Urethritis
Urethritis is inflammation of the urethra, classified as gonococcal (caused by Neisseria gonorrhoeae) or nongonococcal (most commonly Chlamydia trachomatis, Mycoplasma genitalium, or Trichomonas va…
Urethritis is inflammation of the urethra, classified as gonococcal (caused by Neisseria gonorrhoeae) or nongonococcal (most commonly Chlamydia trachomatis, Mycoplasma genitalium, or Trichomonas vaginalis).[1-2] It is one of the most common presentations of sexually transmitted infections in the ED and primary care setting. The following is a clinically focused summary organized for rapid decision-making.
1. History
- Discharge characterization: Color (clear/mucoid vs. mucopurulent vs. frankly purulent), volume, timing (morning "glue" vs. constant)
- Dysuria: Onset, severity, internal vs. meatal burning
- Urethral pruritus or irritation without discharge[1-2]
- Timing: Onset relative to last sexual contact; gonococcal urethritis typically presents 2–8 days after exposure, chlamydial urethritis 7–21 days[3]
- Sexual history: Number and gender of partners, new partners, condom use, oral/anal/vaginal contact, transactional sex[4]
- Prior STI history and treatment: Especially recent azithromycin use (raises concern for macrolide-resistant M. genitalium)[2][5]
- Important negatives: Hematuria, flank pain, fever, testicular pain/swelling, joint pain, skin lesions, eye symptoms
2. Alarm Features
- Testicular pain/swelling → epididymitis/orchitis[2][6]
- Fever + polyarthralgia + skin lesions (pustules/petechiae) → disseminated gonococcal infection (DGI)[2-3]
- Tenosynovitis (especially asymmetric, involving wrists/hands) → DGI[2]
- Abdominal pain in female partners → PID risk from untreated infection[7]
- Conjunctivitis → gonococcal autoinoculation or reactive arthritis (Reiter syndrome)[4]
- Urethral stricture symptoms (weak stream, straining) → rare complication of untreated gonococcal urethritis[3]
- Meningismus or new heart murmur → rare gonococcal endocarditis or meningitis[2]
3. Medications
Empiric treatment (etiology unknown)
- Ceftriaxone 500 mg IM × 1 (1,000 mg if >150 kg) PLUS doxycycline 100 mg PO BID × 7 days
Organism-specific regimens
- Export Etiology Recommended Regimen Alternative References N. gonorrhoeae Ceftriaxone 500 mg IM × 1 Cefixime 800 mg PO × 1[1-2]
- C. trachomatis Doxycycline 100 mg PO BID × 7 days Azithromycin 1 g PO × 1[2-3]
- M. genitalium Doxycycline × 7 days → moxifloxacin 400 mg daily × 7 days Resistance-guided azithromycin if macrolide-sensitive[4-5]
- T. vaginalis Metronidazole 2 g PO × 1 (men) Tinidazole 2 g PO × 1[2, 6]
Key medication pearls
- Azithromycin co-treatment for gonorrhea is no longer recommended per 2021 CDC guidelines[7-8]
- Doxycycline is now preferred over azithromycin for chlamydia due to higher microbiologic cure rates[7][10]
- Azithromycin 1 g remains the recommended chlamydia treatment in pregnancy[7]
- Contraindicated: Doxycycline in pregnancy; fluoroquinolones in pregnancy and pediatric patients
4. Diet
- No specific dietary triggers or restrictions
- Encourage adequate hydration to promote urinary flow and comfort
- Advise avoiding alcohol during metronidazole therapy (disulfiram-like reaction)
5. Review of Systems
- GU: Dysuria, discharge, frequency, urgency, hematuria, testicular pain/swelling, pain with ejaculation[4]
- MSK: Joint pain, swelling (DGI, reactive arthritis)[4]
- Derm: Rash, skin lesions (pustules, papules, ulcers)[2]
- Ophthalmologic: Eye redness, discharge (conjunctivitis)[4]
- GI/Anorectal: Rectal pain, discharge, bleeding, tenesmus (proctitis if receptive anal intercourse)[4]
- Constitutional: Fever, chills, malaise (suggests dissemination or ascending infection)
- Oropharyngeal: Sore throat, exudates (pharyngeal gonorrhea)[3]
6. Collateral History and Family History
- Partner notification is critical: Partners should be evaluated and treated; expedited partner therapy (EPT) is permitted in most states[9]
- Ask about partner symptoms (discharge, dysuria, abnormal bleeding)
- Social context: Incarceration, substance use, transactional sex — all increase STI risk[4]
- Family history is generally not contributory, except terminal complement deficiency (hereditary) increases risk of DGI[2]
7. Risk Factors
- Age <25 years[4]
- Multiple or new sexual partners[4]
- Inconsistent condom use[4]
- Men who have sex with men (MSM)[1]
- Prior STI history[4]
- Transactional sex[4]
- Substance use (particularly in MSM)[4]
- M. genitalium specifically more common in younger men, smokers, and those with multiple partners[1]
- T. vaginalis more common in heterosexual men, older age, incarcerated populations, and high-prevalence geographic areas[1-2]
8. Differential Diagnosis
- Urinary tract infection / cystitis — more common in women; culture-positive with uropathogens
- Prostatitis — suprapubic/perineal pain, prostatic tenderness on DRE, LUTS[11]
- Epididymitis — unilateral testicular pain/swelling, positive Prehn sign[6]
- Herpes simplex urethritis — meatitis, genital ulceration, severe dysuria; more common with HSV-1 via oral-genital contact[2]
- Reactive arthritis (Reiter syndrome) — triad of urethritis, conjunctivitis, arthritis[4]
- Urethral foreign body or trauma
- Chemical/irritant urethritis — soaps, spermicides
- Adenoviral urethritis — dysuria, meatitis, conjunctivitis; associated with oral-genital contact[2]
- Non-infectious/idiopathic NGU — accounts for up to ~50% of NGU cases with no identifiable pathogen[2]
9. Past Medical History
- Prior STI episodes and treatments received (especially azithromycin — raises macrolide resistance concern for M. genitalium)[5]
- HIV status — immunosuppression may alter presentation and increase susceptibility
- History of urethral stricture or instrumentation
- Complement deficiency (risk for DGI)[2]
- Use of eculizumab (inhibits terminal complement → increased DGI risk)[2]
10. Physical Exam
- Urethral meatus: Discharge (express if not spontaneously visible — "milking" the urethra), erythema, meatitis[1]
- Inguinal lymph nodes: Lymphadenopathy (consider LGV if tender, unilateral)[4]
- Testicular exam: Tenderness, swelling, epididymal induration (epididymitis)[6]
- Skin: Pustular or petechial acral lesions (DGI), genital ulcers (HSV, syphilis)[2]
- Joints: Tenosynovitis, effusion (DGI, reactive arthritis)[2]
- Oropharynx: Exudates, erythema (pharyngeal gonorrhea)[3]
- Conjunctivae: Injection, discharge[4]
- Rectal exam: If anorectal symptoms present — discharge, tenderness
- The CDC recommends examination of skin, pharynx, lymph nodes, anogenital area, and neurologic system when evaluating for STIs[1]
11. Lab Studies
- NAAT for N. gonorrhoeae and C. trachomatis on first-void urine (preferred specimen in males) — this is the gold standard diagnostic test[1-3]
- Urinalysis: First-void; ≥10 WBC/HPF or positive leukocyte esterase supports diagnosis[1]
- Gram stain of urethral discharge (if available): ≥2 WBC/oil immersion field confirms urethritis; gram-negative intracellular diplococci (GNID) = presumptive gonorrhea[2]
- HIV, syphilis (RPR/VDRL), hepatitis B screening — recommended for all patients with urethritis and STI risk factors[1]
- Hepatitis C screening in MSM and those on PrEP[7]
- **M. genitalium NAAT — reserve for persistent/recurrent NGU, not initial presentation[2]
- **T. vaginalis NAAT — consider in heterosexual men, recurrent urethritis, or high-prevalence areas[1-2]
- Urine culture — not routinely needed; reserve for suspected antimicrobial-resistant gonorrhea or atypical presentations[1]
12. Imaging
- Imaging is generally unnecessary for uncomplicated urethritis
- Scrotal ultrasound if epididymitis or testicular torsion is suspected
- Pelvic ultrasound in female patients with concern for PID/tubo-ovarian abscess
- Joint imaging if DGI with septic arthritis is suspected
13. Special Tests
- Point-of-care NAAT (binx health io CT/NG, Visby Medical Sexual Health Test) — provides same-day results, reduces loss to follow-up and overtreatment[4]
- Gram stain / methylene blue / gentian violet stain of urethral secretions — highly sensitive and specific POC test for confirming urethritis and identifying gonococcal infection[2]
- Macrolide resistance testing for M. genitalium — recommended when available to guide therapy; not yet widely available in the US[2][5]
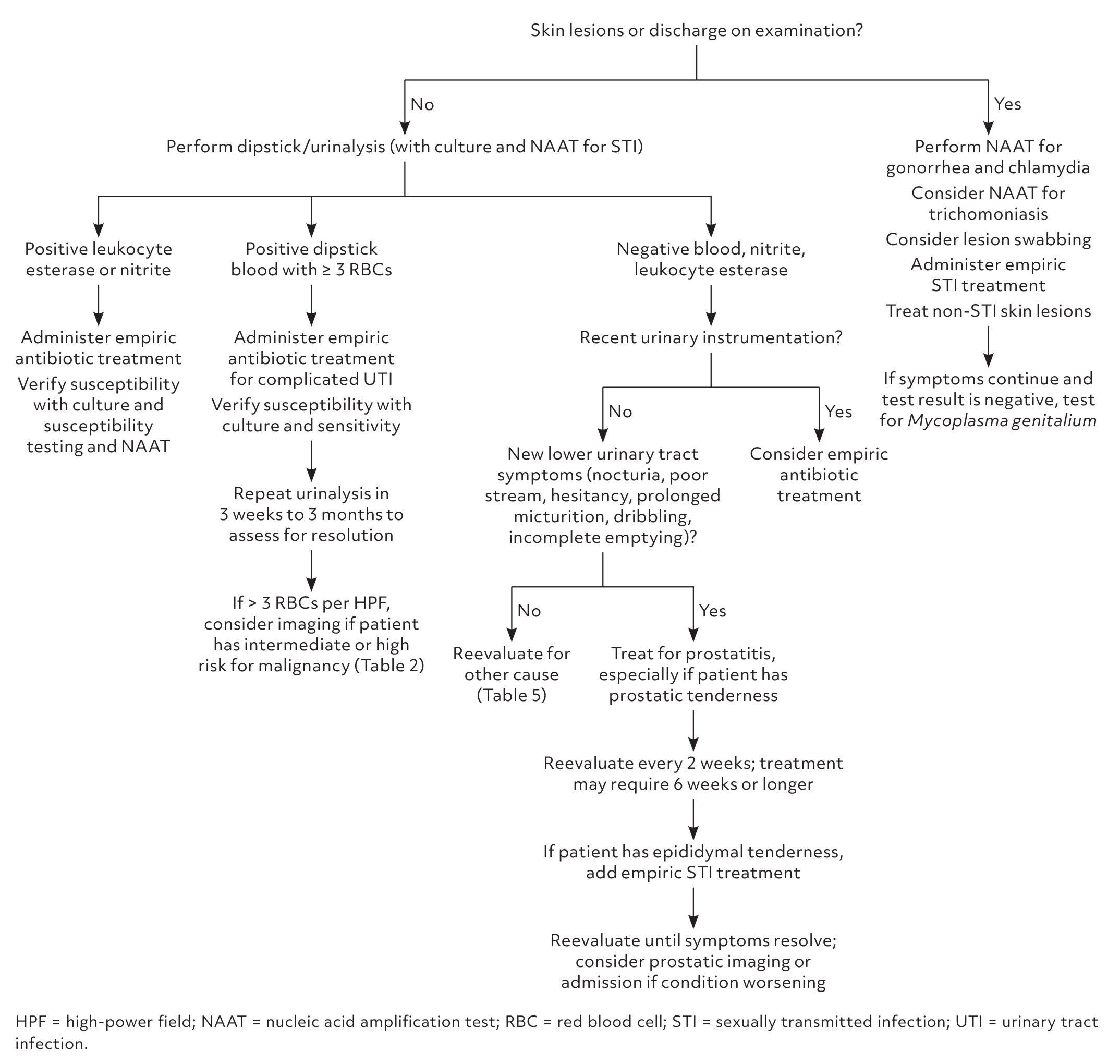
- The following figure illustrates a systematic approach to evaluating dysuria in male patients:
- View full figure Figure 2. Approach to a male with dysuria. Information from references 7, 13, 21, 41, 43, 45, 51–53. Dysuria: Evaluation and Differential Diagnosis in Adults. Am Fam Physician. December 31, 2024.
14. ECG
- Not routinely indicated for uncomplicated urethritis
- Obtain ECG if DGI with suspected endocarditis (new murmur, persistent bacteremia, embolic phenomena)[2]
15. Assessment
- Clinical summary: Urethritis is predominantly an STI-driven condition. N. gonorrhoeae and C. trachomatis account for the majority of cases, with M. genitalium increasingly recognized as a cause of persistent/recurrent NGU (15–25% of NGU cases).[2-3] Approximately 50% of NGU cases remain idiopathic even with comprehensive testing.[2]
Severity stratification
- Uncomplicated: Isolated urethral symptoms, no systemic signs → outpatient management
- Complicated: Epididymitis, prostatitis, DGI, reactive arthritis → escalation of care
Typical vs. atypical presentations
- Gonococcal: Profuse purulent discharge, acute onset 2–8 days post-exposure[3]
- Chlamydial/NGU: Scant mucoid discharge, milder dysuria, may be asymptomatic[1]
- A significant proportion of infections (55–87% of urogenital gonorrhea in men in population-based studies) may be asymptomatic[3]
16. Treatment Plan
Initial management
- Empiric treatment at time of diagnosis — do not wait for NAAT results if clinical suspicion is high:[1-2]
- Ceftriaxone 500 mg IM × 1 + doxycycline 100 mg PO BID × 7 days
- First dose should be directly observed in clinic when possible[2]
- If Gram stain shows no GNID (nongonococcal urethritis): doxycycline 100 mg PO BID × 7 days alone is appropriate[2]
- Persistent/recurrent NGU (symptoms persist after initial treatment):
- Ensure adherence and rule out reinfection (re-exposure)
- Test for M. genitalium (NAAT) and T. vaginalis[2]
- M. genitalium: Doxycycline 100 mg BID × 7 days → moxifloxacin 400 mg daily × 7 days (resistance-guided therapy preferred if available)[2-3]
- T. vaginalis: Metronidazole 2 g PO × 1[1]
- Persistent NGU after M. genitalium and T. vaginalis treatment → refer to ID or urology[2]
Partner management
- All sexual partners within the preceding 60 days should be referred for evaluation and treatment[4]
- Expedited partner therapy (EPT) is an option in most states[9]
17. Disposition
- Discharge (vast majority): Uncomplicated urethritis is managed entirely as an outpatient[1]
Observation/Admission criteria
- Suspected DGI (fever, polyarthralgia, skin lesions, tenosynovitis) → hospitalization and ID consultation recommended[2]
- Suspected gonococcal endocarditis or meningitis[2]
- Inability to tolerate oral medications or concern for nonadherence in complicated cases
Specialist consultation triggers
- Persistent/recurrent NGU after appropriate treatment for M. genitalium and T. vaginalis → ID or urology referral[2]
- Suspected antimicrobial-resistant gonorrhea
- DGI → ID consultation[2]
18. Follow Up / Return Precautions
- Abstain from sexual intercourse for 7 days after single-dose treatment, or until completion of a 7-day course AND symptom resolution AND partner treatment[1][4]
- Repeat testing (test of reinfection): 3 months after treatment, or at first visit within 12 months[1][4]
- Do NOT repeat NAAT <3 weeks after treatment — risk of false-positive results from residual nucleic acid[1]
- Test-of-cure is NOT needed for urogenital gonorrhea but IS recommended for pharyngeal gonorrhea (14 days post-treatment)[7]
- Report gonorrhea and chlamydia to the local health department (both are reportable conditions)[2]
- Return precautions — advise patients to return immediately for:
- Persistent or worsening discharge/dysuria after completing treatment
- Testicular pain or swelling
- Fever, joint pain, or rash
- Eye redness or discharge
- Expected course: Symptoms typically improve within 48–72 hours of appropriate antibiotic therapy. If no improvement, reassess for resistant organisms, alternative diagnoses, or nonadherence.[6]
References
1. Urethritis: Rapid Evidence Review. — Sell J, Nasir M, Courchesne C. American Family Physician. 2021.
2. Sexually Transmitted Infections Treatment Guidelines, 2021. — Workowski KA, Bachmann LH, Chan PA, et al. MMWR. Recommendations and Reports : Morbidity and Mortality Weekly Report. Recommendations and Reports. 2021.
3. Diagnosis and Treatment of Sexually Transmitted Infections: A Review. — Tuddenham S, Hamill MM, Ghanem KG. The Journal of the American Medical Association. 2022.
4. Chlamydial and Gonococcal Infections: Screening, Diagnosis, and Treatment. — Yonke N, Aragón M, Phillips JK. American Family Physician. 2022.
5. Emerging and Reemerging Sexually Transmitted Infections. — Williamson DA, Chen MY. The New England Journal of Medicine. 2020.
6. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
7. Sexually Transmitted Infections: Updates From the 2021 CDC Guidelines. — Dalby J, Stoner BP. American Family Physician. 2022.
8. Management of Neisseria Gonorrhoeae in the United States: Summary of Evidence From the Development of the 2020 Gonorrhea Treatment Recommendations and the 2021 Centers for Disease Control and Prevention Sexually Transmitted Infection Treatment Guidelines. — Barbee LA, St Cyr SB. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2022.
9. Sexually Transmitted Infections: Updated Guideline From the CDC. — Klein DA, Valerio CR, Cofield ZN. American Family Physician. 2022.
10. Diagnosis and Management of Uncomplicated Chlamydia Trachomatis Infections in Adolescents and Adults: Summary of Evidence Reviewed for the 2021 Centers for Disease Control and Prevention Sexually Transmitted Infections Treatment Guidelines. — Geisler WM, Hocking JS, Darville T, Batteiger BE, Brunham RC. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2022.
11. Dysuria: Evaluation and Differential Diagnosis in Adults. — Hoffman A, Dolezal KA, Powell R. American Family Physician. 2025.