Urosepsis
Urosepsis is sepsis originating from a urogenital tract infection, accounting for 9–31% of all sepsis cases, with a mortality of 20–40%.[1] Approximately 80% of cases are due to obstructive uropath…
Urosepsis is sepsis originating from a urogenital tract infection, accounting for 9–31% of all sepsis cases, with a mortality of 20–40%.[1] Approximately 80% of cases are due to obstructive uropathy, with ureterolithiasis being the most common cause.[1-2] The following is a comprehensive clinical summary organized for emergency medicine and primary care workflows.
1. History
- Key HPI questions: Onset and duration of urinary symptoms (dysuria, frequency, urgency, hematuria), flank/back pain, fever/chills/rigors, nausea/vomiting, prior UTIs or urologic procedures
- Symptom characterization: Fever is often high-grade with rigors; flank pain localizes to the upper tract; lower urinary symptoms may or may not be present[3]
- Timing/triggers: Recent urologic instrumentation (cystoscopy, stent placement, PCNL), recent catheterization, recent hospitalization or antibiotic use[2-3]
- Severity/progression: Rapid deterioration from seemingly innocuous UTI symptoms to septic shock can occur within hours[4]
- Associated symptoms: Confusion/altered mental status, oliguria, dyspnea, abdominal pain
- Important negatives: Absence of flank pain does not exclude upper tract source; elderly and immunocompromised patients may present without fever[5]
2. Alarm Features
- Hemodynamic instability: SBP ≤100 mmHg, MAP <65 mmHg, tachycardia
- Altered mental status (GCS <15)[4]
- Respiratory distress: RR ≥22, SpO2 <94%
- Lactate ≥2 mmol/L — defines septic shock when combined with vasopressor requirement[4][6]
- Oliguria/anuria — suggests obstructive uropathy or AKI
- Rigors with high fever (>39°C) or hypothermia (<36°C)
- Signs of DIC: petechiae, oozing from IV sites, thrombocytopenia[7]
- Pyonephrosis or emphysematous pyelonephritis on imaging — surgical emergency[3]
3. Medications
- Empiric IV antibiotics (administer within 1 hour for septic shock, within 3 hours for sepsis without shock):[6]
- First-line empiric options (per IDSA 2025 cUTI guidelines): IV ceftriaxone, piperacillin-tazobactam, or a fluoroquinolone, guided by a 4-step approach: (1) severity of illness, (2) risk factors for resistance, (3) patient-specific considerations, (4) local antibiogram[8]
- If ESBL risk or critically ill: Carbapenems (meropenem 1g IV q8h, ertapenem 1g IV q24h) are preferred[9-10]
- If Enterococcus suspected (indwelling catheter, prior cultures): Add ampicillin or vancomycin
- Avoid: Nitrofurantoin and oral fosfomycin (inadequate tissue/serum levels for systemic infection)[3]
- De-escalate once culture and susceptibility data are available; transition to oral therapy when clinically improving, able to tolerate PO, and an effective oral option exists[11]
- Medications that increase UTI/urosepsis risk: Immunosuppressants, chronic corticosteroids, anticholinergics (urinary retention)
4. Diet
- Acute phase: NPO if hemodynamically unstable or if urologic intervention anticipated
- Hydration: Aggressive IV fluid resuscitation is the priority; oral hydration once stabilized
- Long-term: Adequate fluid intake (≥2L/day) to reduce recurrent UTI/stone risk; dietary modifications based on stone composition if urolithiasis is the underlying cause
5. Review of Systems
- GU: Dysuria, frequency, urgency, hematuria, flank pain, suprapubic pain, urinary retention, penile/vaginal discharge
- Constitutional: Fever, chills, rigors, malaise, night sweats
- GI: Nausea, vomiting, diarrhea, abdominal pain (may mimic intra-abdominal pathology)
- Neurologic: Confusion, lethargy, delirium (especially elderly)
- Respiratory: Dyspnea, tachypnea (may indicate ARDS or metabolic acidosis compensation)
- Skin: Mottling, delayed capillary refill, petechiae
6. Collateral History and Family History
- Collateral: Prior urine culture results and susceptibilities (critical for guiding empiric therapy), recent antibiotic use, recent urologic procedures, baseline mental status, functional status, indwelling devices (Foley, nephrostomy, ureteral stent)[8]
- Family history: Generally not a major factor; however, family history of urolithiasis or polycystic kidney disease may be relevant
- Social context: Nursing home residence (higher MDR risk), ability to comply with outpatient follow-up
7. Risk Factors
- Obstructive uropathy (urolithiasis, BPH, strictures, tumors) — present in ~80% of cases[1-2]
- Urinary catheterization (indwelling or intermittent)[12]
- Diabetes mellitus — 43% higher culture-positive rate[12-13]
- Immunosuppression (transplant, chemotherapy, HIV)
- Chronic kidney disease[12]
- Female sex (higher culture-positive rate in stone-associated urosepsis)[13]
- Advanced age (>65 years)[12]
- Recent urologic instrumentation (cystoscopy, PCNL, TURP, stent exchange)[2]
- Prior antibiotic exposure and healthcare contact (increased MDR risk)[5]
- Structural urinary tract abnormalities (neurogenic bladder, vesicoureteral reflux)
8. Differential Diagnosis
- Pyelonephritis without sepsis — fever + flank pain + pyuria but no organ dysfunction
- Nephrolithiasis (uncomplicated) — colicky flank pain, hematuria, no systemic toxicity
- Intra-abdominal pathology: Acute cholecystitis, appendicitis, diverticulitis, ruptured AAA[3]
- Pelvic inflammatory disease (in women)
- Prostatitis/prostatic abscess (in men)[14]
- Renal abscess or perinephric abscess
- Emphysematous pyelonephritis — a surgical emergency; gas on imaging
- Sepsis from another source with incidental bacteriuria (especially in elderly with asymptomatic bacteriuria)
- Renal vein thrombosis
9. Past Medical History
- Prior UTIs, pyelonephritis, or urosepsis episodes
- History of urolithiasis, BPH, urologic surgery
- Diabetes, CKD, immunosuppression
- Indwelling urinary devices (current or recent)
- Prior urine culture organisms and susceptibilities — the single most useful piece of data for guiding empiric therapy[8]
- Antibiotic allergies (especially beta-lactam, fluoroquinolone)
10. Physical Exam
- Vitals: Temperature (fever >38°C or hypothermia <36°C), HR (tachycardia >90), RR (tachypnea ≥22), BP (hypotension SBP ≤100), SpO2
- General: Toxic appearance, rigors, diaphoresis, altered mental status
- Abdomen: Suprapubic tenderness, distended bladder (retention)
- Flank: CVA tenderness — hallmark of upper tract involvement[3][15]
- GU: Examine for phimosis, urethral discharge, scrotal pathology (epididymitis/orchitis), vaginal discharge
- Rectal (men): Prostate tenderness/boggy prostate (prostatitis/abscess)
- Skin: Mottling, petechiae, delayed capillary refill (>3 seconds), check catheter sites
- Extremities: Peripheral perfusion, edema
11. Lab Studies
- CBC with differential: Leukocytosis (>12,000) or leukopenia (<4,000), bandemia, thrombocytopenia[5]
- BMP/CMP: Creatinine (AKI), BUN, electrolytes (hyperkalemia in AKI), glucose (hyperglycemia common in sepsis)
- Lactate: ≥2 mmol/L associated with tissue hypoperfusion; serial lactate to guide resuscitation[6]
- Procalcitonin: Elevated in bacterial sepsis; useful for risk stratification (≥0.5 ng/mL suggests systemic infection)[16-17]
- CRP: Elevated; nonspecific but useful for trending
- Coagulation studies: PT/INR, fibrinogen, D-dimer (DIC screening)[16]
- LFTs: Elevated aminotransferases in sepsis-related organ dysfunction[7]
- Blood cultures: 2 sets (aerobic + anaerobic) from separate sites before antibiotics[18]
- Urinalysis + urine culture: Pyuria, bacteriuria, nitrites; culture for organism identification and susceptibilities[18-19]
- Blood gas (VBG/ABG): Metabolic acidosis, lactate
12. Imaging
- First-line: Renal/bladder ultrasound — rapid, bedside, identifies hydronephrosis, pyonephrosis, bladder distension, renal abscess[1][14]
- Gold standard: CT abdomen/pelvis with contrast — indicated for sepsis, suspected obstruction, abscess, emphysematous pyelonephritis, or failure to improve[3][18]
- Key findings: Hydronephrosis, perinephric stranding, ureteral calculi, gas within renal parenchyma (emphysematous pyelonephritis), abscess
- When imaging is unnecessary: Uncomplicated pyelonephritis in a young, otherwise healthy patient responding to antibiotics[3]
- CT KUB (non-contrast): Adequate for stone detection but misses abscess and soft tissue detail
13. Special Tests
Scoring systems
- SOFA score (≥2 points = sepsis) — the standard for defining sepsis per Sepsis-3[4][8]
- qSOFA (≥2 of: altered mentation, SBP ≤100, RR ≥22) — screening tool, but the Surviving Sepsis Campaign 2026 guidelines recommend NEWS, NEWS2, MEWS, or SIRS over qSOFA as a single screening tool[20]
- Point-of-care ultrasound (POCUS): Assess for hydronephrosis, IVC collapsibility (volume status), cardiac function
- Bladder scan: Post-void residual to assess for urinary retention
- Urine Gram stain: Rapid identification of gram-negative vs. gram-positive organisms to guide initial therapy
14. ECG
- Indications: All septic patients, especially those with tachycardia, hypotension, chest pain, or elderly patients
Common findings in sepsis
- Sinus tachycardia (39% of sepsis patients)[21]
- QT prolongation (54% of sepsis patients) — associated with poor outcomes[21]
- Atrial fibrillation/flutter (8.8%) — new-onset AF associated with 2.2× higher odds of poor outcomes[21]
- ST changes — may mimic ACS; sepsis-related myocardial dysfunction can cause ST elevation with reciprocal changes even without coronary occlusion[22]
- Decreased QRS amplitude in septic shock[23]
- Electrolyte-related changes: Hyperkalemia (peaked T waves, widened QRS) in AKI; hypokalemia (U waves, ST depression) from fluid resuscitation[24-25]
15. Assessment
Severity stratification (per Sepsis-3 definitions)
- Sepsis: Suspected UTI + SOFA ≥2 (life-threatening organ dysfunction)
- Septic shock: Sepsis + vasopressor requirement to maintain MAP ≥65 mmHg + lactate >2 mmol/L despite adequate fluid resuscitation
- Typical presentation: Elderly patient with obstructive uropathy (stone, BPH) presenting with fever, rigors, flank pain, and hemodynamic instability. E. coli is the causative organism in ~50–65% of cases.[4][13]
- Atypical presentations: Elderly or immunocompromised patients may present with confusion, hypothermia, or nonspecific decline without localizing urinary symptoms.[5]
- Complications: AKI, ARDS, DIC, septic shock, multi-organ failure, septic cardiomyopathy, critical illness polyneuropathy.[7]
16. Treatment Plan
Initial stabilization (Hour-1 Bundle)
- IV access (2 large-bore IVs), continuous monitoring
- Fluid resuscitation: Balanced crystalloid (LR preferred), 500–2,000 mL (up to ~30 mL/kg) for hypotension/hypoperfusion; reassess frequently with dynamic measures[6][18]
- Blood cultures × 2 sets + urine culture before antibiotics[18]
- Lactate measurement[6]
- Empiric IV antibiotics within 1 hour if septic shock, within 3 hours if sepsis without shock[6]
Antibiotic selection (IDSA 2025 four-step approach)
- Non-septic, low risk for resistance: Ceftriaxone 2g IV q24h or fluoroquinolone
- Septic, no MDR risk factors: Piperacillin-tazobactam 4.5g IV q6h or cefepime 2g IV q8h
- Septic with MDR risk factors (prior ESBL, recent antibiotics, healthcare exposure): Meropenem 1g IV q8h[9-10]
- Enterococcal coverage if indicated: Add ampicillin 2g IV q4h or vancomycin
Vasopressors
- Norepinephrine is first-line if hypotension persists after initial fluid resuscitation; target MAP ≥65 mmHg[6][18]
- May be started via peripheral IV or IO without central access[18]
Source control — CRITICAL in urosepsis
- Obstructing stone with infection: Urgent decompression via percutaneous nephrostomy (PCN) or retrograde ureteral stent (RUS) — both are effective; choice depends on clinical scenario and available expertise[26][28-29]
- PCN may be preferred in pyonephrosis or when larger drainage is needed[28][30]
- Definitive stone treatment should be deferred until sepsis resolves[26]
- Infected indwelling catheter: Remove and replace if needed[18]
- Abscess: Percutaneous or surgical drainage
- IV-to-oral transition: Once clinically improving, tolerating PO, and an effective oral option is available (fluoroquinolone, TMP-SMX, or oral cephalosporin based on susceptibilities)[11]
- Duration: Typically 7–14 days depending on source control and clinical response; shorter courses (7 days) are increasingly favored when source control is adequate[5]
17. Disposition
- Admission criteria (most urosepsis patients require admission):
- Sepsis or septic shock (ICU admission within 6 hours if ICU-level care needed)[6][20]
- Hemodynamic instability or vasopressor requirement → ICU
- Obstructive uropathy requiring urgent intervention
- Inability to tolerate oral medications (persistent vomiting)
- Significant comorbidities (CKD, immunosuppression, diabetes with poor control)
- AKI, multi-organ dysfunction
Observation indications
- Moderate illness without shock, responding to initial IV fluids and antibiotics, pending imaging results
- Discharge criteria (rare in true urosepsis; more applicable to uncomplicated pyelonephritis):
- Hemodynamically stable, afebrile, tolerating PO, no obstruction, reliable follow-up[3]
Specialist consultation triggers
- Urology: All cases with obstructive uropathy, stones, abscess, emphysematous pyelonephritis, or need for source control[27]
- Interventional radiology: PCN placement if urology unavailable or antegrade approach preferred[30]
- Infectious disease: MDR organisms, failure to improve on empiric therapy, immunocompromised host
- Critical care/ICU: Septic shock, vasopressor requirement, multi-organ dysfunction
18. Follow Up / Return Precautions
- Follow-up timing: PCP or urology within 1–2 weeks of discharge; earlier if persistent symptoms
- Repeat urine culture: Consider test of cure in complicated cases or if structural abnormality persists
- Definitive stone management: Schedule after infection clears (typically 4–6 weeks) if urolithiasis was the cause[26]
- Review culture susceptibilities and narrow/adjust oral antibiotics accordingly
- Return precautions — instruct patients to return immediately for:
- Recurrent fever, rigors, or chills
- Worsening flank or abdominal pain
- Decreased urine output or inability to urinate
- Confusion, lightheadedness, or feeling faint
- Persistent vomiting or inability to take medications
- Blood in urine (new or worsening)
- Expected recovery: With appropriate antibiotics and source control, clinical improvement is typically seen within 48–72 hours. Failure to improve should prompt re-imaging for undrained collection, reassessment of antibiotic coverage, and consideration of alternative diagnoses.[1][27]
- Relevant images 4 items
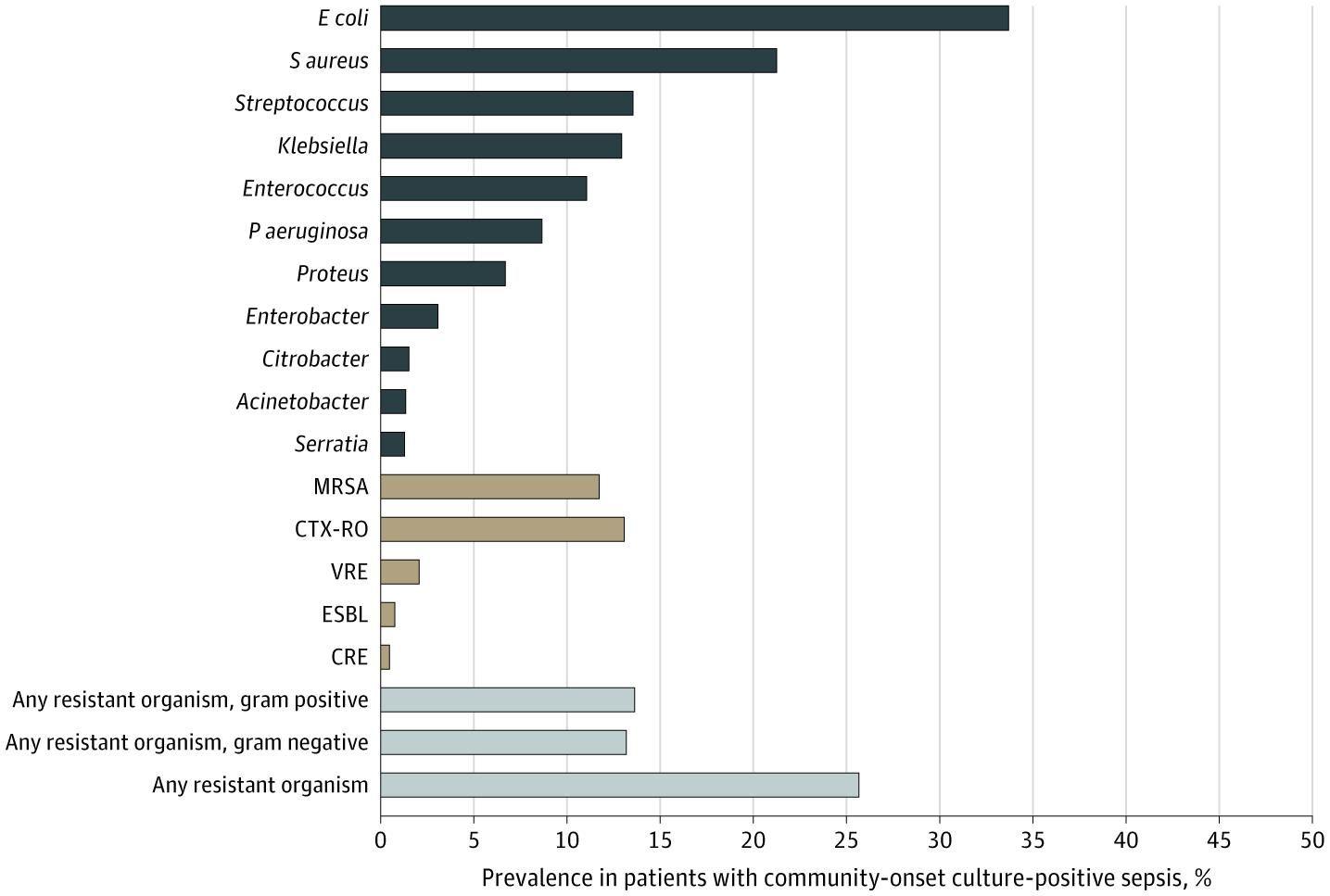
- Prevalence of Pathogens in Culture-Positive Community-Onset Sepsis
- JAMA Netw Open March 31, 2020
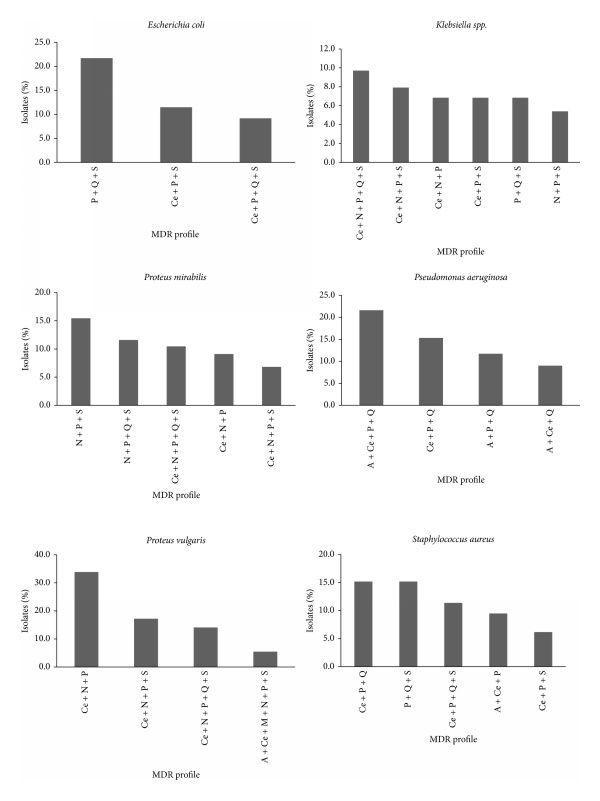
- Variation of the MDR profiles in the main bacteria implicated in UTI during the study period.
- BioMed Research International January 14, 2015
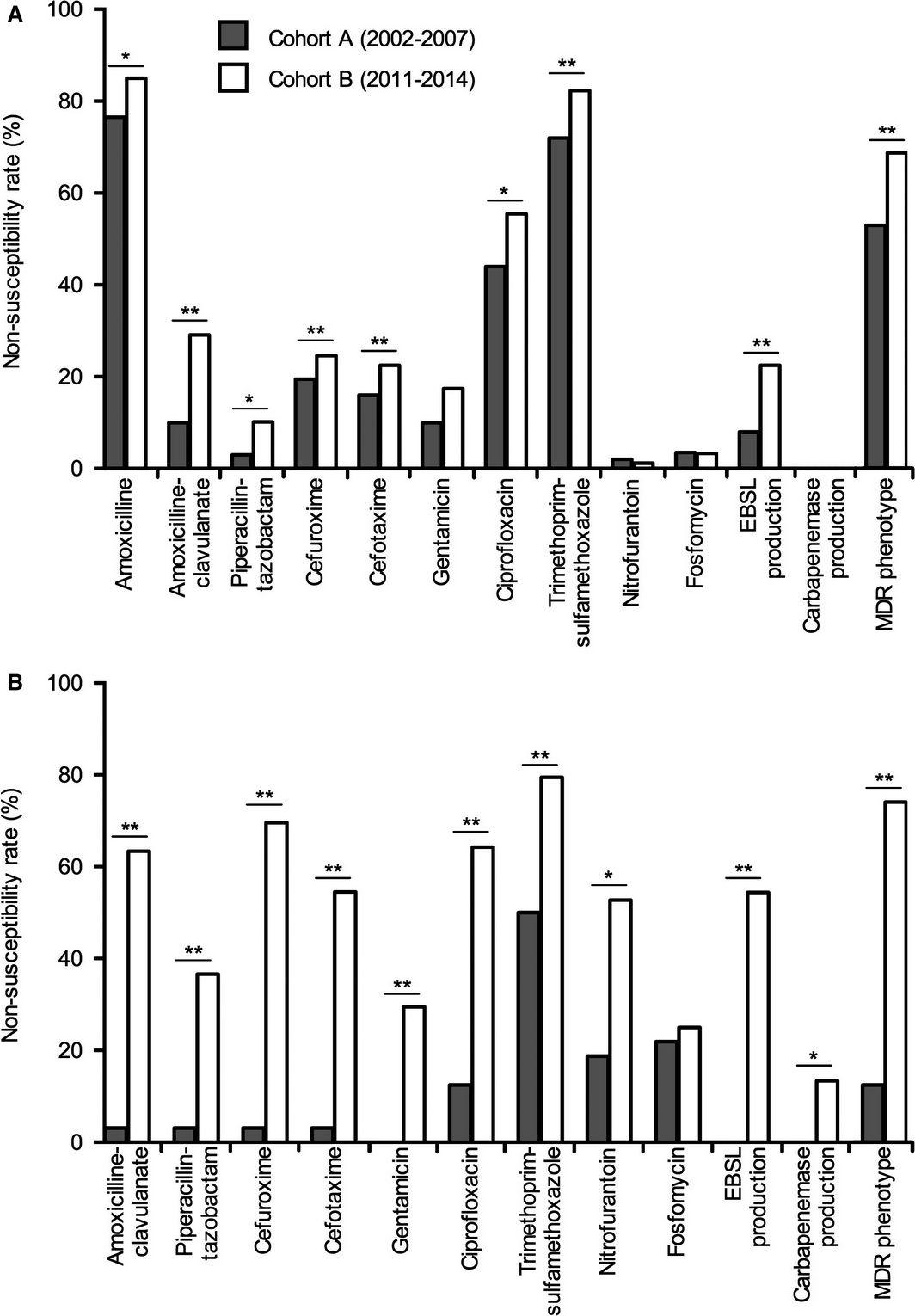
- Non‐susceptibility rates to specific agents and proportion of ESBL ‐producing, carbapenemase‐producing, and MDR isolates in (A) E scherichia coli and (B) K lebsiella pneumoniae according to study cohort.
- Transplant Infectious Disease July 31, 2016
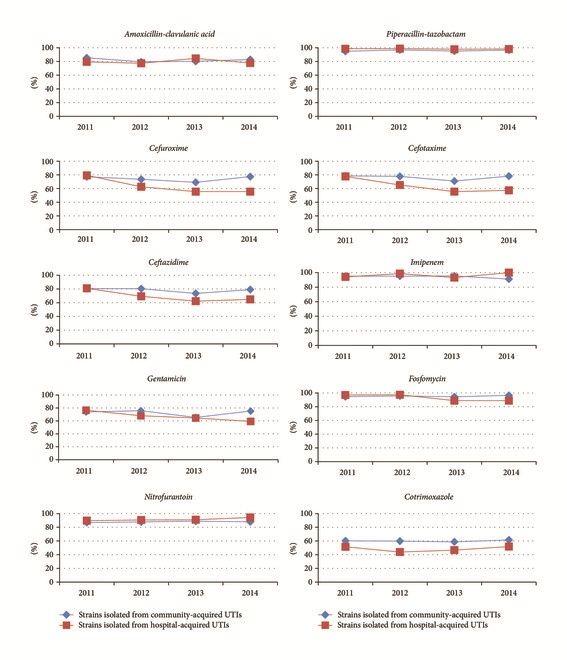
- Activity (in %) of the different antibiotics against all bacteria isolated in urine samples during 2011–2014.
- BioMed Research International January 15, 2017
References
1. Urosepsis--Etiology, Diagnosis, and Treatment. — Dreger NM, Degener S, Ahmad-Nejad P, Wöbker G, Roth S. Deutsches Arzteblatt International. 2015.
2. Urosepsis: Overview of the Diagnostic and Treatment Challenges. — Wagenlehner FME, Pilatz A, Weidner W, Naber KG. Microbiology Spectrum. 2015.
3. Acute Pyelonephritis in Adults. — Johnson JR, Russo TA. The New England Journal of Medicine. 2018.
4. Clinical Situations of Bacteriology and Prognosis in Patients with Urosepsis. — Jiang Y, Li J, Zhang Y, et al. BioMed Research International. 2018.
5. Sepsis and Septic Shock. — Meyer NJ, Prescott HC. The New England Journal of Medicine. 2024.
6. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2021. — Evans L, Rhodes A, Alhazzani W, et al. Critical Care Medicine. 2021.
7. Severe Sepsis and Septic Shock. — Angus DC, van der Poll T. The New England Journal of Medicine. 2013.
8. Clinical Practice Guideline by Infectious Diseases Society of America (IDSA): 2025 Guideline on Management and Treatment of Complicated Urinary Tract Infections: Selection of Antibiotic Therapy for Complicated UTI. — Barbara W. Trautner, Nicolás W. Cortés-Penfield, Kalpana Gupta, et al Infectious Diseases Society of America. 2025.
9. Infectious Diseases Society of America 2023 Guidance on the Treatment of Antimicrobial Resistant Gram-Negative Infections. — Tamma PD, Aitken SL, Bonomo RA, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2023.
10. Infectious Diseases Society of America 2024 Guidance on the Treatment of Antimicrobial-Resistant Gram-Negative Infections. — Tamma PD, Heil EL, Justo JA, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
11. Clinical Practice Guideline by Infectious Diseases Society of America (IDSA): 2025 Guideline on Management and Treatment of Complicated Urinary Tract Infections: Timing of Intravenous to Oral Antibiotics Transition for Complicated UTI. — Barbara W. Trautner, Nicolás W. Cortés-Penfield, Kalpana Gupta, et al Infectious Diseases Society of America. 2025.
12. Risk Factors for Urosepsis in Chronic Kidney Disease Patients With Urinary Tract Infections. — Dimitrijevic Z, Paunovic G, Tasic D, Mitic B, Basic D. Scientific Reports. 2021.
13. Pathogen Distribution and Antibiotic Sensitivity Analysis in Urosepsis Associated With Urinary Stones: A Retrospective Observational Study. — Hu Y, Wang X, Chen Y, et al. Medicine. 2025.
14. Urinary Tract Infections in Older Men. — Schaeffer AJ, Nicolle LE. The New England Journal of Medicine. 2016.
15. Urinary Tract Infections in Pregnant Individuals. — Committee on Clinical Consensus—Obstetrics Obstetrics and Gynecology. 2023.
16. Explainable Machine Learning With Routine Biomarkers Identifies Culture-Defined Bacteremic Urosepsis. — Zhang YL, Yu DX, Zheng YY, et al. Scientific Reports. 2026.
17. A Reference Standard for Urinary Tract Infection Research: A Multidisciplinary Delphi Consensus Study. — Bilsen MP, Conroy SP, Schneeberger C, et al. The Lancet. Infectious Diseases. 2024.
18. Early Care of Adults With Suspected Sepsis in The Emergency Department and Out-of-Hospital Environment: A Consensus-Based Task Force Report. — Yealy DM, Mohr NM, Shapiro NI, et al. Annals of Emergency Medicine. 2021.
19. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
20. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026. — Prescott HC, Antonelli M, Alhazzani W, et al. Critical Care Medicine. 2026.
21. Association of Electrocardiogram Abnormalities With Clinical Outcomes in Emergency Department Sepsis Patients. — Kotruchin P, Chuehongthong M, Tangpaisarn T, et al. The Western Journal of Emergency Medicine. 2026.
22. Emphysematous Pyelonephritis With ST Elevation Accompanied by Reciprocal Changes Mimicking Acute Coronary Syndrome. — Hatakeyama K, Shono Y, Hashimoto T, et al. The American Journal of Emergency Medicine. 2023.
23. ECG Changes During Septic Shock. — Rich MM, McGarvey ML, Teener JW, Frame LH. Cardiology. 2002.
24. Update to Practice Standards for Electrocardiographic Monitoring in Hospital Settings: A Scientific Statement From the American Heart Association. — Sandau KE, Funk M, Auerbach A, et al. Circulation. 2017.
25. Electrocardiographic Manifestations: Electrolyte Abnormalities. — Diercks DB, Shumaik GM, Harrigan RA, Brady WJ, Chan TC. The Journal of Emergency Medicine. 2004.
26. 2007 Guideline for the Management of Ureteral Calculi. — Preminger GM, Tiselius HG, Assimos DG, et al. The Journal of Urology. 2007.
27. Diagnosis and Management for Urosepsis. — Wagenlehner FM, Lichtenstern C, Rolfes C, et al. International Journal of Urology : Official Journal of the Japanese Urological Association. 2013.
28. Percutaneous Nephrostomy Versus Retrograde Ureteral Stent for Acute Upper Urinary Tract Obstruction With Urosepsis. — Xu ZH, Yang YH, Zhou S, Lv JL. Journal of Infection and Chemotherapy : Official Journal of the Japan Society of Chemotherapy. 2021.
29. Choosing the Best Way for Urinary Decompression and Developing a Novel Predictive Model for Septic Shock Using SOFA in These Patients. — Law YXT, Shen L, Khor VWS, et al. International Journal of Urology : Official Journal of the Japanese Urological Association. 2022.
30. CIRSE Standards of Practice on Nephrostomy and Ureteric Stent Placement and Exchange. — Ryan AG, Irvine I, Bardgett H, et al. Cardiovascular and Interventional Radiology. 2026.