Vaginitis (Bacterial)
Bacterial Vaginosis (BV)
Bacterial Vaginosis (BV)
Bacterial vaginosis is the most common cause of abnormal vaginal discharge in reproductive-age women, accounting for 40–50% of identified vaginitis cases.[1-2] It represents a vaginal dysbiosis — not a true infection or inflammatory state — characterized by replacement of normal Lactobacillus-dominant flora with anaerobic organisms including Gardnerella vaginalis, Prevotella, Bacteroides, and Atopobium vaginae.[3] It generates approximately 5–10 million office visits annually.[1]
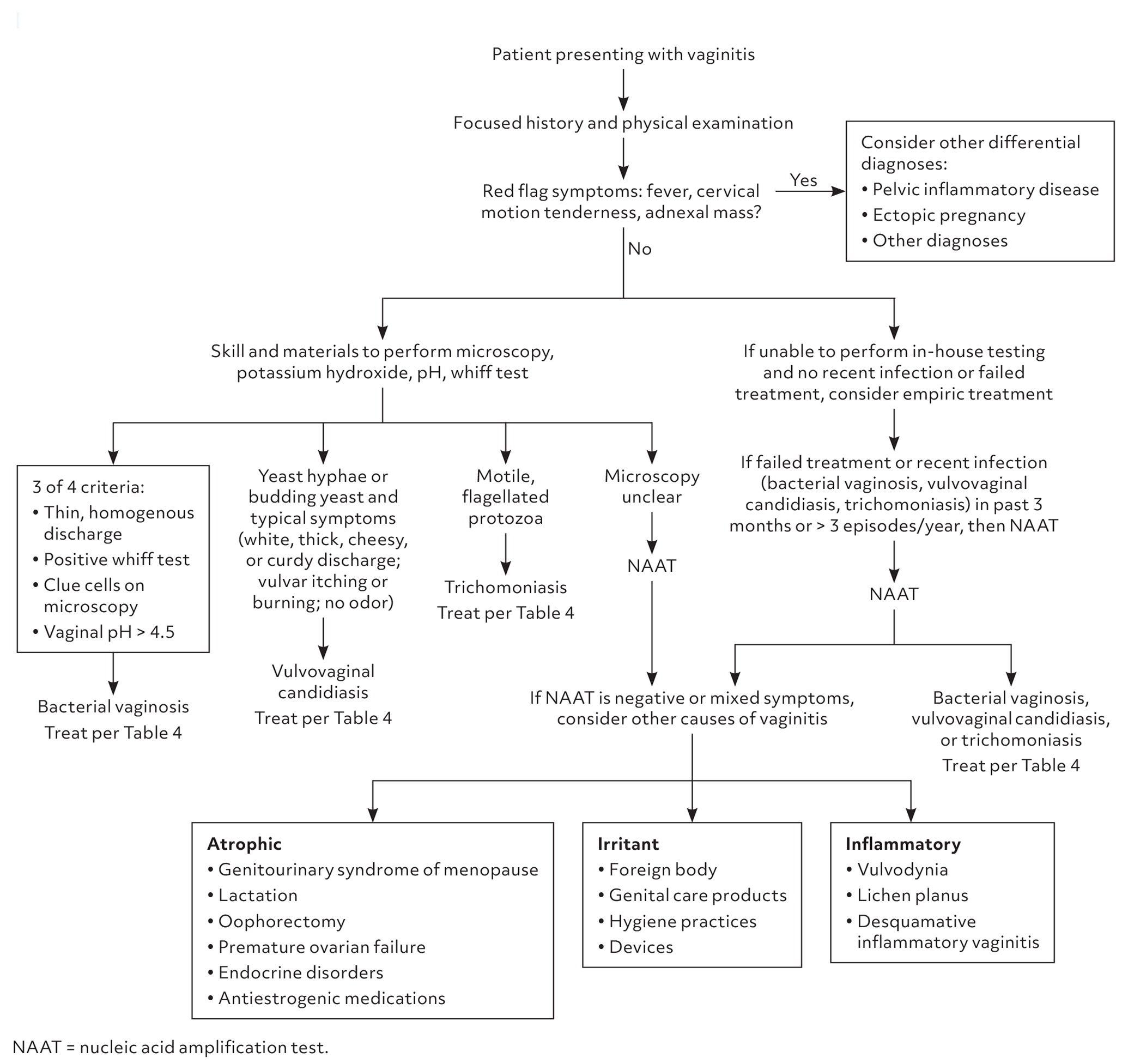
The following diagnostic algorithm from the AAFP provides a practical framework for evaluating vaginal complaints:
View full figure Figure 1. Information from references 2 and 8. Vaginitis: Diagnosis and Treatment. Am Fam Physician. October 31, 2025.
1. History
- Discharge characteristics: Thin, homogeneous, grayish-white discharge that smoothly coats vaginal walls[1][4]
- Odor: "Fishy" amine odor, classically worse after intercourse and during menses[3]
- Timing/triggers: Onset relative to menses, new sexual partner, douching, recent antibiotic use
- Severity/progression: Chronic or recurrent episodes (≥3 documented episodes/year = recurrent BV)[3]
- Associated symptoms: Mild vulvovaginal irritation or burning; significant pruritus is uncommon and suggests candidiasis[1]
- Important negatives: Absence of significant pruritus, dysuria, deep pelvic pain, fever, or purulent discharge helps distinguish BV from other etiologies[5]
2. Alarm Features
- Fever, cervical motion tenderness, adnexal mass/tenderness → consider PID, tubo-ovarian abscess, ectopic pregnancy[1]
- Purulent cervical discharge with WBCs → consider cervicitis (chlamydia, gonorrhea)[6]
- Pregnancy with BV → associated with 2-fold increased risk of preterm birth, PROM, chorioamnionitis, and postpartum endometritis[7-8]
- Bloody or foul-smelling discharge in postmenopausal patients → rule out malignancy, foreign body, atrophic vaginitis
3. Medications
First-line treatment (CDC 2021 / ACOG)
- Metronidazole 500 mg PO BID × 7 days
- Metronidazole gel 0.75% — one applicator (5 g) intravaginally daily × 5 days
- Clindamycin cream 2% — one applicator (5 g) intravaginally at bedtime × 7 days
Alternative regimens
- Secnidazole 2 g PO single dose
- Tinidazole 2 g PO daily × 2 days, or 1 g PO daily × 5 days
- Clindamycin 300 mg PO BID × 7 days
- Clindamycin ovules 100 mg intravaginally at bedtime × 3 days
- Recurrent BV suppression: Metronidazole gel 0.75% twice weekly × 16 weeks after acute treatment[3][9]
Key medication notes
- The CDC 2021 guidelines note that evidence for a disulfiram-like reaction with metronidazole and alcohol is lacking; refraining from alcohol during metronidazole use is considered unnecessary per the CDC, though manufacturers still recommend avoidance[6]
- Clindamycin cream is oil-based and may weaken latex condoms/diaphragms for 5 days after use[6]
- In pregnancy: Oral metronidazole 500 mg BID × 7 days or 250 mg TID × 7 days; tinidazole should be avoided; data insufficient for secnidazole in pregnancy[6]
4. Diet
- No specific dietary triggers are established for BV
- Avoidance of vaginal douching is strongly recommended, as it disrupts normal flora and increases recurrence risk[6]
- Adequate hydration and general nutritional health support immune function
5. Review of Systems
- GU: Vaginal discharge character, odor, dyspareunia, dysuria, urinary frequency
- GYN: Menstrual history, intermenstrual bleeding, postcoital bleeding
- GI: Abdominal/pelvic pain (to rule out PID)
- Constitutional: Fever, chills, malaise (suggests ascending infection)
- Dermatologic: Vulvar rash, lesions, ulcers (to rule out HSV, contact dermatitis)
6. Collateral History and Family History
- Sexual history: Number of partners, new partners, sex of partners (BV occurs in both heterosexual and same-sex female couples), condom use[3]
- Partner symptoms: Emerging evidence supports sexual transmission; the StepUp RCT demonstrated that concurrent male partner treatment (oral metronidazole + topical penile clindamycin × 7 days) reduced BV recurrence from 63% to 35% at 12 weeks[10]
- Hygiene practices: Douching, use of scented products, intrauterine device use
- Family history is not a major contributor, though genetic polymorphisms (e.g., TNF-α SNPs) may modulate risk of BV-associated preterm birth[7]
7. Risk Factors
- Sexual activity (new or multiple partners, female-female sexual contact)[3]
- Douching[3]
- Black, Hispanic, and Mexican American race/ethnicity (higher prevalence)[3]
- IUD use[10]
- Lack of condom use[11]
- Smoking[11]
- Prior history of BV (strongest predictor of recurrence)[3]
- Uncircumcised male partner[10]
8. Differential Diagnosis
- Vulvovaginal candidiasis — thick, white, curd-like discharge; pruritus predominant; pH ≤4.5; KOH shows hyphae/budding yeast[1]
- Trichomoniasis — green/yellow frothy discharge; strawberry cervix; motile trichomonads on wet mount; pH >4.5[1]
- Cervicitis (chlamydia, gonorrhea) — mucopurulent cervical discharge, WBCs on wet mount without clue cells[6]
- Desquamative inflammatory vaginitis — purulent discharge, vaginal erythema, parabasal cells on microscopy[5]
- Atrophic vaginitis — thin, dry mucosa in postmenopausal patients; pH elevated[5]
- Irritant/allergic vaginitis — exposure history to soaps, spermicides, latex[3]
- PID — must-not-miss; fever, CMT, adnexal tenderness[1]
- Foreign body — foul-smelling discharge, often unilateral
9. Past Medical History
- Prior episodes of BV and treatments used (response, recurrence pattern)
- History of STIs (chlamydia, gonorrhea, trichomoniasis, HIV)
- Pregnancy history, prior preterm births
- Recent gynecologic procedures (increased risk of postprocedural infection with BV)[3]
- Chronic conditions: HIV (higher BV prevalence), diabetes
10. Physical Exam
- Vitals: Fever suggests ascending infection (PID, tubo-ovarian abscess)
- External genitalia: Typically normal in BV; erythema/excoriations suggest candidiasis or dermatitis
- Speculum exam: Thin, homogeneous, grayish-white discharge coating vaginal walls; no significant vaginal erythema or inflammation[3-4]
- Cervix: Should appear normal; mucopurulent discharge or friability suggests cervicitis
- Bimanual exam: No cervical motion tenderness or adnexal tenderness (if present, evaluate for PID)
11. Lab Studies
- Vaginal pH >4.5 (sensitivity 97%, specificity 64%)[12]
- KOH whiff test — fishy amine odor with 10% KOH
- Wet mount saline microscopy — clue cells (>20% of epithelial cells); absence of WBCs and trichomonads
- Gram stain with Nugent scoring — reference standard (score 7–10 = BV)[3][6]
- NAAT — available for BV, candida, and trichomoniasis; useful when microscopy is unavailable[1][13]
- STI testing — CDC recommends concurrent testing for HIV and other STIs in patients with BV[3]
- Routine bacterial culture is NOT recommended (G. vaginalis is a commensal in ~50% of healthy women)[3]
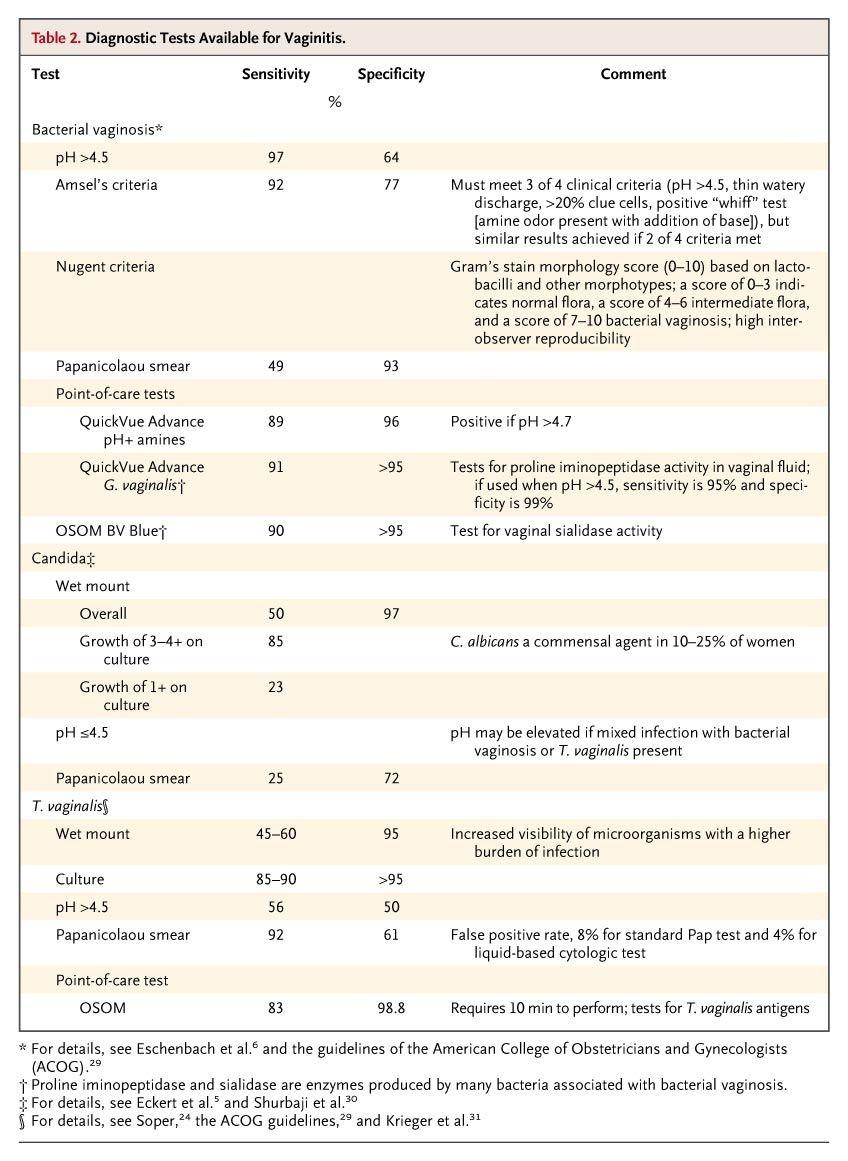
- The following table summarizes diagnostic test performance for vaginitis:
- View full figure Table 2. Diagnostic Tests Available for Vaginitis. Acute Vulvovaginitis. N Engl J Med. September 20, 2006.
12. Imaging
- Not indicated for uncomplicated BV
- Pelvic ultrasound if concern for tubo-ovarian abscess, ectopic pregnancy, or adnexal pathology based on exam findings
13. Special Tests
Amsel Criteria (≥3 of 4 required for diagnosis)
- Thin, homogeneous, white-gray discharge
- Clue cells >20% on saline microscopy
- Vaginal pH >4.5
- Positive KOH whiff test
- Sensitivity 92%, specificity 77% compared to Nugent scoring.[3] Clue cells are the single most reliable indicator.[3]
Point-of-care tests
- OSOM BV Blue (vaginal sialidase activity): sensitivity 90%, specificity >95%
- Affirm VP III (G. vaginalis DNA probe): sensitivity 97% when combined with pH and amine odor
- Multiplex vaginal panels (NAAT-based) — FDA-cleared panels can simultaneously detect BV, candida, and trichomoniasis[13]
14. ECG
- Not applicable for BV
15. Assessment
- BV is a noninflammatory vaginal dysbiosis, not a true infection; it does not cause significant mucosal inflammation[3]
- Approximately 50% of women with BV are asymptomatic[4][14]
- Self-diagnosis is unreliable — ACOG recommends against it due to overlapping symptoms with other causes of vaginitis[3]
- Complications: Increased susceptibility to HIV, HSV-2, chlamydia, gonorrhea, and trichomoniasis; PID; postprocedural gynecologic infections[3][7]
- In pregnancy: 2-fold increased risk of preterm birth (OR 1.76–2.19), PROM (OR 2.59), miscarriage (OR 2.34), and postpartum endometritis[7-8]
- Recurrence is the major clinical challenge: up to 50% recur within 12 months[3][9]
16. Treatment Plan
- Initial treatment — treat symptomatic patients only; asymptomatic screening/treatment is not recommended (USPSTF):[6][15]
- Metronidazole 500 mg PO BID × 7 days (most commonly used)[6]
- Metronidazole gel 0.75% intravaginally daily × 5 days (better GI tolerability)[3]
- Clindamycin cream 2% intravaginally at bedtime × 7 days[6]
Recurrent BV (≥3 episodes/year)
- Extended metronidazole 500 mg BID × 10–14 days
- Followed by suppressive metronidazole gel 0.75% twice weekly × 3–6 months
- Male partner treatment for recurrent BV — the landmark StepUp trial (NEJM 2025) demonstrated that concurrent male partner treatment with oral metronidazole 400 mg BID + topical 2% clindamycin cream to penile skin BID × 7 days reduced BV recurrence from 63% to 35% at 12 weeks (HR 0.37; 95% CI, 0.22–0.61; P<0.001).[10] ACOG now advises considering partner therapy for recurrent BV.[16]
- Pregnancy: Treat all symptomatic pregnant women; oral metronidazole is safe in pregnancy[6]
- Counseling: Avoid douching; use condoms or abstain during treatment; avoid tampons with intravaginal products[3][6]
17. Disposition
- Discharge — the vast majority of BV cases are managed entirely as outpatients
- Admission criteria — only if concurrent PID with systemic toxicity, tubo-ovarian abscess, or inability to tolerate oral medications
Specialist referral
- OB/GYN for recurrent BV refractory to suppressive therapy
- Infectious disease if concern for resistant organisms or complex coinfections
- MFM if pregnant with recurrent BV and history of preterm birth
18. Follow Up / Return Precautions
- Routine follow-up/test of cure is not necessary if symptoms resolve[3]
- Retest within 3 months if symptoms recur (recurrence rate up to 30% at 3 months)[3]
Return precautions — advise patients to return for
- Persistent or worsening symptoms after completing treatment
- New fever, pelvic pain, or abnormal bleeding (concern for PID)
- Recurrent episodes (≥3/year warrants suppressive therapy discussion)
- Expected course: Symptoms typically improve within 2–3 days of starting treatment; full resolution by end of therapy
- Patient counseling: BV is not a classic STI but is associated with sexual activity; partner treatment may be discussed for recurrent cases; avoid douching; complete full course of antibiotics
References
1. Vaginitis: Diagnosis and Treatment. — Geer K, Klega A. American Family Physician. 2025.
2. Vaginitis: Diagnosis and Treatment. — Paladine HL, Desai UA. American Family Physician. 2018.
3. Vaginitis in Nonpregnant Patients: ACOG Practice Bulletin, Number 215. — Committee on Practice Bulletins—Gynecology Obstetrics and Gynecology. 2020.
4. Fighting polymicrobial biofilms in bacterial vaginosis. — Sousa LGV, Pereira SA, Cerca N. Microbial Biotechnology. 2023.
5. Noncandidal Vaginitis: A Comprehensive Approach to Diagnosis and Management. — Neal CM, Kus LH, Eckert LO, Peipert JF. American Journal of Obstetrics and Gynecology. 2020.
6. Sexually Transmitted Infections Treatment Guidelines, 2021. — Workowski KA, Bachmann LH, Chan PA, et al. MMWR. Recommendations and Reports : Morbidity and Mortality Weekly Report. Recommendations and Reports. 2021.
7. Bacterial Vaginosis and Desquamative Inflammatory Vaginitis. — Paavonen J, Brunham RC. The New England Journal of Medicine. 2018.
8. Systematic Review and Meta-Analysis of Maternal and Fetal Outcomes Among Pregnant Women With Bacterial Vaginosis. — Kenfack-Zanguim J, Kenmoe S, Bowo-Ngandji A, et al. European Journal of Obstetrics, Gynecology, and Reproductive Biology. 2023.
9. Characterization and Treatment of Recurrent Bacterial Vaginosis. — Faught BM, Reyes S. Journal of Women's Health. 2019.
10. Male-Partner Treatment to Prevent Recurrence of Bacterial Vaginosis. — Vodstrcil LA, Plummer EL, Fairley CK, et al. The New England Journal of Medicine. 2025.
11. Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery: US Preventive Services Task Force Recommendation Statement. — US Preventive Services Task Force, Owens DK, Davidson KW, et al. The Journal of the American Medical Association. 2020.
12. Acute Vulvovaginitis. — Eckert LO. The New England Journal of Medicine. 2006.
13. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
14. Screening for Bacterial Vaginosis in Pregnant Adolescents and Women to Prevent Preterm Delivery: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. — Kahwati LC, Clark R, Berkman N, et al. The Journal of the American Medical Association. 2020.
15. Sexually Transmitted Infections: Updates From the 2021 CDC Guidelines. — Dalby J, Stoner BP. American Family Physician. 2022.
16. Advances in Treating Bacterial Vaginosis: Recognizing Sexual Transmission and Pipeline of Therapies. — Kim ES, Waltmann A, Duncan JA, Hood-Pishchany I. Current Opinion in Infectious Diseases. 2026.