Vaginitis (Candidal)
Vulvovaginal Candidiasis (VVC)
Vulvovaginal Candidiasis (VVC)
Vulvovaginal candidiasis is the second most common cause of infectious vaginitis, affecting an estimated 75% of women at least once before menopause and accounting for ~1.4 million annual outpatient visits in the United States.[1-2] Candida albicans is the causative organism in ~90% of cases; non-albicans species (especially C. glabrata) are increasingly recognized.[3-4]
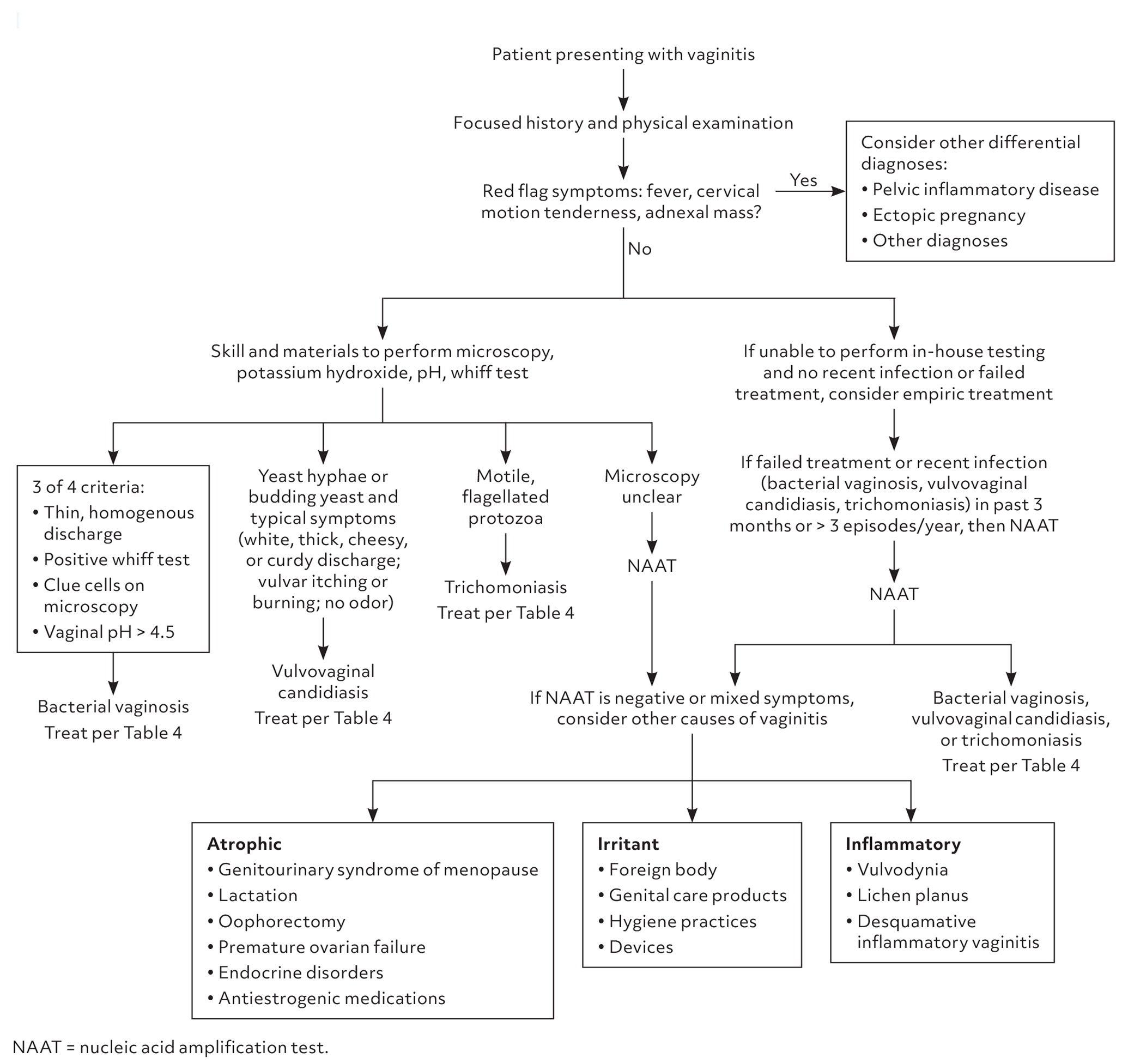
The following diagnostic algorithm from the AAFP provides a practical framework for evaluating vaginitis presentations:
View full figure Figure 1. Information from references 2 and 8. Vaginitis: Diagnosis and Treatment. Am Fam Physician. October 31, 2025.
1. History
- Chief complaint: Vulvovaginal itching, burning, irritation, soreness, external dysuria, dyspareunia[3]
- Discharge character: White, thick, "cottage cheese" or curd-like; typically odorless[5]
- Timing/triggers: Onset relative to menses (often premenstrual flare), recent antibiotic use, new sexual partner, hormonal changes (OCP initiation, pregnancy)
- Severity: Mild intermittent pruritus vs. severe edema/fissuring (suggests complicated VVC)
- Recurrence: ≥4 episodes in 12 months defines recurrent VVC (RVVC) — ask about prior episodes, prior treatments, and response to therapy[3]
- Important negatives: Absence of malodor (argues against BV), absence of frothy discharge (argues against trichomoniasis), no fever or pelvic pain (argues against PID)[5-6]
2. Alarm Features
- Fever, cervical motion tenderness, adnexal mass → consider PID, tubo-ovarian abscess, ectopic pregnancy[5]
- Severe vulvar edema, ulceration, or fissuring → suggests complicated VVC or alternative diagnosis (herpes, Behçet's, vulvar dermatosis)[3]
- Immunocompromised state (HIV with low CD4, uncontrolled diabetes, chronic corticosteroid use) → higher risk for complicated/refractory disease[7-8]
- Failure to respond to appropriate antifungal therapy → consider non-albicans species, azole resistance, or misdiagnosis[6]
3. Medications
Common treatments — Uncomplicated VVC
- Fluconazole 150 mg PO × 1 dose (preferred by most patients)
- Topical azoles: clotrimazole, miconazole, terconazole (OTC or Rx; 1–7 day courses)
- Clinical cure rates >90% with either oral or topical azoles
- Severe acute VVC: Fluconazole 150 mg PO every 72 hours × 2–3 doses[3]
- Recurrent VVC: Induction (10–14 days topical or oral fluconazole), then fluconazole 150 mg weekly × 6 months[3]
- Newer agents: Oteseconazole (FDA-approved 2022 for RVVC in non-reproductive-potential females); ibrexafungerp (FDA-approved for acute and recurrent VVC)[7-9]
- Non-albicans (C. glabrata): Intravaginal boric acid 600 mg daily × 14 days; nystatin suppositories 100,000 units daily × 14 days[3]
- Medication contributors to VVC: Recent antibiotics (especially broad-spectrum), systemic corticosteroids, high-dose estrogen OCPs[4]
Contraindications/cautions
- Fluconazole in pregnancy — associated with spontaneous abortion and craniofacial/cardiac defects; use topical azoles only[8]
- Oteseconazole — contraindicated in women of reproductive potential[9]
- Ibrexafungerp — teratogenic; requires effective contraception during and 4 days after treatment[7]
4. Diet
- No strong evidence supports specific dietary interventions for VVC[8]
- Poorly controlled diabetes is a recognized risk factor — glycemic optimization may reduce recurrence[4]
- Probiotics — no evidence supports their use for treatment or prevention of VVC[8]
- General advice: adequate hydration, avoidance of excessive refined sugars in diabetic patients
5. Review of Systems
- GU: Dysuria (external vs. internal — external suggests vulvitis), vaginal discharge character, dyspareunia, vaginal odor
- GYN: Menstrual cycle timing, pregnancy status, contraceptive use, last Pap smear
- Endocrine: Polyuria/polydipsia (undiagnosed diabetes), weight changes
- Immune: HIV risk factors, immunosuppressive medications, recurrent infections
- Dermatologic: Vulvar skin changes, rashes elsewhere (psoriasis, lichen sclerosus)
- GI: Abdominal/pelvic pain (to rule out PID or other pathology)
6. Collateral History and Family History
- Prior episodes and treatments used (OTC vs. prescription, response)
- Sexual history: new partners, partner symptoms (balanitis)
- Vaginal hygiene practices: douching, scented products (can alter vaginal flora)[6]
- Family history of diabetes or autoimmune conditions
- HIV status and CD4 count if applicable[7]
7. Risk Factors
- Recent antibiotic use (most common modifiable risk factor)[4]
- Hormonal factors: Pregnancy, high-estrogen OCPs, hormone replacement therapy[4]
- Uncontrolled diabetes mellitus[3-4]
- Immunosuppression: HIV (especially CD4 <200), corticosteroids, chemotherapy[7]
- Genetic predisposition — emerging evidence for host immune/genetic factors in RVVC[4]
- Vaginal microbiome disruption — douching, intravaginal products[6]
- Obesity and increased moisture/occlusion in the vulvar area
8. Differential Diagnosis
- Bacterial vaginosis — thin, homogenous discharge; fishy odor; pH >4.5; clue cells on wet mount[5][10]
- Trichomoniasis — frothy green/yellow discharge; strawberry cervix; motile trichomonads; pH >4.5[5][10]
- Contact/irritant dermatitis — exposure to soaps, detergents, spermicides; no infectious organisms on testing[2][11]
- Atrophic vaginitis — postmenopausal; thin, dry mucosa; pale epithelium[11]
- Desquamative inflammatory vaginitis — purulent discharge, diffuse erythema, parabasal cells on wet mount[11]
- Herpes simplex vulvitis — vesicles/ulcers, pain predominant over itch
- Lichen sclerosus / lichen planus — chronic vulvar changes, architectural distortion
- Cervicitis (chlamydia, gonorrhea) — mucopurulent cervical discharge, WBCs without yeast or trichomonads[6]
9. Past Medical History
- Prior VVC episodes and frequency (classify as uncomplicated vs. recurrent)
- Diabetes mellitus (type and control)
- HIV/immunocompromised status
- Pregnancy history
- Prior gynecologic surgeries
- Chronic skin conditions (eczema, psoriasis — may mimic or coexist)
- Medication history including recent antibiotics, steroids, immunosuppressants
10. Physical Exam
- Vitals: Fever suggests alternative/concurrent diagnosis (PID)
- External genitalia: Vulvar erythema, edema, excoriations, fissures, satellite lesions[3]
- Speculum exam: White, thick, curd-like discharge adherent to vaginal walls; erythematous vaginal mucosa[3][5]
- Bimanual exam: Should be non-tender; cervical motion tenderness or adnexal tenderness → consider PID[5]
- Assess for: Ulcers (HSV), vesicles, vulvar skin changes (lichen sclerosus/planus), frothy discharge (trichomoniasis)
11. Lab Studies
- Vaginal pH: Typically normal (4.0–4.5) in VVC; elevated pH suggests BV or trichomoniasis[3][6]
- Wet mount with saline and 10% KOH: Visualization of pseudohyphae or budding yeast on KOH prep is diagnostic[3][6]
- Vaginal yeast culture: Gold standard, especially for recurrent or treatment-refractory cases — allows species identification[2][8]
- NAAT/PCR panels: Multiplex vaginal panels (BV/VVC/TV) increasingly available; high sensitivity and specificity[8][12]
- Whiff test: Negative in VVC (positive = fishy odor → BV)
- Consider: Glucose/HbA1c if recurrent VVC and diabetes not yet evaluated; HIV testing if risk factors present[7]
12. Imaging
- Not indicated for uncomplicated VVC
- Pelvic ultrasound only if concern for tubo-ovarian abscess, ectopic pregnancy, or adnexal pathology based on exam findings
13. Special Tests
- Point-of-care microscopy (saline wet mount + KOH prep) — sensitivity ~50% compared to culture; specificity is high when positive[6][12]
- Vaginal culture — recommended for recurrent VVC, treatment failure, or suspected non-albicans species[2][8]
- Antifungal susceptibility testing — indicated for patients with persistent positive cultures despite maintenance therapy[6]
- Multiplex NAAT panels — useful when microscopy is unavailable or inconclusive[12]
14. ECG
- Not applicable for VVC
- No ECG indications unless concurrent systemic illness warrants evaluation
15. Assessment
Classification is key to management
- Uncomplicated VVC (~90% of cases): Sporadic/infrequent, mild-to-moderate symptoms, likely C. albicans, immunocompetent host
- Complicated VVC (~10%): Severe symptoms, recurrent (≥4 episodes/year), non-albicans species, or immunocompromised/diabetic/pregnant patient
- Typical presentation: premenstrual pruritus with thick white discharge and vulvar erythema in a reproductive-age woman, often following antibiotic use. Atypical presentations (minimal discharge, predominant dysuria, chronic vulvar irritation) should prompt broader differential evaluation.[3][11]
16. Treatment Plan
Uncomplicated VVC
- Fluconazole 150 mg PO × 1 (most convenient; >90% cure rate)
- OR topical azole (clotrimazole 1% cream × 7 days, miconazole 200 mg suppository × 3 days, etc.)
- Oral and topical routes are equally effective[1][13]
Severe Acute VVC
- Fluconazole 150 mg PO every 72 hours × 2–3 doses
Recurrent VVC
- Induction: 10–14 days of topical azole or fluconazole 150 mg PO on days 1, 4, and 7
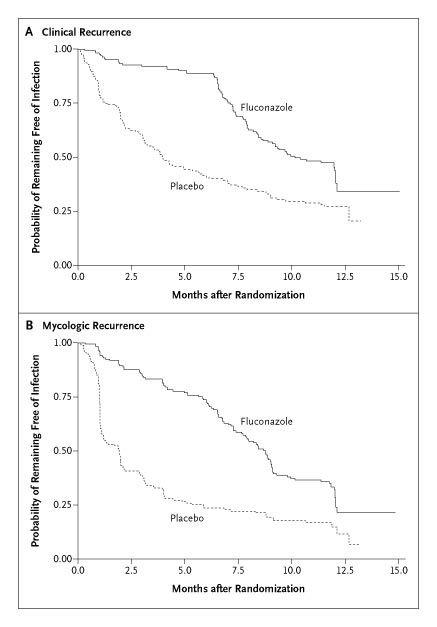
- Maintenance: Fluconazole 150 mg PO weekly × 6 months (controls >90% of episodes; ~40–50% recurrence after cessation)
- Alternatives: Oteseconazole or ibrexafungerp for eligible patients[7][9]
- The following Kaplan-Meier analysis from the landmark Sobel et al. NEJM trial demonstrates the efficacy of weekly fluconazole maintenance in preventing recurrence during the 6-month treatment phase, with subsequent relapse after discontinuation:
- View full figure Figure 1. Kaplan–Meier Analysis of the Time to Recurrence of Vulvovaginal Candidiasis among Patients Randomly Assigned to Fluconazole Prophylaxis or Placebo. Maintenance Fluconazole Therapy for Recurrent Vulvovaginal Candidiasis. N Engl J Med. August 25, 2004.
Non-albicans VVC (C. glabrata)
- Intravaginal boric acid 600 mg daily × 14 days
- Nystatin suppositories 100,000 units daily × 14 days
- Topical flucytosine 17% cream ± amphotericin B 3% cream × 14 days
- Pregnancy: Topical azoles only (7-day course preferred); avoid oral fluconazole[8]
17. Disposition
- Discharge home: The vast majority of VVC cases — uncomplicated VVC is managed entirely outpatient[1-2]
- Observation/admission: Not typically required; consider only if systemic illness, concern for PID/TOA, or severe immunocompromise with systemic candidiasis
Specialist consultation triggers
- Recurrent VVC unresponsive to maintenance fluconazole[2][6]
- Suspected azole-resistant species
- Complicated VVC in immunocompromised patients
- Diagnostic uncertainty after appropriate workup
18. Follow Up / Return Precautions
- Uncomplicated VVC: Routine follow-up not necessary if symptoms resolve[1]
- Recurrent VVC: Follow-up in 1–2 weeks after induction to confirm clinical/mycologic response; periodic monitoring during 6-month maintenance[2-3]
Return precautions — advise patients to return if
- Symptoms do not improve within 3–5 days of treatment
- Symptoms worsen or new symptoms develop (fever, pelvic pain, abnormal bleeding)
- Recurrence within 2 months of treatment
Patient counseling
- Avoid douching and scented vulvar products[6]
- Complete full course of prescribed therapy
- OTC antifungals are appropriate only for patients with prior confirmed VVC who recognize recurrent symptoms; self-diagnosis is inaccurate ~50% of the time[6]
- Expected recovery: symptom improvement within 2–3 days, full resolution within 7 days for uncomplicated cases
References
1. Oral vs. Intravaginal Antifungal Treatments for Uncomplicated Vulvovaginal Candidiasis. — Reedy-Cooper A, Ramirez S, Thomas S. American Family Physician. 2022.
2. Vaginitis in Nonpregnant Patients: ACOG Practice Bulletin, Number 215. — Committee on Practice Bulletins—Gynecology Obstetrics and Gynecology. 2020.
3. Clinical Practice Guideline for the Management of Candidiasis: 2016 Update by the Infectious Diseases Society of America. — Pappas PG, Kauffman CA, Andes DR, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2016.
4. State-of-the-Art Review: Managing Vulvovaginal Candidiasis. — Rautemaa-Richardson R, Sobel JD, Stone N, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2026.
5. Vaginitis: Diagnosis and Treatment. — Geer K, Klega A. American Family Physician. 2025.
6. Sexually Transmitted Infections Treatment Guidelines, 2021. — Workowski KA, Bachmann LH, Chan PA, et al. MMWR. Recommendations and Reports : Morbidity and Mortality Weekly Report. Recommendations and Reports. 2021.
7. Guidelines for the Prevention and Treatment of Opportunistic Infections in Adults and Adolescents With HIV. — Constance Benson, John Brooks, Shireesha Dhanireddy, et al Infectious Diseases Society of America; Office of AIDS Research Advisory Council (2025). 2025.
8. Vulvovaginal Candidiasis: A Review of the Evidence for the 2021 Centers for Disease Control and Prevention of Sexually Transmitted Infections Treatment Guidelines. — Nyirjesy P, Brookhart C, Lazenby G, Schwebke J, Sobel JD. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2022.
9. FDA Orange Book. — FDA Orange Book. 2026.
10. Vaginitis: Diagnosis and Treatment. — Paladine HL, Desai UA. American Family Physician. 2018.
11. Noncandidal Vaginitis: A Comprehensive Approach to Diagnosis and Management. — Neal CM, Kus LH, Eckert LO, Peipert JF. American Journal of Obstetrics and Gynecology. 2020.
12. Guide to Utilization of the Microbiology Laboratory for Diagnosis of Infectious Diseases: 2024 Update by the Infectious Diseases Society of America (IDSA) and the American Society for Microbiology (ASM). — Miller JM, Binnicker MJ, Campbell S, et al. Clinical Infectious Diseases : An Official Publication of the Infectious Diseases Society of America. 2024.
13. Treatment of Uncomplicated Vulvovaginal Candidiasis: Topical or Oral Drugs? Single-Day or Multiple-Day Therapy? A Network Meta-Analysis of Randomized Trials. — Gardella B, Dominoni M, Cassani C, Francesca Pasquali M, Spinillo A. American Journal of Obstetrics and Gynecology. 2025.
14. Maintenance Fluconazole Therapy for Recurrent Vulvovaginal Candidiasis. — Sobel JD, Wiesenfeld HC, Martens M, et al. The New England Journal of Medicine. 2004.