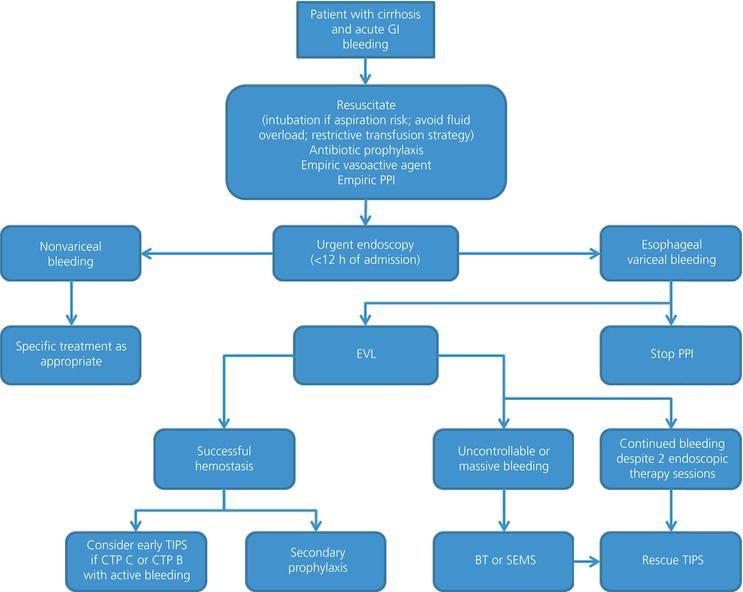
The following algorithm outlines the management pathway for acute GI bleeding in cirrhotic patients:
1. History
- Hematemesis (bright red blood or coffee-ground emesis) — red blood emesis is the most common presentation of variceal bleeding (67%), while melena predominates in peptic ulcer bleeding[4-5]
- Volume and frequency of hematemesis, presence of melena or hematochezia
- Timing of onset, rapidity of progression, preceding symptoms (lightheadedness, syncope, presyncope)
- Prior episodes of GI bleeding or known varices
- Known liver disease, cirrhosis etiology (alcohol, viral hepatitis, NAFLD, autoimmune)
- Recent alcohol use, NSAID/aspirin use, anticoagulant use
- Symptoms of hepatic encephalopathy (confusion, somnolence)
- Important negatives: abdominal pain (less typical in variceal bleed vs. peptic ulcer), dysphagia, weight loss
2. Alarm Features
- Hemodynamic instability: tachycardia, hypotension, orthostasis — common in AVH[6]
- Massive hematemesis with bright red blood
- Altered mental status (encephalopathy vs. hypovolemic shock)
- Signs of aspiration (cough, desaturation during active emesis)
- Refractory bleeding despite initial resuscitation
- Features of decompensated cirrhosis: new or worsening ascites, jaundice, encephalopathy
- Myocardial injury occurs in ~36% of cirrhotic patients with variceal bleeding and is independently associated with higher 6-week mortality (21% vs. 7%)[7]
3. Medications
Acute treatment
- Octreotide: 50 mcg IV bolus → 25–50 mcg/hr infusion for 2–5 days (most commonly used vasoactive agent in the US)[1][8]
- Terlipressin: 2 mg IV q4–6h for 24–48h, then 1 mg IV q4–6h (not approved for this indication in North America)[1]
- Ceftriaxone: 1 g IV q24h for up to 5 days — prophylactic antibiotics reduce short-term mortality (18.5% vs. 22.2% with placebo)[1][9]
- Erythromycin: 125–250 mg IV given 30–120 min before endoscopy as a prokinetic to improve visualization[1]
- PPI: may be started empirically if non-variceal source cannot be excluded[10]
Prophylaxis (secondary prevention)
- Carvedilol (preferred, 12.5 mg daily) or propranolol — initiate at discontinuation of vasoactive therapy[1][9]
- Combination NSBB + EVL is standard for secondary prophylaxis[11]
Contraindicated/caution
- NSAIDs — increase bleeding risk
- Avoid liberal FFP/platelet transfusion — worsens portal pressure without proven benefit[1]
- Vasopressin — associated with ventricular arrhythmias and sudden death in cirrhotic patients[12]
- Caution with ACE inhibitors/ARBs in cirrhosis[13]
4. Diet
- NPO initially during acute bleed and pending endoscopy
- Early feeding within 72 hours post-endoscopy is recommended[14]
- Sodium restriction (<2 g/day) for patients with ascites[9]
- Adequate protein and calorie intake is critical — malnutrition is common in cirrhosis; nutritionist involvement recommended[9]
- Alcohol abstinence is essential regardless of cirrhosis etiology[9]
5. Review of Systems
- GI: hematemesis, melena, hematochezia, abdominal distension, nausea/vomiting
- Neuro: confusion, asterixis, somnolence (hepatic encephalopathy)
- Cardiopulmonary: dyspnea, chest pain, orthopnea (cirrhotic cardiomyopathy, hepatopulmonary syndrome)
- Renal: decreased urine output (hepatorenal syndrome)
- Constitutional: fatigue, weight loss, anorexia, muscle cramps (64% prevalence in cirrhosis), pruritus (39%)[9]
6. Collateral History and Family History
- Alcohol use history (quantity, duration, last drink) — most important collateral
- Prior liver disease diagnosis, prior endoscopy findings, prior TIPS placement
- Medication compliance (beta-blockers, lactulose)
- Family history of liver disease (hemochromatosis, Wilson disease, alpha-1-antitrypsin deficiency)
- Social context: housing stability, caregiver availability, ability to follow up
7. Risk Factors
- Cirrhosis of any etiology (alcohol, viral hepatitis B/C, NAFLD, autoimmune)[1]
- Child-Pugh class B or C — independent predictor of variceal bleeding and mortality[15-16]
- Large variceal size and red wale signs on endoscopy[1]
- HVPG ≥12 mmHg (threshold for variceal bleeding)[1]
- Thrombocytopenia (platelets <110 × 10⁹/L) — associated with CSPH and variceal bleeding risk[9]
- Active alcohol use, non-compliance with beta-blocker prophylaxis
- Hepatocellular carcinoma, portal vein thrombosis
- H. pylori infection (OR 7.36 for variceal bleeding in one study)[15]
- Prior variceal bleeding episode (highest risk factor for rebleeding)
8. Differential Diagnosis
- Esophageal variceal hemorrhage (most common portal hypertensive source, ~70% of UGIB in cirrhosis)[2]
- Gastric variceal hemorrhage — often more massive and harder to control endoscopically[6]
- Peptic ulcer disease — present in ~38% of cirrhotic patients with UGIB; distinguished by melena-predominant presentation[4]
- Portal hypertensive gastropathy — diffuse mucosal oozing
- Mallory-Weiss tear — post-retching, typically self-limited
- Gastric/esophageal malignancy
- Ectopic varices (duodenal, rectal, stomal) — consider if EGD is negative[17]
- Dieulafoy lesion
- Aortoenteric fistula (in patients with prior aortic graft — cannot miss)
9. Past Medical History
- Prior variceal bleeding episodes and treatments (EVL, sclerotherapy, TIPS)
- Cirrhosis etiology and duration, Child-Pugh class, MELD score
- History of ascites, SBP, hepatic encephalopathy, hepatorenal syndrome
- Hepatocellular carcinoma screening status
- Portal vein thrombosis
- Cardiac disease (cirrhotic cardiomyopathy, coronary artery disease — affects transfusion threshold)
- Coagulopathy history
10. Physical Exam
Vital signs
- Tachycardia, hypotension, orthostatic changes, tachypnea
- Stigmata of chronic liver disease (specificity >90% for cirrhosis):[9][18]
- Spider angiomas, palmar erythema, Terry nails
- Jaundice/scleral icterus
- Gynecomastia, testicular atrophy, decreased body hair
- Caput medusae, parotid enlargement (alcohol-related)
- Dupuytren contracture (alcohol use, not cirrhosis per se)
Abdominal exam
- Ascites (shifting dullness — 83% sensitivity, 56% specificity)[9]
- Splenomegaly (palpable spleen suggests portal hypertension)
- Hepatomegaly (early) vs. shrunken liver (advanced cirrhosis)
Neurologic
- Asterixis, disorientation, lethargy (hepatic encephalopathy — West Haven criteria)
Rectal exam
- Melena, hematochezia, or occult blood
11. Lab Studies
- CBC: hemoglobin (transfusion threshold ~7 g/dL), platelet count (thrombocytopenia suggests portal hypertension)[1]
- BMP: creatinine (hepatorenal syndrome, MELD calculation), BUN, electrolytes, sodium (hyponatremia common)
- LFTs: AST, ALT, bilirubin, albumin (Child-Pugh and MELD components)
- Coagulation: PT/INR — note that INR does not reliably predict hemostatic dysfunction in cirrhosis[1]
- Type and crossmatch: at least 2–4 units pRBCs
- Lactate: marker of tissue hypoperfusion
- Blood cultures: if infection suspected
- Ammonia: if encephalopathy present
- Fibrinogen: may be low in advanced liver disease
- Do NOT transfuse FFP based on INR targets — no evidence of benefit and potential harm from volume overload and worsening portal pressure[1]
12. Imaging
- Bedside POCUS: assess for ascites, splenomegaly, portal vein diameter (>12 mm suggests portal hypertension), portal vein flow velocity[19-20]
- CT abdomen with contrast (once stable): evaluate for portal vein thrombosis, hepatocellular carcinoma, portosystemic collaterals, vascular anatomy for potential TIPS[1][21]
- Doppler ultrasound: portal vein patency and flow direction (hepatopetal vs. hepatofugal)[17]
- CXR: rule out aspiration pneumonia (most common infection in variceal bleeding admissions)[1]
- Imaging is NOT required before initiating treatment — do not delay resuscitation or vasoactive therapy
13. Special Tests
Scoring systems
- Child-Pugh Score: best predictor of in-hospital outcome (AUC 0.9); CTP >7 associated with 19.8% vs. 0.9% mortality[22]
- MELD Score: MELD ≥19 predicts ≥20% 6-week mortality; MELD <11 predicts <5% mortality[23]
- Glasgow-Blatchford Score (GBS): useful for initial risk stratification of UGIB; GBS of 0 identifies patients safe for outpatient management (though rarely applicable in variceal bleeding)[22][24]
- AIMS65: excellent discrimination for in-hospital mortality in variceal bleeding (AUC >0.8)[25]
Point-of-care
- POCUS portal vein assessment — SCoPE score (splenomegaly, coagulopathy, portal vein flow velocity) has AUC 0.843 for predicting variceal etiology[19]
- Fibrosis scores (FIB-4, APRI) can help predict variceal etiology in undifferentiated UGIB[19][26]
Endoscopy
14. ECG
- QTc prolongation present in ~25% of cirrhotic patients — associated with cirrhotic cardiomyopathy and worsening Child-Pugh class[27]
- Monitor for electrolyte-driven arrhythmias (hypokalemia, hypomagnesemia from diuretics, massive transfusion)
- Ventricular arrhythmias reported with vasopressin use — avoid vasopressin; use octreotide instead[12]
- Obtain ECG to evaluate for demand ischemia/myocardial injury — troponin elevation occurs in ~36% and independently predicts mortality[7]
- Sinus tachycardia is expected with hemorrhage; new arrhythmias warrant further evaluation
15. Assessment
- Severity stratification is driven by Child-Pugh class and MELD score:[16][28]
- Child-Pugh A / MELD ≤11: low mortality (2–4%)
- Child-Pugh B / MELD 12–18: intermediate mortality (10–12%)
- Child-Pugh C / MELD ≥19: high mortality (22–46%) — consider early/preemptive TIPS
- Typical presentation is acute hematemesis with bright red blood in a patient with known or suspected cirrhosis. Atypical presentations include isolated melena, syncope, or worsening encephalopathy without overt bleeding. Complications include aspiration pneumonia, hepatorenal syndrome, SBP, hepatic encephalopathy, rebleeding (20% in-hospital), and multiorgan failure.[1][4]
16. Treatment Plan
Initial stabilization (ED)
- Airway: intubate only if necessary (massive hematemesis, altered mental status, aspiration risk) — intubation itself increases mortality; extubate as soon as safely possible[1][24]
- Two large-bore IVs, avoid aggressive crystalloid resuscitation (worsens portal pressure)
- Restrictive transfusion: target Hgb ~7 g/dL (8 g/dL if active coronary disease)[1]
- Start octreotide immediately: 50 mcg IV bolus → 25–50 mcg/hr drip[1]
- Start ceftriaxone 1 g IV q24h[1]
- Erythromycin 125–250 mg IV 30–120 min pre-endoscopy[1]
Endoscopic therapy
- EGD within 12 hours[1]
- Esophageal varices: endoscopic variceal ligation (EVL) — success rate ~89%[1][4]
- Gastric varices: cyanoacrylate glue injection ± coil embolization (success 87–100%); EVL less effective for gastric varices[1]
Refractory bleeding
- Balloon tamponade (Sengstaken-Blakemore or Minnesota tube) or self-expanding metal stent as bridge to definitive therapy[1][14]
- Preemptive TIPS within 72 hours (ideally 24 hours) for high-risk patients: Child-Pugh B >7 with active bleeding at endoscopy, or Child-Pugh C 10–13 — improved 1-year survival (86% vs. 61%)[1][9]
Post-endoscopy
- Continue octreotide drip for 2–5 days[1]
- Continue antibiotics for up to 5 days[1]
- Initiate NSBB (carvedilol preferred) at discontinuation of vasoactive therapy[1]
- Repeat EVL every 2–4 weeks until variceal obliteration[1]
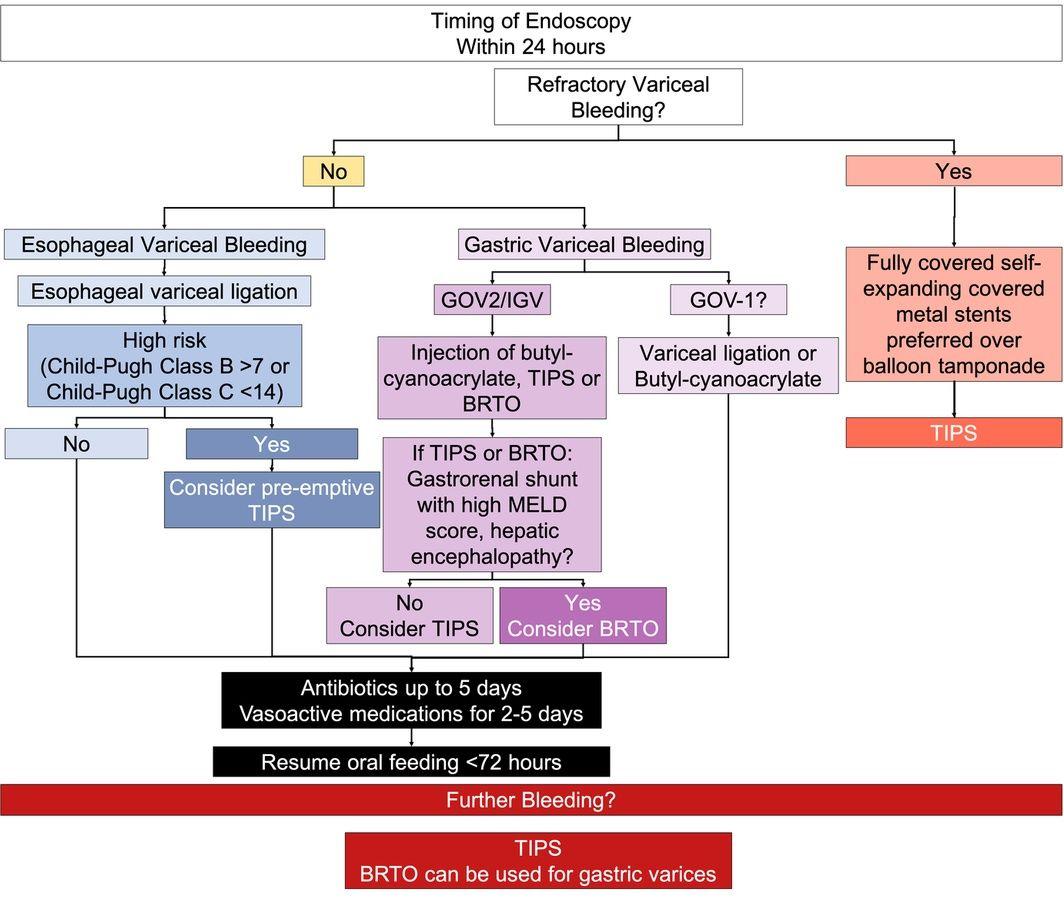
- The following figure summarizes the endoscopic and post-endoscopic management algorithm:
- View full figure Figure 3. Endoscopic management and post‐endoscopic management for patients with acute upper gastrointestinal bleeding from varices. Review article: Upper gastrointestinal bleeding – review of current evidence and implications for management. Aliment Pharmacol Ther. April 30, 2024.
17. Disposition
Admission criteria (all variceal bleeds require admission)
- ICU admission for hemodynamic instability, active bleeding, need for intubation, or high-risk features (Child-Pugh C, MELD ≥19)[1][8]
- Step-down/monitored bed for stable patients after successful endoscopic hemostasis
Specialist consultation triggers
- GI/Hepatology: all cases — for urgent endoscopy and ongoing management
- Interventional radiology: for TIPS evaluation in high-risk patients or refractory bleeding[1]
- Surgery: rarely needed; consider if all other modalities fail
- Transplant hepatology: evaluate for liver transplant candidacy during admission
Discharge criteria
- Hemodynamically stable for ≥24 hours
- No evidence of rebleeding
- Tolerating oral intake
- On appropriate secondary prophylaxis (NSBB ± EVL plan)
- Encephalopathy resolved or at baseline
- Reliable follow-up arranged
18. Follow Up / Return Precautions
Follow-up timing
- Repeat EVL every 2–4 weeks until variceal obliteration[1]
- Hepatology follow-up within 1–2 weeks of discharge
- Liver transplant evaluation if appropriate
- Variceal screening endoscopy: annually if decompensated, every 2–3 years if compensated[9]
- Return precautions — instruct patients to return immediately for:
- Recurrent hematemesis, bloody or black stools
- Lightheadedness, dizziness, or syncope
- Confusion, excessive drowsiness (encephalopathy)
- Fever, abdominal pain, worsening abdominal distension
- Inability to tolerate medications or oral intake
Patient counseling
- Absolute alcohol abstinence
- Medication adherence (beta-blockers, lactulose if prescribed)
- Avoid NSAIDs
- Expected recovery: rebleeding risk is highest in the first 6 weeks (~15–20% 6-week mortality even with optimal therapy)[1-2]
- Ensure understanding of when to activate EMS
References
1. AASLD Practice Guidance on Risk Stratification and Management of Portal Hypertension and Varices in Cirrhosis. — Kaplan DE, Ripoll C, Thiele M, et al. Hepatology. 2024.
2. AGA Clinical Practice Update on the Use of Vasoactive Drugs and Intravenous Albumin in Cirrhosis: Expert Review. — Garcia-Tsao G, Abraldes JG, Rich NE, Wong VW. Gastroenterology. 2024.
3. Management of upper gastrointestinal hemorrhage related to portal hypertension. — Patrick S. Kamath, Louis M. Wong Kee Song Yamada's Textbook of Gastroenterology 7e. 2022.
4. Characteristics of Peptic Ulcer Bleeding in Cirrhotic Patients With Esophageal and Gastric Varices. — Lu Z, Sun X, Han J, et al. Scientific Reports. 2020.
5. Upper Gastrointestinal Bleeding Etiology Score for Predicting Variceal and Non-Variceal Bleeding. — Pongprasobchai S, Nimitvilai S, Chasawat J, Manatsathit S. World Journal of Gastroenterology. 2009.
6. Gastroesophageal Variceal Hemorrhage. — Sharara AI, Rockey DC. The New England Journal of Medicine. 2001.
7. Myocardial Injury Is a Risk Factor for 6-Week Mortality in Liver Cirrhosis Associated Esophagogastric Variceal Bleeding. — Liu B, Li Q, Ding H, et al. Scientific Reports. 2023.
8. The Role of Endoscopy in the Management of Variceal Hemorrhage. — Hwang JH, Shergill AK, Acosta RD, et al. Gastrointestinal Endoscopy. 2014.
9. Diagnosis and Management of Cirrhosis and Its Complications: A Review. — Tapper EB, Parikh ND. The Journal of the American Medical Association. 2023.
10. Management of Acute Upper Gastrointestinal Bleeding. — Stanley AJ, Laine L. BMJ. 2019.
11. Clinical Algorithms for the Prevention of Variceal Bleeding and Rebleeding in Patients With Liver Cirrhosis. — Pfisterer N, Unger LW, Reiberger T. World Journal of Hepatology. 2021.
12. Cirrhotic Cardiomyopathy. — Zardi EM, Abbate A, Zardi DM, et al. Journal of the American College of Cardiology. 2010.
13. Cardiovascular Complications of Cirrhosis. — Møller S, Henriksen JH. Gut. 2008.
14. Review article: Upper gastrointestinal bleeding – review of current evidence and implications for management. — Shung DL, Laine L. Alimentary Pharmacology & Therapeutics. 2024.
15. Clinical Characteristics and Predictors of Esophagogastric Variceal Bleeding Among Patients With HCV-induced Liver Cirrhosis: An Observational Comparative Study. — El Sheref SEDM, Afify S, Berengy MS. PloS One. 2022.
16. Multicenter External Validation of Risk Stratification Criteria for Patients With Variceal Bleeding. — Conejo I, Guardascione MA, Tandon P, et al. Clinical Gastroenterology and Hepatology : The Official Clinical Practice Journal of the American Gastroenterological Association. 2018.
17. Diagnosis and Management of Ectopic Varices in Portal Hypertension. — Tranah TH, Nayagam JS, Gregory S, et al. The Lancet. Gastroenterology & Hepatology. 2023.
18. Liver Cirrhosis. — Ginès P, Krag A, Abraldes JG, et al. Lancet. 2021.
19. A Portal Into Hemodynamics: Utility of Portal Vein Ultrasound in Predicting Variceal Etiology of Upper Gastrointestinal Hemorrhage in the Emergency Department. — Naik S, Ravindra P, Chaudhuri S, et al. Internal and Emergency Medicine. 2025.
20. AASLD Practice Guideline on Noninvasive Liver Disease Assessment of Portal Hypertension. — Sterling RK, Asrani SK, Levine D, et al. Hepatology. 2025.
21. CT Rule-in and Rule-Out Criteria for Clinically Significant Portal Hypertension in Chronic Liver Disease. — Heo S, Lee SS, Choi SH, et al. Radiology. 2023.
22. Child-Pugh Score, MELD Score and Glasgow Blatchford Score to Predict the in-Hospital Outcome of Portal Hypertensive Patients Presenting With Upper Gastrointestinal Bleeding: An Experience From Tertiary Healthcare System. — Jamil Z, Perveen S, Khalid S, et al. Journal of Clinical Medicine. 2022.
23. A MELD-based Model to Determine Risk of Mortality Among Patients With Acute Variceal Bleeding. — Reverter E, Tandon P, Augustin S, et al. Gastroenterology. 2014.
24. Emergency Medicine Updates: Upper Gastrointestinal Bleeding. — Long B, Gottlieb M. The American Journal of Emergency Medicine. 2024.
25. Prognostic Value of Risk Scoring Systems for Cirrhotic Patients With Variceal Bleeding. — Tantai XX, Liu N, Yang LB, et al. World Journal of Gastroenterology. 2019.
26. Prediction of Esophageal Varices and Variceal Hemorrhage in Patients With Acute Upper Gastrointestinal Bleeding. — Rockey DC, Elliott A, Lyles T. Journal of Investigative Medicine : The Official Publication of the American Federation for Clinical Research. 2016.
27. Electrocardiographic characteristics of cirrhotic patients and their association with Child‐Pugh score. — Jahangiri S, Abdiardekani A, Jamshidi S, et al. Clinical Cardiology. 2023.
28. MELD, MELD 3.0, Versus Child Score to Predict Mortality After Acute Variceal Hemorrhage: A Multicenter US Cohort. — Buckholz A, Wong R, Curry MP, et al. Hepatology Communications. 2023.